
Abstract
Background:
Hypertension is a major modifiable risk factor for coronary artery disease (CAD), the main cause of death in women. While association between the two is frequent, limited data exist regarding the feasibility of blood pressure (BP) management and outcomes in women across the spectrum of CAD. Accordingly, we analyzed patient characteristics, BP control rates, and outcomes among hypertensive women with CAD, enrolled in The INternational VErapamil SR-trandolapril STudy (INVEST).
Methods:
The 11,770 hypertensive women with CAD in INVEST were studied based on presence (n = 3,879) or absence (n = 7,891) of history of myocardial infarction (MI) or coronary revascularization, to evaluate outcomes across risk groups based on severity of CAD.
Results:
Women with prior MI or revascularization were older (4 years, p < 0.0001), were predominantly white (62% vs. 29%), and had more associated comorbidities than women without these events. At 24 months, JNC VI (sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure) BP control rates were lower in women with prior MI or revascularization (57% vs. 64%, p < 0.0001), despite more intensive antihypertensive therapy. The primary outcome (first occurrence of all-cause death, nonfatal MI, or nonfatal stroke) was also more frequent in women with prior MI or revascularization (adjusted hazard ratio [HR] 1.53, 95% confidence interval [CI] 1.34–1.74), who were 42% more likely to die (adjusted HR 1.42; 95% CI 1.22–1.64), twice as likely to have a nonfatal MI (adjusted HR 2.4, 95% CI 1.64–3.51), and 56% more likely to have a nonfatal stroke (adjusted HR 1.56, 95% CI 1.1–2.21).
Conclusions:
In a prospective, multinational cohort of hypertensive women with CAD, those with prior MI or revascularization comprised a group at higher risk for death, nonfatal MI, and nonfatal stroke, and were less likely to have their BP controlled, despite more aggressive therapy. The feasibility and benefit of reducing BP to <130/80 mmHg in women, particularly with more severe CAD, warrant further investigation.
Introduction
Hypertension is the most prevalent modifiable risk factor for mortality in women. 1 It is a major contributor to coronary artery disease (CAD), as well as to stroke, heart failure (HF), and chronic kidney disease. Both hypertension 2 and CAD 3 occur a decade later in life for women. This has led to a lower perceived risk among both the public 4,5 and health care practitioners, 5 –7 with consequent lax adherence to guideline-directed therapy in these women. 2 Consequently, many women, even those with end-organ damage such as prior stroke or transient ischemic attack, do not have blood pressure (BP) adequately controlled. 8 –10
The 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults 11 recommended a lower treatment target (<130/80 mmHg) for patients with CAD based on data from the recent Systolic Blood Pressure Intervention Trial (SPRINT) 12 and other randomized controlled trials and meta-analyses. 11 However, there is a paucity of data to support such treatment targets in CAD patients, who represented a minority of the population included in these studies. This discrepancy is particularly relevant in women, who were underenrolled in SPRINT 12 and other studies. 13
Sex-based differences in cardiovascular pathophysiology are supported by the interplay of traditional cardiovascular risk factors, lifetime hormonal cycling, and nontraditional cardiovascular risk factors in the female population. 2,13 This heterogeneity of risk is reflected in the phenotypic expression of CAD, with women more frequently displaying myocardial ischemia with no obstructions on the coronary arteries (INOCA) than classical obstructive CAD. 14 –16 Although the INOCA syndrome was considered benign for decades, contemporary studies have proven that angina caused by coronary microvascular dysfunction in the absence of significant atherosclerotic obstruction entails a significant negative impact on patient prognosis. 16 –18
The lack of data on hypertensive women with CAD prompted this evaluation of data from The INternational VErapamil-trandolapril STudy (INVEST), which enrolled 22,576 participants with hypertension and CAD. Having included 11,770 women, INVEST is the largest cohort of hypertensive women enrolled in a clinical trial to date. Importantly, these women span the entire spectrum of CAD, from angina to myocardial infarction (MI). The purpose of this analysis was to evaluate BP control rates and the relationship between baseline CAD severity and adverse outcomes in women.
Methods
Study design and treatment
The design, baseline characteristics, and outcomes of INVEST are detailed elsewhere. 19 –22 Briefly, hypertensive patients ≥50 years old with a CAD diagnosis were randomized to either a calcium channel blocker- or beta-blocker-based antihypertensive regimen and planned follow-up for a minimum of 24 months. A CAD diagnosis was required for inclusion in the study and was based on the presence of one of the following signs of symptoms of myocardial ischemia: classic angina pectoris, concordant abnormalities suggestive of ischemia on two different types of stress test, angiographic coronary stenosis ≥50%, prior myocardial revascularization, or a remote (≥3 months before enrollment) confirmed MI. Patients with diabetes, renal failure, and HF class I–III were included. Patients treated with beta-blockers 2 weeks before randomization were excluded to avoid withdrawal phenomena in those assigned to the calcium blocker group. INVEST BP management was guided by the recommendations of the sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI), which included a BP target ≤140/90 mmHg, except for patients with diabetes, chronic kidney disease, and HF, for whom a BP ≤130/85 mmHg was targeted.
