
Abstract
Introduction:
Little is known about how exposure to adverse childhood experiences (ACEs) and protective factors, such as resilience, influence prenatal mental and behavioral health. This study examined associations between exposure to ACEs and mental and behavioral health during pregnancy overall and among women with high versus low levels of resilience.
Materials and Methods:
Women in two Kaiser Permanente Northern California medical centers were screened for ACEs and resilience during prenatal care (∼14–23 weeks of gestation; N = 355). Multivariable logistic regression analyses examined associations between ACEs and prenatal mental and behavioral health conditions overall and for women with low (≤32) versus high (>32) resilience on the 10-item Connor-Davidson Resilience Scale.
Results:
Overall, 54% of women reported 0 ACEs, 28% 1–2 ACEs, and 18% 3+ ACEs. Relative to women with 0 ACEs, those with 1–2 ACEs had higher odds of an anxiety or depressive disorder and intimate partner violence (IPV) (odds ratios [ORs] 2.42–3.12, p < 0.05), and those with 3+ ACEs had higher odds of an anxiety or depressive disorder, depression symptoms, and IPV (ORs 3.08–4.71, p < 0.05). In stratified analyses by high (56%) and low (44%) resilience, having one or more ACEs (vs. 0 ACEs) was only associated with worse mental and behavioral health in women with low resilience.
Conclusions:
ACEs predicted mental and behavioral health conditions among pregnant women, and associations were the strongest among women with low levels of current resilience. Longitudinal research is needed to understand the causal mechanisms underlying these associations.
Introduction
Adverse childhood experiences (ACEs), defined as physical, sexual, or emotional abuse, neglect, parental loss, or family dysfunction before the age of 18, are common, 1 with approximately two-thirds of adults in the United States experiencing at least one form of ACE. 2 There is a strong dose–response relationship between exposure to ACEs and poor health outcomes, including depression, anxiety, substance use, sexually transmitted diseases, suicide attempts, and a range of chronic diseases. 2 –10 These health risks are compounded by continued stressful experiences such as intimate partner violence (IPV) in adulthood. 11 –17
Less studied but of great interest is the potential impact of ACEs on maternal health outcomes during pregnancy. A small but growing body of literature suggests that ACEs are associated with increased mental health risks during pregnancy, including higher depressive symptoms, 18 –21 anxiety, 22,23 suicidality, 24,25 and substance use. 20,26 –28 In addition, a history of ACE exposure is associated with higher rates of psychosocial difficulties 29 and IPV in pregnancy, 20,30 –32 which contribute to poor mental health outcomes. ACE-related mental and behavioral health conditions are associated with both adverse pregnancy outcomes and poorer child health, 33 –44 making it critically important to understand and reduce the risk of developing these conditions.
Although the literature on the health impacts of ACEs is robust, studies have generally omitted protective and positive factors, such as resilience, even though evidence suggests that they can influence the impact of ACEs on an individual. 45 Resilience reflects one's adaptive ability to cope with adversity, bounce back after hardship, handle unpleasant feelings, and adapt to change, 46,47 Resilience may modify the impact of ACE exposure by encouraging the use of healthy, rather than maladaptive, coping strategies, promoting self-esteem, and from internal capabilities or environmental resources. 48,49 Researchers have recently called for the inclusion of strength-based questions in studies of ACEs to better understand whether and how protective factors reduce the negative impact of ACEs on health and functioning. 45 To address this gap in knowledge, several recent studies have investigated the potential protective role of resilience in adulthood on mental and behavioral health outcomes. 50 –53 The majority of these studies have found evidence consistent with a buffering effect of resilience on the association between ACEs and psychological distress, 54,55 depression, 50,51,56 emotion dysregulation, 52 and substance use. 57 However, one study found that although resilience moderated the association between adult trauma exposure and depression, it did not moderate the association between ACEs and depression. 53
To our knowledge, only one study to date has examined whether the relationship between ACEs and mental and behavioral health during pregnancy or the postpartum period varies with resilience. Sexton et al. found that resilience moderated associations between ACEs and postpartum major depressive disorder and posttraumatic stress disorder in a sample of 214 mothers, such that risk for these conditions was the highest among women who had a combination of both ACEs and low resilience. 58 Given the deleterious consequences of mental and behavioral health conditions during pregnancy on mothers and their babies, it is critical to examine whether resilience buffers the negative impacts of ACEs on prenatal mental and behavioral health.
