
Abstract
Background:
Group prenatal care is a promising strategy to improve perinatal outcomes. Research in larger more diverse populations with attention to adherence is needed to inform clinical practice recommendations. We examined the impact of group prenatal care on preterm birth and low birth weight in a large metropolitan hospital, accounting for patient adherence, over an 8.5-year period.
Materials and Methods:
We analyzed data from 9,348 pregnant women with a live, singleton birth who received group (CenteringPregnancy or Expect With Me) or individual prenatal care at Vanderbilt University Medical Center from January 2009 through June 2016. Propensity scores were used for matching based on year of delivery, age, race, pregnancy risk, and adequacy of care. The propensity score matched sample included 1,384 group and 5,055 individual prenatal care patients (total = 6,439 women). Preterm birth (<37 weeks gestation) and low birth weight (<2,500 g) were obtained from systematic medical review. Risks were estimated using Poisson regression.
Results:
Controlling for individual visits, receiving group prenatal care resulted in significantly lower risk of having a preterm birth (Rate ratio [RR] 0.63, 95% confidence interval [CI] 0.49–0.81) and low birth weight baby (RR 0.62, 95% CI 0.47–0.81), compared to receiving individual care only. Women with ≥5 group prenatal care visits experienced even greater benefits: 68% (RR = 0.32; 95% CI 0.22–0.45) and 66% (RR = 0.34; 95% CI 0.23–0.50) risk reduction in preterm birth and low birth weight, respectively.
Conclusions:
Participation in group prenatal care may improve birth outcomes. Efforts to promote adoption and sustainability of group prenatal care by health systems may be warranted.
Introduction
N
Limitations of previous studies include the use of clinical sites naive to group prenatal care and lack of attention to patient adherence. Initial adoption challenges may complicate an evaluation of comparative effectiveness. Attendance at more group visits is associated with better perinatal outcomes, 4 but group prenatal care is routinely complemented by individual visits (e.g., missed appointments and issues requiring private examinations). 13 Barriers to patient adherence may include scheduling conflicts, lack of transportation or child care, or privacy concerns. 14,15 Once group session dates and times are set, they typically cannot be changed, which may be problematic for women with limited control over their daily schedules. Studies involving larger more diverse samples from established implementation sites, with attention to adherence, are needed to inform clinical practice recommendations.
We assessed the impact of two group prenatal care programs implemented successively over a period of 8.5 years in a large metropolitan hospital that serves a diverse population. The specific aim of the study was to compare risk of preterm birth and low birth weight for pregnant women who received group prenatal care to a matched comparison group of women who received individual care only, accounting for patient adherence.
Materials and Methods
To meet study objectives, we conducted a retrospective matched cohort study of 9,348 women receiving group or individual prenatal care only at a university-based health center from January 2009 through June 2016. To reduce bias in estimating treatment effects, propensity score matching was conducted comparing women with the same or similar year of delivery, age, race, pregnancy risk, and adequacy of care. This study was approved by Institutional Review Boards at Vanderbilt and Yale Universities.
Participants
Pregnant women with a live singleton birth who received prenatal care at Vanderbilt University Medical Center (One Hundred Oaks Clinic, Nashville, TN) between January 2009 and June 2016 were included in this study. Deidentified data were extracted from billing, scheduling, and medical records. Maternal and infant records were linked via unique identifiers. Women were categorized as having received group prenatal care if they attended one or more group prenatal care visits. All women who received group prenatal care also received one or more individual care visits: upon intake; when group appointments were missed; or if individual appointments were deemed clinically necessary. To avoid within-person correlation, we included only the first birth that occurred during the study period for each woman. Following previous studies, women with a prior preterm birth or who entered prenatal care after 24-weeks gestation were excluded. 3,4 Excluding women with prior preterm births enabled us to examine the impact of group prenatal care on preterm birth and low birth weight among women who might otherwise have no known risk factors. To be eligible to receive either model of group prenatal care, women must have their first prenatal care visit before 24-weeks gestation.
