
Abstract
Background:
Inappropriate gestational weight gain (GWG) is prevalent in the United States. About 20% of women gain below Institute of Medicine (IOM) recommendations; more than 50% gain above. GWG outside of recommendations is linked to poor birth outcomes and health issues for mother and baby. Counseling by health care providers is important to encourage appropriate GWG.
Methods:
Assess patient recall of counseling regarding GWG, provider knowledge, and opinions about IOM GWG guidance, and GWG outcomes in a subset of women. Cross-sectional, with questionnaires distributed by 8 medical centers across the United States to patients. Questionnaires were distributed to providers and data on maternal body mass index (BMI) and GWG collected at seven sites.
Results:
A total of 1,157 women returned questionnaires (1,820 maximum possible). A majority at all sites reported a provider discussed their expected GWG with them. Close to half reported that a provider had discussed potential harms from inappropriate GWG. Most of the women (71.2%) considered their obstetrician to be a helpful resource for GWG advice. Most providers (87.5%) reported they were aware of IOM guidelines. As many providers disagreed (18.8%) as agreed (20.8%) that they were successful helping their patients attain appropriate GWG (58.3% were neutral). Physician self-reported confidence was associated with whether they believed they could help their patients avoid excessive GWG. The most common outcome was GWG above recommendations (51.4%). Overweight and obese women were more likely to gain above recommendations. Providers underestimated the proportion of their patients that gained below IOM recommendations (8.5% vs. 18.6%).
Conclusions:
Providers are aware of the dangers of excessive GWG and a majority of patients report receiving counseling. Providers appear more cognizant of excessive GWG and underestimate inadequate GWG. Most women are not achieving an appropriate GWG, with overweight and obese women especially likely to gain above recommendations.
Introduction
Maternal body mass index (BMI) and weight gain during pregnancy are important factors for neonatal and maternal health both immediately postpartum and well into the future. Prior work has shown that underweight women who do not gain enough weight during pregnancy are at risk for small gestational age neonates and preterm birth, 1 –4 birth outcomes that are associated with poor health later in life for the neonate. In contrast, high maternal BMI and excessive gestational weight gain (GWG) are independent risk factors for increased neonatal adiposity. 5 Excessive GWG is also a risk factor for fetal macrosomia, cesarean delivery, postpartum weight retention, 6 and future obesity of both mother and child. 7 –9 The effect appears to extend into adolescence and beyond. 10 Daughters of mothers who gained weight above the Institute of Medicine (IOM) GWG recommendations were more likely to be overweight or obese at age 40 compared with women who gained within recommendations. 11
Over the last few decades, excessive GWG has become more prevalent than inadequate GWG with almost half of U.S. pregnant women gaining weight in excess of the IOM recommendations, with overweight and obese women the most likely to gain more than the IOM recommendations. 12 –14 The proportion of women who gain below recommendations has been relatively constant at about 20%. 12
In 2009 the IOM published revised guidance for total GWG and weekly weight gain during the second and third trimesters taking into account the mother's prepregnancy BMI. 6 In 2013 the American College of Obstetricians and Gynecologists (ACOG) endorsed the 2009 IOM GWG recommendations. 15 Two of the Maternal, Infant, and Child Health (MICH) objectives listed in Healthy People 2020 are to increase the proportion of women who gain the recommended amount of weight during pregnancy (MICH 13) and to increase the proportion of women delivering a live birth who had a healthy weight before pregnancy (MICH 16.5). 16
Counseling by health care providers could be an important component to reduce the prevalence of excessive GWG, however, the effectiveness of current provider counseling practices is in question. In 2014, 1 year after ACOG endorsed the IOM recommendations for GWG, a survey of practicing ACOG Fellows found that almost one-in-five were unaware of the recommendations. 17 Physician self-confidence in their ability to counsel patients on GWG was associated with practice, with more confident physicians exhibiting greater efforts in counseling. 17 Two published studies found that about one-third of the enrolled pregnant women did not recall receiving advice regarding GWG, with overweight and obese women either more likely not to recall receiving guidance or more likely to have received advice not consistent with the IOM guidelines. 18,19 A cross-sectional study using data from four states that participated in the 2010–2011 Pregnancy Risk Assessment Monitoring System found that about 25% of women did not remember receiving GWG advice, and about 50% remembered advice not consistent with IOM recommendations. Lack of advice and advice outside of IOM recommendations were associated with inappropriate GWG. 20
The primary objectives of this study were to investigate patient recall of counseling on GWG by providers, the knowledge and attitudes of providers regarding appropriate GWG in relation to the IOM guidance with respect to maternal BMI, their self-reported confidence in their ability to counsel their patients on GWG, and GWG outcomes at multiple medical centers across the United States.