In this study, we examined the hypothesis that ACEs would be associated with mental and behavioral health conditions during pregnancy, including anxiety, depression, substance use, and exposure to IPV. In addition, we conducted stratified analyses for pregnant women with high versus low levels of resilience to test the hypothesis that associations between ACEs and mental and behavioral health conditions would be stronger for women with low versus high levels of resilience. To our knowledge, this is the first study to examine how ACEs and resilience combine to influence a range of mental and behavioral health outcomes during pregnancy.
Materials and Methods
Study site
Kaiser Permanente Northern California (KPNC) is a nonprofit, integrated healthcare delivery system that insures >40% of the Northern California region's commercially insured population and provides health services to >4 million members. 59 KPNC has >40,000 pregnancies each year across 15 medical centers. KPNC patients are diverse and generally representative of the northern California population. 60
From March 1, 2016 to June 30, 2016, KPNC implemented a pilot program to screen English-speaking women aged ≥18 for ACEs and resilience at their second or third prenatal visit (between 16 and 23 weeks gestation) as part of standard prenatal care in two KPNC medical centers. All patients who met the criteria described earlier were included in the study. Patients completed the ACEs and resilience questionnaires in the exam room. Clinicians reviewed the questionnaires with patients and provided resources, including an educational handout with relevant classes, support groups, books, videos and community resources, and referrals as needed. Additional details on study materials and methods have been previously published. 61
Participants
Three-hundred fifty-five English-speaking women completed the ACEs and resilience questionnaires during the 4-month study period. As previously reported, 50 women (12%) who were offered but did not complete the ACE/resilience questionnaire were not significantly different from those who did complete the questionnaire on demographics, with the exception that they were more likely to be of “Other” or “Unknown” race/ethnicity. 61 This study was approved by the KPNC Institutional Review Board.
Measures
We used a modified version of the 11-item Behavioral Risk Factor Surveillance System Questionnaire 62 to assess eight ACE exposures before age 18. The modified version was developed for easier self-administration in a healthcare setting and to be appropriate for prenatal patients. Questions are presented in Table 1. Response options were yes or no; possible ACE scores ranged from 0 to 8. Given that ACEs are highly interrelated, 63 and the cumulative impact may be stronger than the impact of individual ACEs, we categorized ACEs into three categories for this study (0, 1–2, 3+) as done in our prior work with prenatal patients. 61 For stratified analyses by resilience, we combined 1–2 and 3+ ACEs and examined 0 versus 1+ ACEs to increase power for analyses among the smaller stratified populations. Studies suggest that exposure to one or more ACEs increases health risk, suggesting this stratification is clinically relevant. 64,65 We also ran stratified analyses by resilience with 0–1 ACEs versus 2+ ACEs and the pattern of results was similar (not shown).
Prevalence of Adverse Childhood Experiences Among Pregnant Women (N = 355)
ACE, adverse childhood experience.
The 10-item Connor-Davidson Resilience Scale (CD-RISC 10) is a widely used, validated, self-reported measure of core aspects of past-month psychological resilience (e.g., ability to bounce back after hardship, handle unpleasant or painful feelings, ability to adapt to change, see the humorous side of problems) that has been used in prior research with prenatal and postpartum patients. 61,66 Answer options range from “not at all true” (0) to “true nearly all the time” (4), with higher scores indicating higher resilience, and total scores ranging from 0 to 40. 58,67 We utilized the CD-RISC 10 in this study and dichotomized resilience based on the national average (low ≤32 and high >32). 66
Diagnoses of anxiety and depressive disorders diagnosed during pregnancy were extracted from the electronic health record (EHR) by using International Classification of Diseases (ICD)-9 or ICD-10 codes (Supplementary Table S1).
Depression symptoms were based on the Patient Health Questionnaire (PHQ-9), 68 which is given during pregnancy as part of standard prenatal care (<5 none, 5–9 mild depression, 10+ moderate/severe depression). Scores range from 0 to 27 and were dichotomized into no depression (<5) versus mild, moderate, or severe depression (≥5) to include subclinical levels of depression symptoms and supplement data on depressive disorder diagnoses. Of the 355 women in this study, 63 women (17.7%) were missing a PHQ-9 score. Missing a PHQ-9 score was not significantly associated with ACEs or any demographic characteristics.