Intervention
Two models of group prenatal care, CenteringPregnancy and Expect With Me, were implemented sequentially. Described in detail elsewhere, 2,16 each model has a unique curriculum; however, both follow guidelines from the American Congress of Obstetricians and Gynecologists for recommended content and schedule of prenatal care. For both models, groups are led by a licensed healthcare provider (obstetrician or midwife) and assistant. At Vanderbilt University Medical Center, group prenatal care sessions are led by certified nurse midwives and medical faculty. Residents and medical students participate as co-facilitators, when possible, during their rotations on service. Following individual intake, all prenatal care occurs within the group setting, except for visits requiring private consultation (e.g., late-pregnancy cervical assessments). Groups include 8–12 women of similar gestational age. Depending on gestational age at enrollment and delivery, women participate in up to 10 group sessions of 120 minutes each. During group care, providers conduct individual clinical assessments (e.g., fundal height and heart rate monitoring), women practice self-care skills (e.g., weighing themselves and taking own blood pressure), and group members participate in facilitated discussions on healthy pregnancy, birth, and parenting. Expect With Me patients additionally have access to a novel information technology platform designed to improve patient engagement and support, improve health behaviors and decision-making skills, connect providers and patients, and enhance health service delivery. 16 Vanderbilt University Medical Center transitioned from using CenteringPregnancy to Expect With Me in 2013. There were no other changes to the prenatal care delivery practice pattern during the study period.
The cohorts of women receiving CenteringPregnancy and Expect With Me group prenatal care were combined as they share the same structure and underlying philosophy. The timing of sessions and core content of prenatal care are the same. Each model has a unique curriculum. However, previous research has demonstrated that fidelity to the process of group prenatal care (i.e., patient engagement and facilitative leadership), rather than fidelity to session content, may drive the observed reductions in preterm birth and other adverse birth outcomes. 17 Expect With Me includes a technology platform that serves to facilitate model implementation and reinforces the social relationships and learning that happen in groups.
Measures
Primary outcomes were preterm birth (<37 weeks gestation) and low birth weight (infants <2,500 g). Factors used in the propensity score matching were year of birth to control for historical variation, as well as mother's age (<18, 18–34, and ≥35 years), race (black vs. other), pregnancy risk (classified based on number of maternal-fetal medicine visits attended (0–1 = low risk, ≥2 = high risk)), and adequacy of care (classified as adequate, intermediate, or inadequate using the Revised-Graduated Prenatal Care Utilization Index). 18 Our clinical experience is that sociodemographic characteristics and presence of comorbid conditions may contribute to self-selection or provider referral bias for group prenatal care. A pregnant woman seeking prenatal care at Vanderbilt University Medical Center is likely to be seen by a maternal fetal medicine specialist two or more times if she is deemed to have a complex maternal medical condition, obstetric complication, or fetal condition that requires intermittent assessment and management. These conditions can include, but are not limited to, anticipated birth defects, multiple gestations, preexisting diabetes, heart disease, hypertension, infection diseases or kidney diseases, or history of preterm delivery. A minimum of two maternal-fetal medicine visits was selected as a proxy for higher pregnancy risk since there are instances where women may receive a referral but the condition that prompted the initial visit does not require ongoing specialty care. 19 Adequacy of care, which encompasses both the timing of the initial and total number of prenatal care visits, was included to ensure that comparisons between the study groups reflected the type of care received as opposed to amount. 18 Number of individual prenatal care visits attended was included in adjusted models (categorized as 0–1, 2–9, and 10+ visits).