Methods
A prospective cross-sectional study was undertaken at seven clinics (Washington, District of Columbia; Honolulu, Hawaii; Minneapolis, Minnesota; Albany, New York; Cleveland, Ohio; Dallas; and Houston, Texas) where questionnaires were distributed to obstetrical patients and health care providers, and at an eighth site (Geisinger, Pennsylvania) where questionnaires were only distributed to patients. While in the waiting room, pregnant patients 18 years or older were provided with an information sheet describing voluntary consent to participate. Women were excluded if they were unwilling or unable to complete the survey. No identifiable information was collected with the survey or data sheet. The questionnaire was self-administered and available in English. Patients could receive a questionnaire at any time during pregnancy. Medical providers known to provide prenatal care at the seven sites were similarly given an anonymous questionnaire, either by internal mail or email, to fill out at the beginning of the data collection period. All surveys were sealed in envelopes and collected by individual sites. Evidence of consent to the study for patients and providers was a returned, completed survey. Patients and physicians were not compensated or rewarded for participation in the survey. Each site received approval through its Institutional Review Board.
The questionnaire given to patients included demographic questions and questions regarding the patient's current pregnancy. These pregnancy questions asked patients about their weight, opinions about the association of GWG with their health and that of their baby, as well as whether or not their medical provider discussed topics such as GWG and gestational diabetes with them. Surveys also inquired into which sources of pregnancy information were most helpful in understanding GWG. Provider questionnaires included demographic questions, questions regarding their practice profiles, and questions about their knowledge, beliefs, and practices involving weight gain during pregnancy. The questions on the provider surveys were taken from a longer questionnaire regarding GWG distributed to practicing obstetrician–gynecologists in 2014 with results published in 2017. 17
At the seven sites, a subset of the patients who participated in the survey had their maternal BMI and total GWG calculated. These calculations could not be linked to the survey data, as the questionnaires were completely anonymous; it was simply noted whether a patient had returned a survey and thus enrolled in the study. The BMI and GWG calculations were restricted to patients who gave birth to a live, term, singleton baby and for whom a reliable height, prepregnancy or first prenatal visit weight, and a weight within 10 days of delivery were recorded or could be extracted from medical records. For each such patient, her GWG was coded as below, within, or above the IOM recommendations based on maternal prepregnancy or early pregnancy BMI. 6 The number of patients with a calculated GWG was less than the number that completed a questionnaire.
After the end of data collection, surveys and other data sheets were sent to ACOG for data entry, data checking, and cleaning and then statistical analysis using a personal computer-based statistical package (IBM SPSS 24.0; IBM Corp, Armonk NY). The Chi-square or Fisher exact tests were was used to analyze categorical variables. Student t tests were used to analyze continuous variables. The Mann–Whitney U test was used to analyze ordinal variables. Missing values were excluded from analysis. P-values less than .05 were considered to be statistically significant.
Results
A total of 1,820 patient surveys were sent to the seven sites; 1,157 women returned completed questionnaires ranging from 45 to 278 at each site (Table 1). A conservative estimate of response rate is 63.5%, however, some sites did not distribute all their questionnaires, so the actual rate is likely higher. Unfortunately, we did not get a count of undistributed questionnaires. Three sites (Cleveland OH, Geisinger PA, and Washington DC) reported distributing all their patient questionnaires. The response rates for those sites were 92.7%, 91.5%, and 76.3%, respectively.
Age and Education Level of the Patients from the Eight Sites
The demographics (by self-report) of the pregnant women who participated in the study are given in Tables 1 and 2. The sites differed in patient age, educational attainment, insurance status, and race/ethnicity makeup. Specifically, the Dallas TX site had significantly younger patients who were either Hispanic or non-Hispanic African American, were less educated, and had either Medicaid or no health insurance. The patients from the Houston TX and Minneapolis MN sites were older, more educated, and most had private insurance. The women from the Geisinger PA and Minneapolis MN sites were predominantly non-Hispanic white, while the women from the Honolulu HI site were predominantly Asian. The Houston TX, Albany NY, Cleveland OH, and Washington DC sites were racially diverse (Table 2).
Race/Ethnicity and Insurance Status of the Patients from the Eight Sites
Rows for race/ethnicity will not necessarily add to 100% because the Table excludes responses of “other.”
