
Abstract
Background:
Data are lacking concerning possible age-specific sex-based differences in anemia in myocardial infarction (MI) patients and its association with the outcome. The aim was to assess whether these differences in anemia (on admission and at discharge) in MI patients who underwent percutaneous coronary intervention (PCI) are associated with the outcome.
Methods:
Data from 5579 MI patients (31.0% women) undergoing PCI at our institution were analyzed. Men and women in different age groups were compared regarding anemia and its association with the 30-day and long-term all-cause mortality. Data were analyzed using descriptive statistics.
Results:
Women suffered anemia more than men (37.5% vs. 26.8%; p < 0.0001). The prevalence of anemia increased rapidly with age in men but not in women. A J-shaped relationship between age and anemia was found in women. The lower the age, the greater the difference in the prevalence of anemia between the sexes. The difference in the prevalence of anemia at discharge was even more pronounced. Anemia on admission (odds ratio [OR] = 1.39; 95% confidence interval [CI] = 1.10–1.76; p = 0.005) and at discharge (OR = 2.61; 95% CI = 1.98–3.44; p < 0.0001) predicted a higher 30-day mortality. Women had a better adjusted long-term prognosis (hazard ratio [HR] = 0.78; 95% CI = 0.69–0.87; p < 0.0001) for the total population. Anemia on admission (HR = 1.43; 95% CI = 1.29–1.60; p < 0.0001) and at discharge (HR = 1.96; 95% CI = 1.23–2.21; p < 0.0001) predicted a higher long-term mortality.
Conclusion:
Younger women with MI suffer anemia more frequently than their male peers. Anemia was associated with a worse outcome. Age-specific sex-based differences in anemia help to explain the increased sex-related mortality in MI patients undergoing PCI.
Introduction
Previous observations have demonstrated higher mortality rates for women with myocardial infarction (MI) compared with men. 1,2 In addition, the differences are much more pronounced among young women compared with men. 1 –4 Despite the increased attention, this relationship remains poorly understood. 5,6 The worse outcome is mainly attributed to delays in presentation and recognition of acute coronary events, treatment differences in women, worse risk factor profiles, and greater comorbidities. 2,4,7,8 Differences in the pathophysiology of MI between the sexes, unique sex-specific biology, and disease manifestations and management may be alternative explanations for the differences in mortality. 2,4 –6 Women more often show nonobstructive coronary artery disease, and they present more often with non-ST elevation MI and less frequently with ST elevation MI compared with men. 6 Many unanswered questions remain, and explanations for the higher mortality in women remain somewhat speculative. 2 Women are also frequently underrepresented in clinical trials.
There is substantial evidence of the association between anemia and a worse outcome in patients with MI. 9 –12 Data on anemia as a sex-related risk factor are limited. 13 –15 It is not yet clear whether there are age-specific sex-based differences in anemia in MI patients. The association of these possible differences with the outcome has also not yet been evaluated. We speculated that there are age-specific sex-based differences in anemia (on admission and at discharge) in these patients. The aim was to assess whether these age-specific sex-based differences in anemia in MI patients are associated with the outcome. The 30-day and long-term all-cause mortality were observed.
Materials and Methods
This study is a single-center analysis of 5611 consecutive MI patients who were treated with percutaneous coronary intervention (PCI) at the University Medical Center Maribor between January 2007 and December 2015. Thrombolysis has not been used in our region since 2003. Patients with incomplete data (n = 32) were excluded, leaving 5579 for further analysis.
Patients were treated according to the guidelines for MI management. 16,17 The vascular access, angioplasty strategy, and concomitant medication were left to the discretion of the operator. All medical records were obtained from the hospital's information system to complete the data collection. The patients were prospectively followed-up until January 2017. Data on the dates of death were provided by the Slovenian National Cause of Death Registry. The median follow-up time was 47 months (25th–75th percentile: 21–78). The study was approved by the local ethics committee.
The patients were divided into five age groups to assess the age-specific sex-related incidence of anemia: <50, 50–59, 60–69, 70–79, and >79 years, and the incidence of anemia in each group was obtained. For calculations of mortality, we divided the patient cohorts into four age groups: <60, 60–69, 70–79, and >79 years. We decided to do so because, in the group younger than 50 years, the number of end points was very low.