Propensity score matching
Randomization was not possible in this observational study of routine clinical practice; therefore, propensity score matching was conducted to reduce bias in estimating treatment effects. 20 Propensity score matching provides a rigorous approach for comparing treatment groups, matching on observable characteristics believed to be related to the exposure of interest or that which are confounders. 21,22 Propensity score matching enables creation of study groups that are similar and, in turn, more accurate assessment of the relationship between treatment and outcome than direct comparisons of two potentially disparate groups. This method has been used recently in studies of maternal and child health outcomes (e.g., use of antidepressants in pregnancy 23 and screening by echocardiography among extremely preterm infants 24 ).
We generated a greedy-matched sample of women who received any group prenatal care versus individual prenatal care only using propensity scores based on year of delivery, age, race, pregnancy risk, and adequacy of care. In greedy matching, a group prenatal care subject is first selected at random. An individual prenatal care subject whose propensity score is closest to that of this randomly selected group prenatal care subject is then chosen as a match. Each group prenatal care patient was matched with up to four individual care patients using a caliper of 0.25 standard deviations of the logit of the propensity score, without replacement. We evaluated whether variables used to create propensity scores were balanced postmatching, based on standardized difference <0.10. 20
Statistical analyses
Women who delivered preterm were eligible to attend fewer group/individual care sessions than those who reached or exceeded expected due dates. In addition, women who joined the study at later gestational ages were more likely to receive fewer group/individual care sessions compared to women who joined the study at earlier gestational ages. To account for this variation in duration of prenatal care, we used Poisson regression models to compare rates of preterm birth and low birth weight among group care patients versus those who did not receive any group care. Poisson regression models are generalized linear models that account for the observation time per person (in this case duration of prenatal care in days from first visit to delivery), thus allowing estimation of incidence rate ratios (RRs). 25 The regression models were adjusted for number of individual care visits (i.e., we included a variable that classified the women according to the number of individual visits they attended). Following previous research, 4 we conducted a post hoc subgroup analyses to evaluate the impact of receiving five or more group care visits versus individual care only, as well as five or more group versus five or more individual care visits. Finally, we conducted a post hoc stratified analysis to compare the birth outcomes for women who received Expect With Me versus CenteringPregnancy versus individual care only, using the same propensity score matching and control criteria to ensure that the cohorts in these two types of group prenatal care were combined appropriately.
Results
A total of 13,892 women with a live delivery at Vanderbilt University Medical Center during the study period were eligible to receive group prenatal care (i.e., received any prenatal care at the One Hundred Oaks Clinic) (Fig. 1). Approximately one-third (32%; n = 4,454) were excluded based on the following criteria: entered prenatal care >24 weeks gestation, prior preterm birth, and/or missing data to determine prior preterm birth history. Women missing data on prior preterm birth were significantly more likely to have received individual prenatal care than those with a known history (p < 0.05). There were no other differences between those included and excluded from these analyses. Only the first birth that occurred during the study period for each woman was included (n = 1,577 subsequent births excluded). The full sample included 9,348 women, of whom 85% (n = 7,963) received individual prenatal care exclusively; 15% (n = 1,385) received at least one group prenatal care visit.