Exposure to IPV was based on either (i) an ICD-9 or ICD-10 diagnosis of IPV within 1 year of the ACEs screening (Supplementary Table S1) or (ii) self-reported exposure to IPV as part of routine prenatal screening. Women with an IPV diagnosis during pregnancy (which could include a history of IPV) or endorsement of IPV during routine screening in prenatal care were coded as positive for IPV.
KPNC pregnant women are routinely screened for prenatal alcohol and marijuana use as standard part of entry to prenatal care, via both self-report on a prenatal substance use screening questionnaire and toxicology testing (typically between 6 and 13 weeks gestation). Prenatal alcohol and marijuana use were defined as self-reported use of any amount alcohol or marijuana since pregnancy or a positive toxicology test for alcohol or cannabis as part of standard prenatal substance use screening.
Smoking status is routinely asked about and documented in the EHR for all pregnant patients. We obtained patient-reported smoking status (i.e., current, former, or never-smoker) from the EHR at the time of the ACEs screening. 69 Prior studies support the validity of EHR-based smoking status data. 70 –72
Demographic characteristics for each patient were collected from the EHR and include patient age at screening, race/ethnicity (non-Hispanic white, Asian/Pacific Islander, Black, Hispanic, Other/unknown), and neighborhood median income.
Analyses
All statistical analyses were performed in SAS 9.3. Data were assessed for normality, and non-parametric tests were used for non-normally distributed variables. Descriptive statistics were used to describe the prevalence of each ACE category (0, 1–2, 3+) and the mean number of ACEs. Demographic and mental and behavioral health conditions were calculated for the sample overall and by ACE category. Chi-square tests were used to examine whether demographic and mental and behavioral health variables differed by ACE category. A non-parametric Kruskal–Wallis test was used to test whether age differed by ACE category. Multivariable logistic regression models were run to calculate the odds of mental and behavioral health conditions during pregnancy by ACE category, adjusting for age, race, and median neighborhood income. For multivariable analyses, we combined individual types of prenatal substance use into an overall substance use variable.
Next, we calculated the prevalence of mental and behavioral health conditions by ACE category separately for women with low and high levels of resilience. Stratified multivariable logistic regression analysis was used to calculate the odds of mental and behavioral health conditions during pregnancy by ACE category, adjusting for age, race, and median neighborhood income, separately for women with high and low resilience. All stratified analyses used a dichotomous measure of ACEs (0 vs. 1+) to increase power for analyses among the smaller stratified populations.
Results
The sample of 355 women was 41.4% White, 25.9% Hispanic, 16.3% Black, 13.5% Asian/Pacific Islander, and 2.8% Other; 8.2% had a neighborhood median income <$40,000, 34.8% had a neighborhood median income of $40,000–$79,999, 44.5% had a neighborhood median income of $80,000–109,000, and 12.5% had a neighborhood median income >$110,000. The median age was 30 (Interquartile range [IQR]: 22–38).
The prevalence of each ACE is presented in Table 1. The most common ACEs reported were “losing a parent through divorce, abandonment, death or other reason” (27%), “being verbally put down by a parent or adult” (19%), and “living with someone with a drinking or drug problem” (19%). A total of 193 (54%) women reported 0 ACEs, 99 (28%) women reported 1 or 2 ACEs, and 63 (18%) women reported 3+ ACEs. Women with 0, 1–2, and 3+ ACEs were not significantly different on race/ethnicity, neighborhood median income, or age. The median and mean ACEs scores were 0 (IQR: 0–1) and 1 (standard deviation = 1.6), respectively.
The median resilience score was 34 (IQR: 29–37), and 44% had low resilience based on a score at or below the national average of 32. Women with low resilience (≤32) and high resilience (>32) did not differ significantly on mean number of ACEs, race/ethnicity, neighborhood median income, or age.
Overall, 11.6% of the sample had an anxiety disorder, 9.9% had a depressive disorder, 27.4% had any self-reported current depression symptoms, and 7.6% had an IPV diagnosis during this pregnancy or in the previous 12 months. In terms of prenatal substance use, 7.6% screened positive for any alcohol use, 9.8% screened positive for any marijuana use, 1.4% were current smokers, and 17% screened positive for any of the three substances.
Chi-square analyses indicated that ACEs were associated with an increased likelihood of having an anxiety disorder (p = 0.017), depressive disorder (p = 0.006), any depression symptoms (p = 0.003), experiencing IPV (p = 0.007), and cigarette smoking (p = 0.043) (Fig. 1). Use of alcohol, marijuana, overall substance use, and low resilience did not differ significantly by ACEs, but did follow the same trend as the other mental and behavioral health conditions.