Definitions
The definition of MI was based on the guidelines. 16,17 Anemia was defined as proposed by the World Health Organization: a serum hemoglobin level <130 g/L for men and <120 g/L for women. 18 Hemoglobin levels were determined on admission and after 24 hours. After the first 24 hours, hemoglobin levels were obtained at various time points, at the discretion of the treating physician. For hemoglobin at discharge, the last hemoglobin during hospitalization was used.
The Bleeding Academic Research Consortium (BARC) bleeding criteria and BARC 3a bleeding (hemoglobin drop of 30–50 g/L or any transfusion) were used. 19
Renal dysfunction on admission was defined as a glomerular filtration rate (GFR) <60 mL/kg/1.73 m2. GFR was calculated with the Modification of Diet in Renal Disease Study formula. 20 Unsuccessful PCI was defined as thrombolysis in MI flow grade 0/1 after PCI. 21
End points
The end points were the incidence of anemia in men and women in separate age groups and its association with all-cause 30-day and long-term mortality.
Statistical methods
The differences between men and women in baseline clinical, angiographic, and procedural characteristics were compared using the independent samples t-test or the Mann–Whitney U-test for continuous variables, and the chi-square test for categorical variables, as appropriate.
We counted end-point events that occurred during the follow-up period and compared their rates between the men and women. The cumulative incidence rates of the unadjusted long-term mortality were estimated by the Kaplan–Meier method and compared by the log-rank test. Multivariate logistic regression modeling was used to calculate the adjusted odds of 30-day mortality and sex.
Cox proportional hazards regression was used to compute hazard ratios (HRs) as estimates of long-term mortality. Besides sex, covariates that differed significantly between the groups were included in all regression analyses: age, hypertension, diabetes, hyperlipidemia, renal dysfunction on admission, anemia on admission (or at discharge), bivalirudin, PCI of the left main coronary artery (LMCA), PCI of the left anterior descending artery (LAD), and bleeding.
Data were analyzed with SPSS 21.0 software for Windows (IBM Corp., Armonk, NY). All p values were two-sided and values <0.05 were considered statistically significant.
Results
Descriptive data for patients
Of 5579 MI patients, 1730 (31.0%) were women. Women were, on average, almost 7 years older than the men. They suffered more often from diabetes, hypertension, renal dysfunction, and anemia. On the contrary, they had less hyperlipidemia and were less frequently treated with bivalirudin. More PCIs of the LMCA and LAD were performed in women. Bleeding was more frequent in women.
Women had a higher overall prevalence of anemia on admission compared with men. This difference was most marked in the patient groups younger than 60 years and gradually disappeared with advanced age. The difference in anemia at discharge was even greater between the sexes. The basic clinical, angiographic, and procedural characteristics are given in Table 1.
Basic Characteristics of Patients with Myocardial Infarction
Mean (standard deviation); comparison made using the t-test.
Comparison made using the chi-square test.
GPI, GPIIb-IIIa receptor inhibitors; LAD, left anterior descending artery; LCX, circumflex artery; LMCA, left main coronary artery; P2Y12, P2Y12 receptor inhibitors; PCI, percutaneous coronary intervention; RCA, right coronary artery; STEMI, ST-elevation myocardial infarction.