Educational attainment and insurance status were highly associated. More than 90% of the women without a high school diploma were either on Medicaid (71.8%) or had no insurance (20.0%). Among women with a high school diploma, 64.7% were on Medicaid and 12.3% had no insurance. In contrast, 74.4% of women with a college degree and 91.0% of women with a graduate or professional degree had private insurance.
A majority of women at all sites reported that a health care provider had discussed their weight and diet (71.6%, range = 61.7%–79.7%) and the expected amount of weight they should gain during pregnancy (71.2%, range = 59.3%–83.9%). Women were less likely to report that a health care provider had discussed possible harms to the mother (51.2%, range = 42.2%–65.6%) or problems during delivery from too much weight gain (45.2%, range = 35.8%–64.8%), or the potential for harm to the baby from inadequate weight gain (46.2%, range = 36.0%–58.9%) or from too much weight gain (50.4%, range = 41.7%–67.2%).
Insurance status was associated with patient recall of discussions with a health care provider regarding these issues. A higher proportion of women with private insurance reported recalling a discussion regarding expected weight gain (76.1% compared with 69.4% and 56.3% for women with Medicaid or no insurance, respectively, Chi square = 25.5, df = 4, p < 0.001). However, a majority of women with Medicaid reported discussions regarding harms to their baby from inadequate or excessive weight gain, whereas less than half of women with private insurance or no insurance reported having discussions about these issues (Chi square = 27.2 and 16.4, df = 4, p < 0.001 and p = 0.003, respectively). Similarly, 55.8% of women with Medicaid reported discussions regarding harms to themselves from too much weight gain compared with 49.9% and 39.8% for women with private insurance or no insurance, respectively (Chi square = 22.5, df = 4, p < 0.001). Less than half of the women reported discussions regarding problems during delivery due to excessive weight gain (46.9%, 46.4%, and 34.0% for Medicaid, private insurance, and no insurance, respectively; Chi square = 14.9, df = 4, p = 0.005).
Most of the women (70.2%, range 55.6%–84.0%) reported that they considered their obstetrician to be a helpful resource for advice for GWG, with only a small proportion (2.6%) considering the advice unhelpful. However, 24.7% reported not receiving advice. Patients with private insurance or no insurance were more likely to report not receiving advice from their obstetrician (27.3% and 27.7%, respectively) compared with patients on Medicaid (18.8%; Chi square 12.8, df = 4, p = 0.012). Other sources