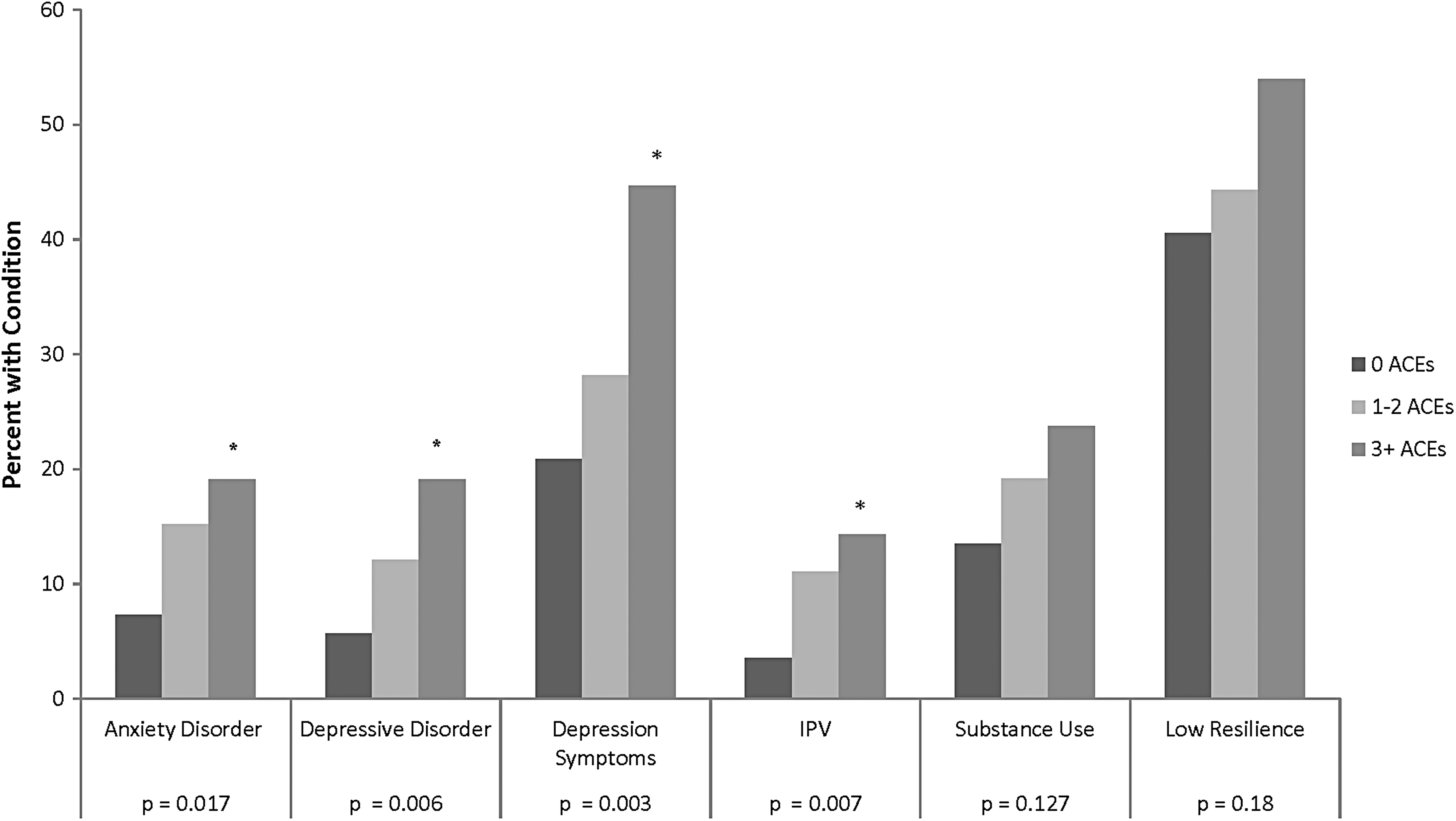
Prevalence of mental and behavioral health conditions among pregnant women by ACEs. Depressive symptoms are based on the Patient Health Questionnaire-9 survey routinely given during the first trimester of prenatal care. IPV includes a diagnosis of IPV in the EHR in the year before or during pregnancy or endorsing any of the three questions related to IPV at the beginning of prenatal care. Low resilience is based on a score below the national average (≤32) on the Connor-Davidson RISC-10 Resilience questionnaire given at the time of ACE screening. *Significant at p < 0.05. ACE, adverse childhood experience; EHR, electronic health record; IPV, intimate partner violence.