Prevalence of anemia according to age and sex
On admission, 1679 (30.1%) patients were anemic. Women suffered anemia more frequently than men (Table 2). The prevalence of anemia increased rapidly with age in men but not in women. There was a J-shaped relationship between age and anemia in women (Fig. 1A). The lower the age, the greater the difference in the prevalence of anemia between the sexes. The prevalence of anemia in women younger than 50 years was three times higher compared with men of the same age. Anemia was also found twice as often in women aged 50–59 years compared with their male counterparts. There was no sex difference in the group aged 60 years and older (Table 2 and Fig. 1A). The difference in anemia at discharge was even more pronounced (Table 2 and Fig. 1B). The hemoglobin levels on admission and at discharge in all age groups are given in Supplementary Table S1 (Supplementary Data are available online at
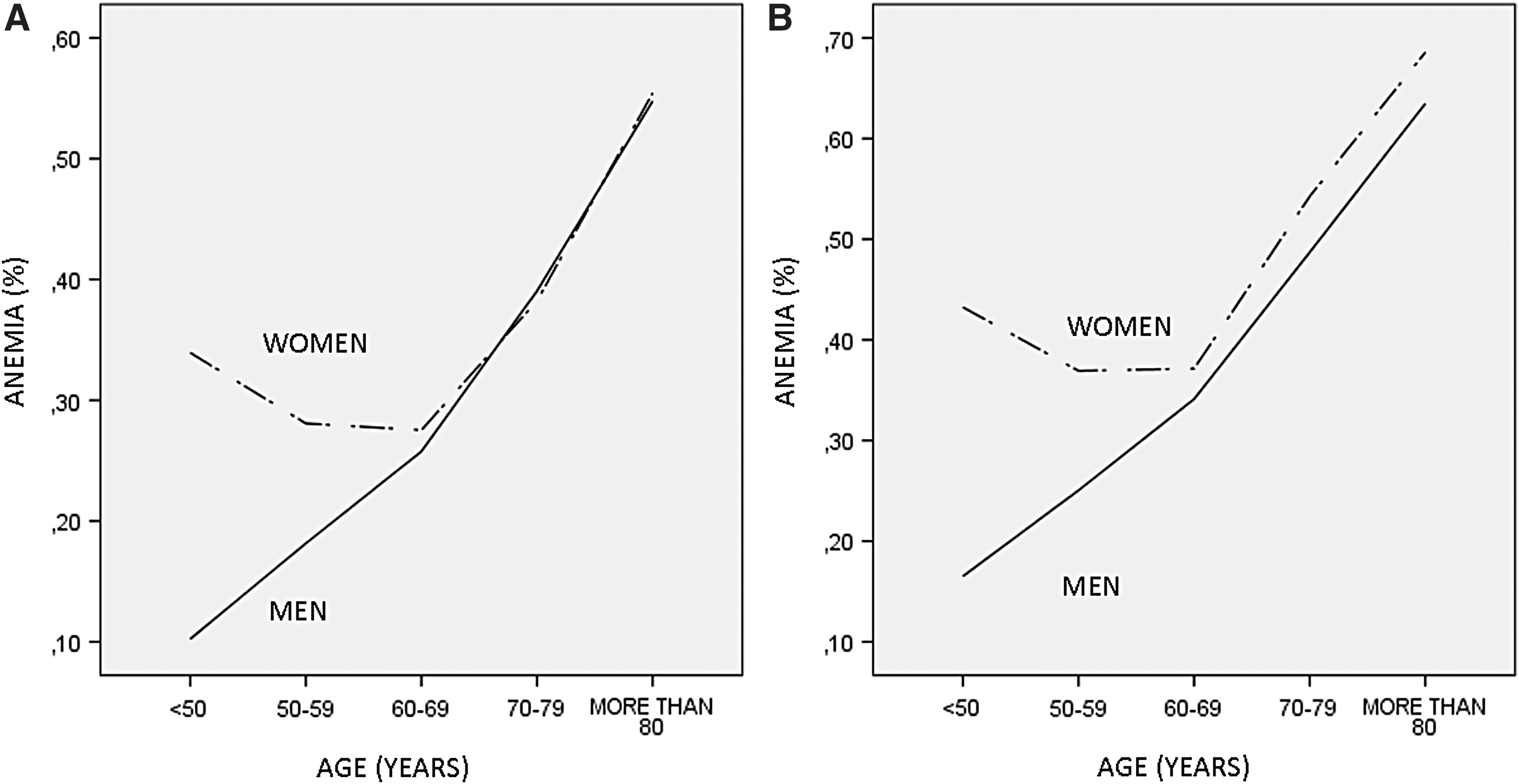
Prevalence of anemia on admission and at discharge in men and women with MI according to age. Dashed line—women; solid line—men.
Prevalence of Anemia on Admission and at Discharge in Men and Women with Myocardial Infarction According to Age
Comparison made using the chi-square test.