of information reported by the women as helpful were: web sites (66.6%), family (61.1%), another health care provider besides their obstetrician (53.1%), and brochures (51.5%). Educational attainment was associated with the proportion of women who reported that family and web sites were helpful sources of information, but in opposite directions, with women with more education rating web sites higher and women with less education rating family higher (Fig. 1).
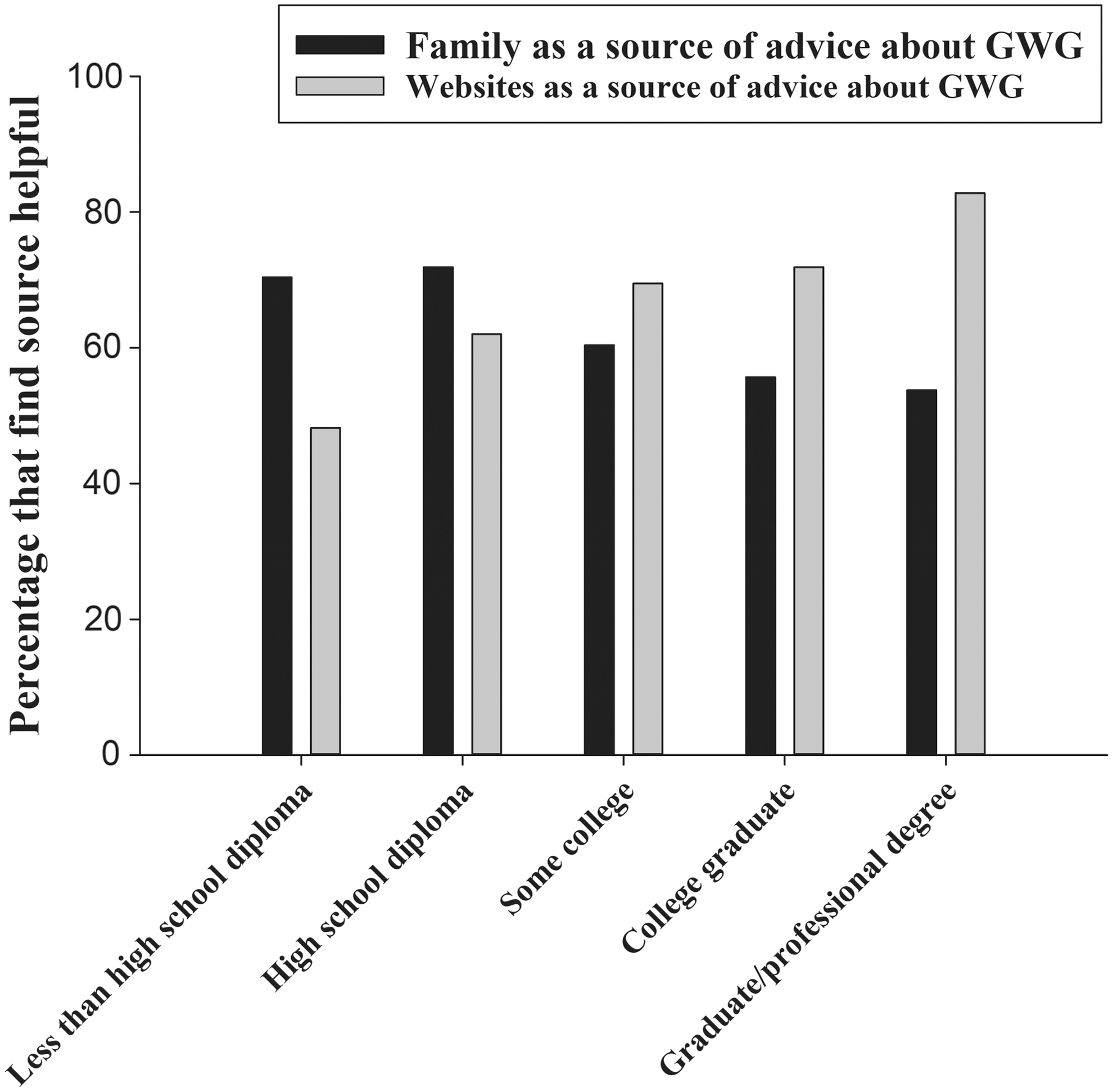
The effect of educational attainment on the perception of family and web sites as useful sources of information on gestational weight gain.
The distribution of patients by trimester was 24.8% in the first, 37.5% in the second, and 37.7% in the third trimester. The proportion of women who reported they had not received advice about GWG from their obstetrician declined with gestational age (32.6%, 22.3%, and 20.6% for first, second, and third trimester, respectively, p = 0.007), however, the proportions that reported receiving GWG advice from another health care provider did not vary by month of gestation (p = 0.267). There was no difference in the proportion of women who reported a discussion regarding weight and diet during pregnancy by trimester, however, a lower proportion of women in the first trimester reported discussions about their expected weight gain and the harms due to inappropriate weight gain (data not shown).
Patient medical record data
The mean BMI of the 451 women who were seen in the first trimester and had documented prepregnancy weight and weight gain recorded until delivery was 27.7 ± 0.4 kg/m2; mean BMI differed between sites (range = 26.1–29.5 kg/m2, F = 2.68, df = 6, p = 0.014). The most common prepregnancy BMI category at all sites was normal weight, however, on average more than 50% of women were overweight or obese (Table 3). Very few women were underweight. Gestation length did not vary across sites (mean = 276 days, range = 273–277 days), primarily because data were restricted to term births. Mean birthweight (3,326 ± 26g) also did not differ between sites. Overall mean GWG was 29.7 lbs, ranging from 27.4 lbs to 33.0 lbs, and did not significantly differ across sites (Table 3). The most common result at all seven sites was for GWG to be above the IOM recommendations (Table 4). On average, almost one of five women gained below recommendations. At every site, overweight and obese women were more likely to gain above recommendations than were women with a BMI of less than 25 kg/m2 (60.2% and 56.2%, for overweight and obese women, respectively, compared with 43.8% for normal-weight women, Chi square = 18.5, df = 6, p = 0.005).