Results from multivariable models examining associations between ACEs and prenatal mental and behavioral health adjusting for age, race/ethnicity, and median neighborhood income found a graded relationship between ACEs and several mental and behavioral health outcomes (Table 2). Women with 1–2 ACEs had significantly increased odds of an anxiety disorder (OR = 2.42, 95% confidence interval [CI] = 1.09–5.41), depressive disorder (OR = 2.49, 95% CI = 1.03–6.00), and IPV (OR = 3.12, 95% CI = 1.13–8.61) relative to those with 0 ACEs. Women with 3+ ACEs had significantly increased odds of an anxiety disorder (OR = 3.08, 95% CI = 1.28–7.39), depressive disorder (OR = 3.98, 95% CI = 1.60–9.90), depressive symptoms (OR = 3.13, 95% CI = 1.58–6.17), and IPV (OR = 4.71, 95% CI = 1.59–13.95) relative to those with 0 ACEs. Increased odds for all outcomes were larger for the 3+ versus 0 ACEs comparison relative to the 1–2 ACEs versus 0 ACEs comparison, indicative of a cumulative effect of ACEs. The ACEs were not significantly associated with prenatal substance use or low resilience.
Multivariable Models of Odds of Mental and Behavioral Health Conditions by Adverse Childhood Experiences Among Pregnant Women (N = 355)
Bold values are significant at p < .05.
All analyses adjusted for age, age squared, race, and median neighborhood income. Depressive symptoms are based on the PHQ-9 survey routinely given during the first trimester of prenatal care. IPV includes a diagnosis of IPV in the EHR in the year before or during pregnancy or endorsing any of the three questions related to IPV at the beginning of prenatal care. Low resilience is based on a score below the national average (≤32) on the Connor-Davidson RISC-10 Resilience questionnaire given at the time of ACEs screening.
IPV, intimate partner violence; PHQ, Patient Health Questionnaire; OR, odds ratio; CI, confidence interval.
Stratified analyses by high and low resilience
The prevalence of each mental and behavioral health condition by dichotomous ACE category (0 vs. 1+) and resilience status is presented in Figure 2. Among the 192 women with 0 ACEs, 78 had low resilience (41%) and 114 had high resilience (59%). Among the 160 women with 1+ ACEs, 77 had low resilience (48%) and 83 had high resilience (52%). Among those with low resilience, those with 1+ versus 0 ACEs had a higher prevalence of anxiety disorders (26% vs. 9%; p = 0.01), depressive disorders (22% vs. 9%; p = 0.02), depression symptoms (46% vs. 27%; p = 0.05), and IPV (17% vs. 4%; p = 0.01), but not substance use (21% vs. 18%; p = 0.66). In contrast, among those with high resilience, having 1+ versus 0 ACEs was not significantly associated with anxiety disorders (8% vs. 6%; p = 0.54), depressive disorders (7% vs. 4%; p = 0.33), depression symptoms (23% vs. 15%; p = 0.20), or IPV (8% vs. 4%; p = 0.21), but it was associated with a higher prevalence of substance use (20% vs. 11%; p = 0.05).