Mortality
Women had a significantly higher unadjusted 30-day mortality [257 men (6.7%) died vs. 168 women (9.7%); p < 0.0001]. The unadjusted women-to-men odds ratio (OR) for mortality was 1.50 (95% CI = 1.23–1.84; p < 0.0001). After adjustment for confounding factors, women's mortality was similar to men's (adjusted OR = 1.12; 95% CI = 0.89–1.43; p = 0.33). However, anemia (adjusted OR = 1.39; 95% CI = 1.10–1.76; p = 0.005) predicted a higher 30-day mortality. Other predictors were bleeding, renal dysfunction, hyperlipidemia, age, arterial hypertension, PCI of LMCA, and PCI of LAD, which are listed in Supplementary Table S2.
The long-term all-cause unadjusted mortality was higher in women [921 (23.9%) men died vs. 544 (31.40%) women; p < 0.0001] (Fig. 2A). After multivariable adjustments, women had a better prognosis (adjusted HR = 0.78; 95% CI = 0.69–0.87; p < 0.0001) for the total population (Fig. 2B). Anemia on admission and at discharge predicted a higher long-term mortality (Table 3). Other predictors were diabetes, hyperlipidemia, arterial hypertension, age, bleeding, renal dysfunction, and PCI of LAD (Supplementary Table S2).
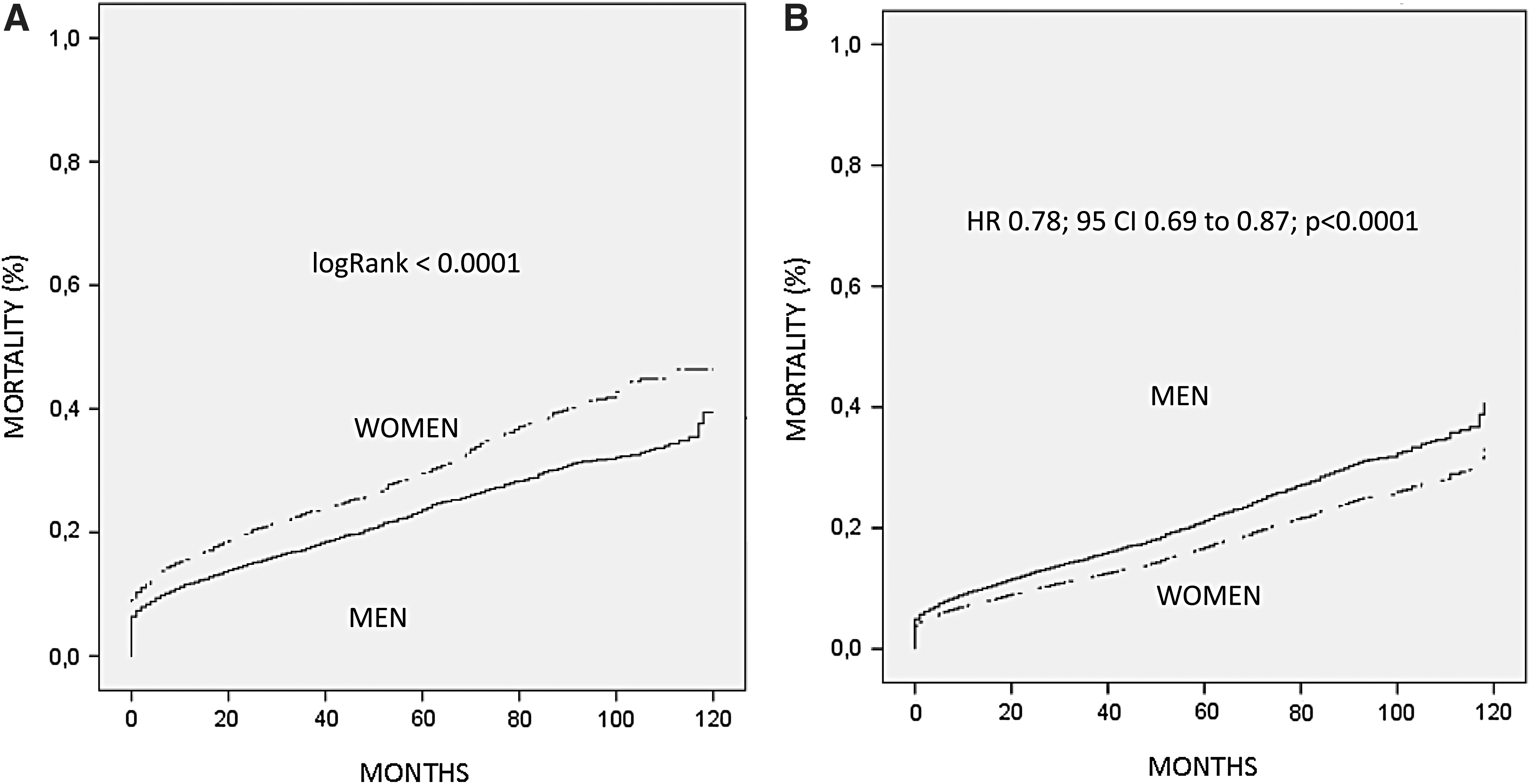
Unadjusted and adjusted long-term mortality.