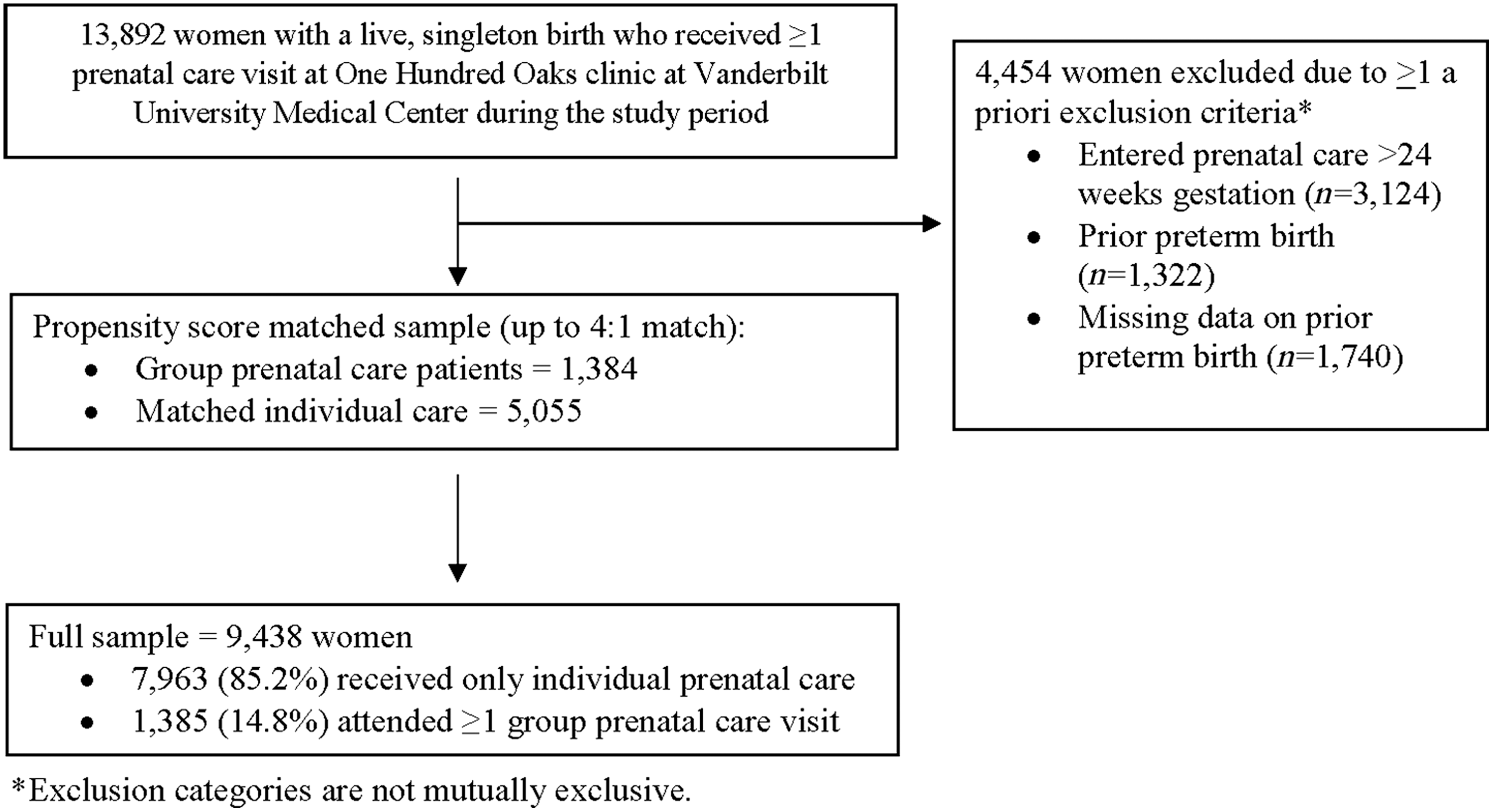
Flowchart for analytic sample based on inclusion/exclusion criteria.
The propensity score matched sample was effective at creating equivalent intervention groups, in terms of the factors used in the matching: year of delivery, age, race, pregnancy risk, and adequacy of care (Table 1). The final analytic sample included 5,055 exclusive individual prenatal care patients and 1,384 group prenatal care patients. Group prenatal care patients attended an average of 6.3 (standard deviation [SD] = 2.6) group sessions and 3.4 (SD = 2.5) individual visits. Individual care only patients had a mean of 9.1 (SD = 2.4) prenatal visits.
Full and Propensity Score Matched Sample Characteristics [% (N)]
Difference between proportion1 (group care) and proportion2 (individual care) divided by the standard deviation of the sampling distribution of proportion1–proportion2; imbalance defined as absolute value >0.10. 23
Through June, 2016.