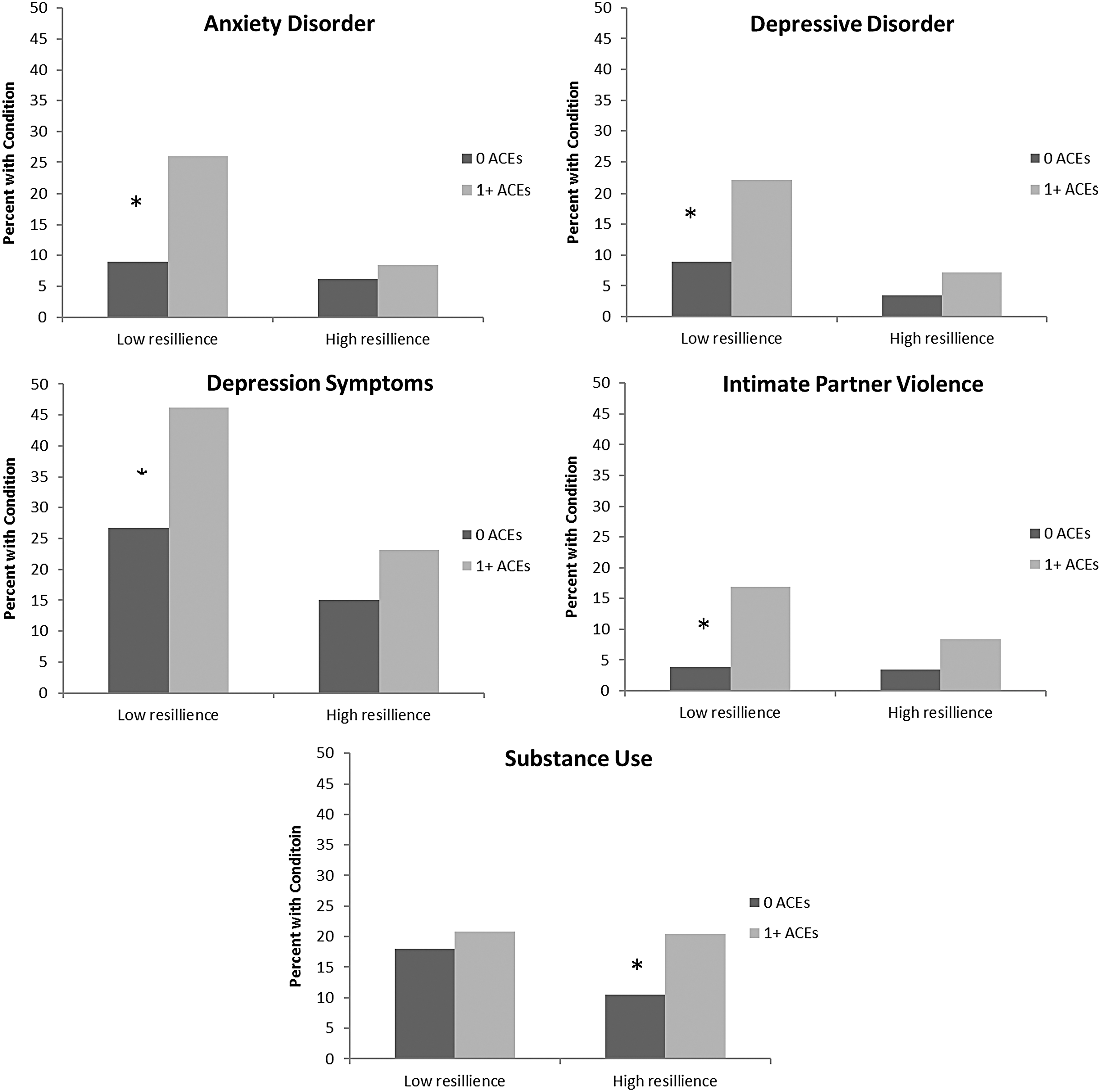
Prevalence of mental and behavioral health conditions among pregnant women by ACEs and resilience. Resilience was measured by using the Connor-Davidson Resilience Scale (CD-RISC 10), which defines low resilience as ≤32 and high resilience as >32. *Significant at p < 0.05.
Results from stratified multivariable models examining resilience-specific associations between ACEs and prenatal mental and behavioral health adjusting for age, race/ethnicity, and median neighborhood income are presented in Table 3. Among women with low resilience, those with 1+ ACEs had significantly increased odds of an anxiety disorder (OR = 4.21, 95% CI = 1.54–11.50), depressive disorder (OR = 3.09, 95% CI = 1.13–8.45), and IPV (OR = 6.50, 95% CI = 1.47–28.71) relative to those with 0 ACEs. Conversely, ACEs were not significantly associated with mental and behavioral health conditions among women with high resilience.
Multivariable Models of Odds of Mental and Behavioral Health Conditions by Adverse Childhood Experiences and Resilience Among Pregnant Women (N = 355)
Bold values are significant at p < .05.
Depressive symptoms are based on the PHQ-9 survey routinely given during the first trimester of prenatal care. IPV includes a diagnosis of IPV in the EHR in the year before or during pregnancy or endorsing any of the three questions related to IPV at the beginning of prenatal care. Low resilience is based on a score below the national average (≤32), and high resilience is based on a score greater than or equal to the national average (>32) on the Connor-Davidson RISC-10 Resilience questionnaire given at the time of ACEs screening.