Anemia as a Predictor of 30-Day and Long-Term Mortality According to Age
HR, hazard ratio; OR, odds ratio.
Anemia and mortality
We checked for any association between anemia on admission and anemia at discharge with the outcomes.
30-Day mortality
After adjustments for confounders, anemia on admission predicted 30-day mortality in the total patient cohort (adjusted OR = 1.39; 95% CI = 1.10–1.76; p = 0.005) but did not predict 30-day mortality in all age groups (Table 3).
Anemia at discharge predicted 30-day mortality in the whole patient cohort (adjusted OR = 2.61; 95% CI = 1.98–3.44; p < 0.0001) and in all age groups except for the group aged >79 years. Even in that group, those anemic at discharge tended to be at higher risk of dying within 30 days (Table 3).
Long-term mortality
Anemia on admission and at discharge was associated with a higher long-term mortality in all age groups and in the total patient cohort (Table 3).
Discussion
Data on the relationship between age, anemia, and sex in patients with MI and its possible association with the outcome are lacking. In this long-term follow-up study, we demonstrated age-specific sex-based differences in anemia in patients with MI. Younger women were more frequently anemic than their age-matched male counterparts. This difference disappeared from the age of 60 onward. At the end of hospitalization, the difference in age-specific anemia between the sexes was even greater.
Anemia was more often present in women and was linked to a worse 30-day and long-term mortality in the total patient cohort, which is consistent with previous data. 7,9,10,22,23 On the contrary, sex per se was not associated with 30-day mortality.
Similar to previous studies, we found that women were older, with more comorbidities and had a higher unadjusted short-term and long-term mortality. 2,5,24 We also found, as have others previously, that bleeding, renal dysfunction, hyperlipidemia, age, arterial hypertension, diabetes, and PCI of LMCA and LAD are associated with higher mortality. 16,17
We found a 22% lower multivariable adjusted risk of cumulative long-term mortality in women compared with men; hence, women actually have a better prognosis for survival than do men in the long run, which is in accordance with previous observations. 1 However, data on the association between sex and the outcome are still inconclusive and conflicting. 6,7,25
Surprisingly, anemia on admission was not associated with 30-day mortality in the group aged <60 years. In previous observations, anemia was associated with noncardiac mortality in younger anemic MI patients, but not with cardiac mortality. 26 In young women, hormonal changes (menstruation) might explain their higher prevalence of anemia, which is not associated with a poorer noncardiac short-term prognosis. In contrast, in elderly patients, anemia is more commonly associated with comorbidities (neoplasms, renal failure, etc.) that increase mortality.