Mean ± SEM for Gestational Weight Gain at Each Site, and the Proportions of Women Who Were Underweight, Normal Weight, Overweight, and Obese Prepregnancy
The Mean and Range Across Sites of the Proportion of Women Delivering a Singleton, Term Birth with GWG Below, Within, or Above the IOM Recommendations with Both Patient Data and Estimates Reported by the Providers Using Their Own Criteria
Provider questionnaires
A total of 96 providers from seven sites returned completed surveys. Most providers were women (79.2%). Three of the providers were nurse practitioners and 14 were nurse-midwives; the remaining providers were either residents in obstetrics and gynecology or obstetrician–gynecologists. Years in practice ranged from 1 to 35 years, however, provider responses to the questions did not significantly differ by this parameter. Most of the providers reported they were aware of the IOM guidelines (mean 87.5%, range 76.5%–100% across sites). Although there was significant variation in opinion of the IOM recommendations across the sites, of those who were aware of the IOM guidelines most (80.6%) agreed with them and none disagreed. However, about one-in-five were neutral.
The providers were asked to estimate, based on their own criteria, the proportion of pregnant patients in their practice that gained too little, an appropriate amount, or too much weight during pregnancy (Table 4). The provider estimates for the proportion of women who gained too little weight were less than the actual proportion of patients in the study who gained below IOM recommendations based on patient records for all seven sites. The providers overestimated the proportion of patients who gained an appropriate amount of weight compared with the results from the patient data. The estimates for the proportion of patients that gained too much weight were better matched to the patient data, although on average the providers' estimates were lower.
Most of the providers agreed (47.9%) or strongly agreed (45.8%) that excessive GWG is a major health concern in their practice and most disagreed (53.1%) or strongly disagreed (32.3%) that the health risks of excessive GWG are overstated. Most agreed (46.9%) or strongly agreed (32.3%) that an increasing number of their patients gain too much weight during pregnancy and almost all agreed (45.8%) or strongly agreed (46.9%) that excessive GWG is more of a problem in their practice than inadequate GWG. Most providers agreed (47.9%) or strongly agreed (42.7%) that GWG can be modified through diet and exercise, and most disagreed (60.4%) or strongly disagreed (30.2%) that GWG is beyond a woman's control.
Although more than half of providers were confident in their ability to affect the weight of their pregnant patients (57.3%), about as many disagreed that they were successful (18.8%) at helping their patients gain an appropriate amount of weight during pregnancy as agreed (20.8%; 58.3% were neutral). Provider self-reported confidence was not associated with years of practice, gender, or type of provider. Provider confidence was associated with their opinions on whether they could help their patients avoid excessive weight gain and whether their patients would follow their advice on GWG, diet, and exercise (Table 5).
The Association Between Physicians Answer to the Question: “How Confident Are You in Your Ability to Affect Your Patients' GWG?” and Their Opinions on Whether Their Patients Will Be Helped and Follow Their Advice
p < 0.001 for all questions.
Discussion
More than 7 of 10 women in this study recalled discussing their expected GWG with a health care provider and specifically considered their obstetrician to be a helpful source of information or advice for GWG. Women in the first trimester were less likely to report discussions about their expected weight gain and potential harms due to inappropriate GWG and more likely to report not receiving advice from their obstetrician. However, there was no difference by trimester in having a discussion about weight and diet and they were equally likely to report having received GWG advice from another health care provider, suggesting that early pregnancy counseling on GWG may often be done by nurses, midwives, and other providers. Our findings are similar to single-site studies, which have reported that between 76% to 87% of pregnant women recall having received advice on GWG from their health care provider. 20,21 The proportion reporting they received advice is higher than previously published reports of survey data, in which only about half of women reported receiving advice on GWG. 18,19 This may indicate that provider counseling on GWG is improving, however, the fact that almost 30% of patients in the current study reported receiving no advice on GWG remains disappointing.
Health insurance status was associated with recall by patients of discussions of expected weight gain and of problems associated with inappropriate weight gain, with women with no insurance consistently being less likely to report having such discussions. Although women with private insurance were the most likely to report having a discussion with their provider about their expected GWG, women on government-sponsored insurance were the most likely to report discussions regarding problems associated with inappropriate GWG. Educational attainment was associated with insurance status, with women having greater education being more likely to have private insurance. Our results suggest that providers may be tailoring their counseling based on socioeconomic factors (e.g., insurance status, education) with women of higher socioeconomic status being more likely to receive specific GWG advice and women of lower status to receive warnings regarding problems and health risks associated with inadequate or excessive GWG.