Discussion
This study of the association between ACEs, resilience, and mental and behavioral health conditions in pregnancy has three key findings. First, there was a dose–response relationship between ACEs and prevalence of prenatal anxiety, depression, and exposure to IPV, consistent with previous studies. 18,19,32 Second, the associations between having any ACEs and mental and behavioral health conditions were stronger and significant only for women who reported low levels of resilience during pregnancy. Third, ACEs were not associated with use of cigarettes, alcohol, or marijuana during pregnancy in multivariable models, regardless of resilience.
Results from this study lend support to a small but growing body of literature suggesting that ACEs are associated with greater mental and behavioral health problems during pregnancy, including psychosocial difficulties, 29 depressive symptoms, 18 –21 anxiety, 22,23 and risk for IPV. 20,30,31 Findings indicate that relative to women with 0 ACEs, women with 1–2 ACEs had between 2.4- and 3.1-fold increased odds of having an anxiety disorder, depressive disorder, or IPV during pregnancy; whereas women with 3+ ACEs had between 3.1- and 4.7-fold greater odds of having an anxiety disorder, depressive disorder, depressive symptoms, or IPV during pregnancy. Interestingly, the strongest association was between ACEs and adult IPV. This novel finding in this prenatal population is consistent with the literature suggesting that victimization in childhood increases risk for experiencing IPV in adulthood. 12,15,16 The exact mediating and moderating relationships between ACEs, IPV, and mental health remain to be established. 11
These results fit well with a larger body of literature surrounding the biological mechanisms underlying the connection between ACE exposure and mental and behavioral health outcomes. 73 Prolonged stress exposure, particularly during the neurodevelopmentally vulnerable period of infancy through early childhood, can reprogram the physiological stress response system through epigenetic reprogramming 74 and is associated with volumetric differences in stress-sensitive brain regions. 75 ACE exposure is associated with molecular markers of aging and disease risk, such as telomere shortening and mitochondrial DNA copy number increases. 73,76,77 These results suggest that such molecular mechanisms may impact women in the prenatal period as well, which is particularly important given the potential for intergenerational transmission of ACEs through these biological mechanisms. 78
A particularly important contribution of this article is the finding that during pregnancy, resilience, or the adaptive ability to cope with adversity, 46 may mitigate the negative impact of ACEs on mental and behavioral health. For example, among women with high resilience, the prevalence of an anxiety disorder was similar among those with 0 (6%) and 1+ ACE (8%). However, anxiety disorders were about three times more prevalent in women with 1+ ACEs compared with women with 0 ACEs in the low resilience group (26% vs. 9%). Similar increased prevalence was found for depressive disorders, depression symptoms, and IPV for women with 1+ ACEs compared with women with 0 ACEs in the low resilience group. Although these findings are consistent with the hypothesis that resilience may moderate the impact of childhood adversity exposure, underscoring the importance of taking resilience into account when screening for adversity, we are unable to determine the direction of these associations due to the cross-sectional nature of the study. It is also possible, for example, that mental and behavioral health problems during the prenatal period contribute to lower levels of resilience.
In contrast to prior studies that have found greater risk of prenatal substance use among women with ACEs, 20,26 –28 ACEs were not significantly associated with substance use upon entry to prenatal care in multivariable models regardless of resilience. Our measures of prenatal marijuana and alcohol use were based on screening at ∼8 weeks gestation, and due to the nature of our screening, we are unable to distinguish prenatal substance use before versus after women knew they were pregnant and we could not tell whether women continued to use substances throughout pregnancy. We were also not able to determine the heaviness of substance use in pregnancy, and the lack of significant association may be due to these factors. Future studies with larger samples that include more refined measures of substance use in pregnancy (e.g., quantity, frequency, trimester of use) are needed to better understand the association of ACEs with prenatal substance use.
Mitigating the effects of ACEs on mental and behavioral health will require developing and testing interventions that foster resilience in pregnancy. Interventions such as resilience training, which includes emotional regulation training, cognitive and behavioral approaches to reframe thoughts and refocus on positive emotion, improving physical health through sleep, exercise, nutrition and relaxation, social support, and mindfulness, hold promise toward building resilience. 79 –81 Researchers have highlighted the need for services matched to key moderators, such as resilience, 82 that are responsive to intervention. 83 –85 Trauma-informed treatment approaches exist and data on their efficacy are growing. 86 For example, psychoeducational programs designed to meet pregnancy-specific needs of women with ACEs exposure may help to improve mental and behavioral health. 87 Further research is needed regarding the optimal content and timing of such programs.