The overall cumulative incidence of preterm birth and low birth weight among the propensity matched sample was 7.4% and 6.7%, respectively. Table 2 presents results of the Poisson regression models comparing rates of preterm birth and low birth weight for group prenatal care versus those with individual care only. Adjusting for number of individual visits, group prenatal care patients had significantly lower risk of having a preterm (RR 0.63, 95% confidence interval [CI] 0.49–0.81) or low birth weight (RR 0.62, 95% CI 0.47–0.81) baby than those who received no group prenatal care. Adjusting for the number of individual visits, the rates of preterm birth were 1.75% and 8.56%, and the rates of low birth weight were 1.21% and 7.17% for group prenatal care and individual care only, respectively.
Results of Poisson Regression Models Comparing Birth Outcomes for Group Versus Individual Prenatal Care Patients Among the Propensity Score Matched Sample
Adjusted for number of individual visits. N = 6,771 for preterm birth; N = 6,767 for low birth weight, due to listwise deletion.
p < 0.001.
Approximately, 77.6% women participating in group care attended at least 50% of recommended group prenatal care visits (5 out of 10). Post hoc subgroup analyses demonstrate that women who attended at least 50% of recommended group visits experienced even greater risk reductions in adverse birth outcomes. Compared to individual care only patients, risk of preterm birth and low birth weight among women who attended five or more group prenatal care sessions decreased by 68% (RR = 0.32; 95% CI 0.22–0.45) and 66% (RR = 0.34; 95% CI 0.23–0.50), respectively. In addition, we observed a lower risk of preterm birth and low birth weight among women who attended five or more group care sessions compared to women who attended five or more individual care only visits, (RR = 0.55; 95% CI 0.41–0.72) and (RR = 0.52; 95% CI 0.38–0.72), respectively.
Finally, the results of post hoc analyses stratified by type of group prenatal care revealed that, compared to individual care, women who received Expect With Me experienced a 49% (RR = 0.51; 95% CI 0.33–0.76) reduction and those who received CenteringPregnancy a 32% (RR = 0.68; 95% CI 0.52–0.88) reduction in risk of preterm birth. Likewise, Expect With Me was associated with a 51% (RR = 0.49; 95% CI 0.30–0.79) reduction and CenteringPregnancy a 33% (RR = 0.67; 95% CI 0.51–0.89) reduction in low birth weight. Differences in the magnitude of these reductions should be interpreted with caution, as this study was not designed to compare group prenatal care models to one another. Results suggest that both Expect With Me and CenteringPregnancy were associated with reduced rates of preterm birth and low birth weight.
Discussion
Among more than 9,000 pregnant women, we observed statistically and clinically meaningful risk reductions for both preterm delivery and low birth weight among women who attended any group care sessions. This study also demonstrates the importance of adherence. Specifically, attending five or more group prenatal care visits resulted in more than a two-thirds reduction in risk of having a preterm birth or low birth weight baby. Compared to women who attended five or more individual care only visits, those who attended five or more group sessions also experienced lower risk of preterm birth and low birth weight. It is possible that a minimum “dose” may be required to observe enhanced benefits of group relative to individual care, particularly if increased social support, which may take multiple meetings to establish the necessary trust to achieve, is one of the mechanisms through which the group dynamic positively influences birth outcomes. More than three-fourths of the pregnant women who started group prenatal care attended at least half of the recommended 10 group sessions.
Effect sizes observed in the current study are comparable to those reported in previous studies. 10,11 This study examined women who received prenatal care at a large clinical site over an 8.5-year period. We included one of the largest study samples to date, and women were diverse regarding medical and social risk factors. Previous studies have included women who were predominantly young, minority, and low income. In addition, prior studies, and particularly those based on an intent-to-treat analytic approach, may have diluted the effect of group prenatal care on birth outcomes depending on treatment adherence. We accounted for heterogeneity in terms of amount of group versus individual prenatal care visits women attended. Women who carry to term are eligible to access more prenatal care than women who deliver preterm simply because they are pregnant longer. To address this, we included adequacy of care, based on the Revised-Graduated Prenatal Care Utilization Index which considers gestational age at first prenatal care visit and at delivery, as one of the variables used to create the propensity scores. 18 We also used Poisson regression models to account for variation in duration of care. Therefore, we conclude that any observed effects of group prenatal care are not the result of temporal confounding.