The results from Geisinger PA reinforce the proposed link between patient demographics and recall of counseling, as the responses of those women were consistent with their relatively high educational attainment. However, the fact that women from Geisinger were the most likely to recall warnings about inappropriate GWG suggest that institutional practice patterns are also important. Unfortunately, any differences in counseling practice at Geisinger do not appear to have resulted in better outcomes, as a 10-year examination of GWG at Geisinger found no change from 2006 to 2015, with a majority of women (52.9%) gaining above recommendations and only 25.8% gaining within recommendations. 22
The proportion of providers that were aware of the IOM guidelines (mean 87.5%) was marginally better than the proportion of practicing obstetrician–gynecologists that were aware of the recommendations in a 2014 study (81.8%), 17 and essentially the same proportion found in a more recent study of providers at single-site institution in Washington, D.C. (86%). 21 Among providers who were aware of the guidelines, a higher proportion in this study agreed with them (80.6%) than in the 2014 study (66.2%). 17 We cannot distinguish whether this difference is due to the IOM recommendations becoming better accepted by providers or simply that the providers at these institutions are more positively disposed toward them.
The proportions of women in this study who gained below, within, and above the IOM recommendations were consistent with previously published national data. 13,14 About one of five gained below recommendations and more than half gained above recommendations. This result did not match the provider estimates, specifically for gaining inadequate weight (Table 4). The provider estimate for inadequate GWG in their practice based on their own criteria was only 8.5%, on average. This value is remarkably similar to the result (7.8%) found in surveys of obstetrician–gynecologists conducted in 2012 and 2014. 17 We cannot distinguish whether this implies that providers believe the IOM inadequate GWG recommendations are too generous or if providers are less concerned over GWG below recommendations and therefore less aware of its occurrence in their practice. Most providers agreed that excessive GWG was more a problem than was inadequate GWG in their practice, and while the patient data do confirm that impression, one of five patients gaining below recommendations could still be concerning. The underestimation of inadequate GWG within their patient populations raises the concern that providers might be discounting an important health issue due to the epidemic of excessive GWG.
Consistent with previously published studies, 17 physician confidence was associated with physician belief that they could affect their patients' GWG and that patients would listen to their advice. Physician confidence has been associated with practice effort for both GWG 17 and weight gain in nonpregnant patients. 23 Unfortunately, the measured GWG outcomes of this study and others are not encouraging and suggest that any physician confidence regarding helping their patients gain an appropriate amount of weight during pregnancy may be misplaced. If provider counseling on GWG remains ineffective, this could lead to reduced efforts as confidence is lessened by an observed lack of change in outcomes.
A focus group study found that providers were concerned that their training regarding GWG was inadequate. A common reported motivation for providers to participate in the focus groups was “…to find out what other people are doing,” indicating an interest in learning new counseling methods and tools. 24 The study by Delgado et al. 21 found a disconnect between providers and patients over the utility of informational posters and brochures/pamphlets in the examination and waiting rooms, with patients more likely to report they are useful/helpful. 21 Delgado et al. suggest that given the amount of time patients likely spend in these rooms before interacting with a provider, making pamphlets/brochures available and having posters regarding GWG prominently on display might be simple methods to increase patient awareness and the ease of bringing a discussion of GWG into the prenatal visit.
The current study is unique in that it sampled patients and health care providers simultaneously to compare their perceptions. While our study has a large patient and health care provider sample size across a diverse geographic area of the United States, our study is not without limitations. Almost 40% of surveys were not returned. No information is available on this missing proportion of women, and how these individuals may have differed from our study subjects cannot be determined. Individuals who are willing to participate in surveys may differ from those who are not willing to respond. The data from the provider and patient surveys are from self-report, and thus subject to imperfect recall and recall bias.
Conclusions
Health care providers are aware of the risks of excessive GWG and are counseling patients, however, actual clinical practice success is lacking. A majority of patients continue to have inappropriate GWG. Providers also appear more cognizant of the hazards of excessive GWG and underestimate the proportion that may have inadequate GWG. Providing effective tools for physicians to manage GWG in their patients could increase practice effort by increasing physician confidence in a potentially self-reinforcing cycle that would be beneficial for public health.
Footnotes
Acknowledgments
Many people assisted in this research. The authors would like to specifically thank Dr. Renee Samelson for her help in supporting the research at Albany Medical Center Obstetrics and Gynecology, Drs. Angie Jelin and Caroline McCormick for assistance with data collection at MedStar Washington Hospital Center, Ms. Sydney Stark for her assistance in chart review at MetroHealth Medical Center, Case Western Reserve University, and Ms. Heather Gray for her assistance with data collection at the University of Minnesota. The efforts of the ACOG Research Department staff were invaluable, specifically Katie Murtough and Lauren Stark for their efforts to establish the project, and Carrie Snead for her work on organizing and entering data. This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreements UA6MC19010 and UA6MC31609: Pregnancy-Related Care Research Network. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.