Healthcare organizations have the opportunity to empower prenatal patients to cultivate their strengths and build on existing resources. This study demonstrates that ACEs and resilience screening during standard prenatal care can help clinicians identify women at risk of mental and behavioral health problems, including IPV, who may need extra support or services during pregnancy and the postpartum period. Women's health clinicians and prenatal patients should be educated about the relevance of ACEs and resilience to patients' health in pregnancy. Models integrating substance use treatment, mental health services, parenting education, family support, and other services can address these needs. 88 Incorporating ACEs and resilience screening as part of standard prenatal care is feasible and generally acceptable to patients and clinicians, provided that appropriate training and adequate mental and behavioral health referral resources are available. 61 Comprehensive and routine screening for ACEs, resilience, and mental and behavioral health conditions, in conjunction with interventions, resources, and treatment, is likely to have a strong return on investment when the health of both the mother and child is considered.
Additional longitudinal research is needed to investigate how obstetric and pediatric clinicians can promote perinatal resilience through screening, brief intervention, and broader systems-level changes, and to determine whether prenatal ACEs and resilience screening and intervention is associated with improved maternal or pediatric outcomes and reduced healthcare costs.
Strengths and limitations
To our knowledge, this is the first study to examine associations between ACEs and multiple mental and behavioral health conditions during pregnancy separately for women with high and low levels of resilience. KPNC's integrated healthcare delivery system and robust EHR allowed us to examine associations between self-reported exposure to ACEs and resilience assessed as part of standard prenatal care and mental and behavioral health conditions and IPV in an ethnically diverse population of pregnant women. However, several limitations should be noted. This study took place in two KPNC medical centers and was limited to English-speaking adult patients screened for ACEs at their second or third prenatal visit (at ∼14–23 weeks gestation), and results may not generalize to non-English-speaking patients, those without healthcare, and those who enter prenatal care late. Future research is needed to examine associations between ACEs, resilience, and mental and behavioral health conditions in non-English-speaking women and adolescent patients. Twelve percent of women chose not to complete the ACEs questionnaire and, although those women were similar on demographic characteristics to women who completed the screening, our study did not assess reasons for non-completion. Our measures of ACEs, resilience, and certain mental and behavioral health outcomes were based on self-report and are subject to self-report biases; however, it is noteworthy that past research indicates good test–retest reliability for ACEs. 9 In addition, our ACEs questions did not assess ACEs severity, frequency, age or duration of exposure, or neglect, and all ACEs were considered equal (e.g., physical abuse was equivalent to losing a parent through divorce). We used the term “sexual abuse” in our ACEs screening, but future research should avoid emotion-laden terms such as “abuse,” which may lead to underreporting, 89 and should instead use descriptive questions. In addition, due to sample size limitations, we dichotomized ACEs (0 vs. 1+) and resilience (high vs. low) in stratified analyses, which may have muted our findings. Additional studies with larger sample sizes that include more detailed information about a broader range of ACEs and more nuanced categorization of resilience are needed to better understand how childhood experiences and resilience impact mental and behavioral health. Finally, due to the cross-sectional nature of the study design, we are unable to determine causality between resilience and maternal mental and behavioral health.
Conclusions
The prenatal period has been identified as a unique window of opportunity for clinicians to impact a family's long-term health by identifying women with ACEs and providing appropriate resources. 25,61 Pregnant women have increased contact with the healthcare system and are often motivated to live healthier lifestyles to improve the health of their developing child. This study adds novel data to the literature on protective factors related to maternal mental and behavioral health during pregnancy, indicating that although ACEs are important risk factors for poorer maternal mental and behavioral health in pregnancy, resilience may help mitigate this risk. Longitudinal cohort studies with larger samples will allow for greater understanding of the causal mechanisms through which ACEs and resilience combine to influence maternal behavioral health. In addition, future studies are needed to develop strategies and interventions to increase women's sense of resilience in the prenatal period and to directly test whether improvements in resilience during pregnancy reduce the adverse impact of ACEs on prenatal mental and behavioral health.
Footnotes
Acknowledgments
This study was supported by a Grant from the Kaiser Permanente Community Benefits Program and an NIH NIDA K01 Award (DA043604). The authors thank Carla Wicks, Fiona Sinclair, Krista Kotz, Diane Lott-Garcia, Dorothy Ferguson, and Gina Smith-Anderson for their assistance with the pilot study implementation.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.