Group prenatal care will only achieve large-scale national impact on maternal and child health outcomes to the extent that it is adopted by patients and providers. Despite Vanderbilt University Medical Center's long-standing commitment to providing group prenatal care, only 15% of eligible patients participated. Inadequate systems for recruitment and retention can contribute to low group prenatal care enrollment. 26 Other challenges may include difficulties with securing adequate space, scheduling, and staffing. 27 Transitioning health systems to provide group prenatal care requires an organizational culture that supports innovation and substantial investment in terms of clinical space and provider and support staff time. 26,27 Paradoxically, although the healthcare delivery system bears the burden of transformation to provide group care, the beneficiary of cost savings is most often the payor. Recent studies of Medicaid payment models in South Carolina have incentivized providers to deliver group prenatal care and produced significant returns on investment for all stakeholders. 5,10
We acknowledge several study limitations. As with other cohort studies, we rely on matching techniques in our analysis because assignment to group care was not randomized, the gold standard for clinical research. Billing and medical record data contained limited sociodemographic and clinical information. Data were not available for other race categories, smoking history, or medical conditions (e.g., hypertension and diabetes). We were able to use number of maternal-fetal medicine visits as a proxy for a medically high-risk pregnancy, but were limited in our ability to control for potential social risk factors. Moreover, although women with complex maternal medical conditions, obstetric complications, or fetal anomalies may be more likely to have had two or more maternal-fetal medicine visits, not all high-risk pregnancies are identified before labor and delivery and some primary care providers may be more comfortable executing a care plan for certain conditions than others who may prefer the subspecialist to continue to follow the patient. We were also not able to differentiate between spontaneous versus iatrogenic preterm births.
Although we account for heterogeneity arising from group prenatal care patients' mix of individual and group care visits, future studies should also examine patterns of individual care visits among group care patients, patient characteristics (e.g., sociodemographic factors, comorbid health conditions, stress, and anxiety) associated with supplemental individual care visits, and consequences of such visits on clinical sites' implementation of group care models. Finally, although this study includes women who received two different group prenatal care interventions, it was not designed to assess the comparative effectiveness of the two models. We believe them to be comparable, as they are both based on clinical guidelines established by the American Congress of Obstetricians and Gynecologists. Although each uses a unique curriculum, previous research suggests that it is the group process (e.g., facilitation by provider leaders and social support provided by the group of women at a similar stage of pregnancy) and not content (e.g., specific curriculum) that drives observed differences in birth outcomes. 23
Despite substantial biomedical advances and intervention efforts, preterm and low birth weight deliveries persist, with serious consequences for infant, child, and adult health. The multifaceted supportive nature of group prenatal care provides mothers with holistic care during a time of stress and change, embedding them within a social network of peers, empowering them with knowledge and skills, and increasing their access to medical care throughout the second and third trimesters of pregnancy. Group prenatal care participation may result in improved birth outcomes and patients also report higher levels of care satisfaction, 3 both important components of value-based healthcare. Health service innovations come with many implementation challenges, and more research is needed to better understand how group prenatal care may be positively influencing outcomes. Nonetheless, efforts to promote more widespread adoption and sustainability of group prenatal care, including innovative incentive strategies and enhanced reimbursement, are warranted.
Footnotes
Acknowledgments
This study was supported by a grant from UnitedHealth Foundation, with additional in-kind support from UnitedHealth Group. The authors thank Dr. Urania Magriples for her review and feedback on this article.
Author Disclosure Statement
No competing financial interests exist.