Another possible explanation could be the hypothesis that young hearts are more resistant to anemia. 26 Unfortunately, we only had the data for all-cause mortality. In our opinion, the low number of events within 30 days (with an expected low noncardiac mortality in this age group) and the “relative resistance to anemia” of younger hearts were reasons for the similar 30-day all-cause mortality in this age group (Table 3). This would also explain why anemia (on admission and at discharge) with its several hemodynamic and nonhemodynamic effects on the cardiovascular system and an additional unfavorable effect on concomitant noncardiac diseases, is associated with higher all-cause long-term mortality in all age groups after MI (Table 3). 11,26,27
Bleeding, which is also related to ischemic complications, is the most common complication of modern therapy for MI. 12,16 Many patients are therefore discharged after PCI with hemoglobin levels that are lower than admission levels. 12 Anemia can worsen or develop even without overt bleeding during hospitalization in the intensive care unit. 28 In our analysis, women had a lower “reserve” before becoming anemic during hospitalization than men (123.6 ± 16.6 g/L hemoglobin on admission in women compared with 138.4 ± 17.2 g/L in men). As previously seen, women suffered more bleeding related to PCI than men. 1 Bleeding in women might be associated with smaller vessel size, which is an important risk factor for mechanical vessel injury during the procedure. 29 Younger women have a different estrogen status with increased levels of various coagulation factors and inflammatory markers that affect vascular endothelial function and its reaction to circulating vasoactive factors. 29 Premenopausal women may also have an abnormal arterial response to estrogen because of quantitative or qualitative abnormalities of blood estrogen receptors. 29 Furthermore, the women in our study weighed less than men (72.8 ± 13.9 kg in women vs. 85.6 ± 14.4 kg in men; p < 0.0001), they were more often admitted with renal dysfunction (with lower GFRs), but received antiplatelet drugs in the same doses as men. Women have higher circulating lipid levels that may be associated with drug exposure and volume of distribution. 30 All these factors may lead to sex-specific differences in drug bioavailability and distribution with a potential overdose of antiplatelet drugs. 30,31
Consistent with those findings, we found more anemia at the end of hospitalization and the difference between men and women was even greater than on admission (Table 2 and Fig. 1B). Actually, anemia at discharge was a more powerful predictor of mortality than anemia on admission in our analysis, and independently predicted 30-day mortality in the group aged 60 and less (Table 3).
Anemia decreases oxygen delivery to the body and myocardium. 23,26,28 The compensatory response to maintain adequate systemic oxygenation is a larger stroke volume and a higher heart rate. 10,22,26 The increased myocardial oxygen demand cannot be met in the setting of anemia because the oxygen supply is already decreased. 22 If the coronary arteries are not diseased, compensatory vasodilatation tries to maintain an adequate myocardial oxygenation. 32 However, in the setting of MI, anemia worsens ischemia by reducing oxygen delivery to the injured myocardium. 26 Anemia may also potentially be caused by occult diseases, such as malignancy or kidney dysfunction, which may actually be the major determinant of the poorer outcome. 26
In conclusion, we found age-specific sex-based differences in anemia in patients with MI. The prevalence of anemia increased with age in men, but a J-shaped relationship between age and anemia was found in women. The lower the age, the greater the difference in anemia between sexes, especially at discharge. Anemia was also linked with the 30-day and long-term mortality. Our data suggest that the increased prevalence of anemia in women younger than 60 years may help to explain the increased sex-related mortality in younger MI patients. These data need to be cautiously accepted because of the relatively small sample size in our analysis. The present findings should be considered as hypothesis generating for future trials in a similar setting.
Whether anemia on admittance in younger women is just related to menstruation and is simply a confounder, or whether anemia serves as a surrogate marker for sicker patients or anemia per se is directly linked to the outcome with its unfavorable effect on the whole body, is still to be elucidated in future research.
At present, we do not know exactly whether or not to treat anemia, and how to treat it in the acute phase of MI. Transfusion is not the right answer for every case of anemia in this setting. 33 There are some promising data on intravenous iron supplementation in patients with heart failure, but no data exist for patients with MI. 34 Until future investigations are undertaken, we should try to prevent any worsening of the anemia during treatment.
Limitations
This was an observational, single-center study. Our data only encompassed all-cause mortality. We lack data on smoking and the reason for the anemia on admission. Eventual comorbidities associated with anemia could have the potential to confound our analysis. The data on complications of PCI are also missing. In addition, the data on anticoagulation therapy, treatment with beta-blockers, and angiotensin-converting enzyme inhibitors are lacking.
Conclusion
Our data show age-specific sex-based differences in anemia in patients with MI. Women aged <60 years with MI more often suffer from anemia than their age-matched male peers. Anemia was associated with a worse outcome. These differences in anemia help to explain the increased sex-related mortality in women with MI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.