The two treatment strategies were found to be equivalent relative to prevention of the primary outcome, other adverse outcomes, and BP control rates (∼63% according to JNC VI guidelines). Thus, the treatment strategies were combined for this cohort analysis.
In this analysis, we compared women who had experienced an MI or coronary revascularization with those that exhibited other signs or symptoms of myocardial ischemia before study entry, as specified in the inclusion criteria. Prior MI was defined as history of documented MI, and coronary revascularization was defined as history of percutaneous coronary intervention or coronary artery bypass graft surgery. The primary outcome was first occurrence of death (all cause), nonfatal MI, or nonfatal stroke. Secondary outcomes included the individual components of the primary outcome. Additional prospectively specified secondary outcomes were, among others, BP control and cardiovascular death. 20 All outcomes were adjudicated by the events committee.
Statistical analysis
Baseline data were summarized as means and standard deviations (SDs) for continuous variables, or numbers and percentages for categorical variables. Chi-square test was used for categorical variables and t-test for numerical variables to compare different characteristics between women with and without prior MI or revascularization. Kaplan-Meier method and log-rank test were used to compare the time to adverse outcome in women with prior MI or revascularization to those without. Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for each adverse outcome. Each model was fit using stepwise selection with the following prespecified covariates forced into all models: treatment strategy, age, HF, and race/ethnicity. Additional baseline covariates considered in the full model were age, origin in the United States, body mass index, baseline BP and heart rate, history of angina, left ventricular hypertrophy (LVH), arrhythmia, hypercholesterolemia, peripheral vascular disease, stroke or transient ischemic attack, diabetes mellitus, renal failure, cancer, and smoking. Covariates were entered into the model if p < 0.1 and retained in the model if p < 0.05. Data management and statistical analyses were performed using SAS statistical software (version 9.4; SAS Institute, Inc., Cary, NC).
Results
Baseline characteristics
Women with prior MI or revascularization differed significantly from women without, in all baseline characteristics, with the exception of body mass index (Table 1). Interestingly, Hispanic women represented a larger proportion of those without (52%) than those with prior MI or revascularization (20%, p < 0.0001). Women with prior MI or revascularization were older (mean ± SD, 69 ± 10 years vs. 65 ± 10 years, p < 0.0001) and more frequently exhibited CAD-associated risk factors (tobacco smoking, hyperlipidemia, and diabetes) and cardiovascular comorbidities (HF, arrhythmias or prior transient ischemic attacks, and stroke). While unstable angina was more frequent among women with prior MI or revascularization (17% vs. 6%, p < 0.0001), stable angina was two times more frequent in women without prior MI or revascularization (91% vs. 45%, p < 0.0001).
Patient Characteristics at Baseline
Number and percent if not stated otherwise.
Heart failure class IV patients were excluded.
History of or currently taking antidiabetic or lipid-lowering medications.
History of or currently have elevated serum creatinine level, but <4 mg/dL (<354 μmol/L).
Patients were not excluded if they had long survival expectancy.
Insulin and/or oral hypoglycemic.
BMI, body mass index; CABG, coronary artery bypass graft; LVH, left ventricular hypertrophy; MI, myocardial infarction; PVD, peripheral vascular disease; SD, standard deviation; TIA, transient ischemic attack.
The majority of women were receiving BP treatment before study enrollment (n = 10,394, Table 2). Baseline mean systolic blood pressure (SBP) was similar between groups (150.8 mmHg vs. 150.2 mmHg, p = 0.15), but diastolic blood pressure (DBP) was lower in the prior MI or revascularization group (84 mmHg vs. 88 mmHg, p < 0.0001). In treated women at baseline, SBP control rates were lower in those with prior MI or revascularization (32% vs. 35%, p = 0.004), despite requiring more intensive antihypertensive therapy (mean number of drugs, 1.8 vs. 1.6, p < 0.0001). A small number of women (n = 1,376, Table 2) were hypertensive and untreated with BP-lowering drugs before study enrollment. Their mean SBP was 161 mmHg.
Baseline Blood Pressure Control and Antihypertensive Medication
Included clonidine, methyldopa, and moxonidine.
Patients taking beta-blockers within 2 weeks from randomization were excluded from the study to avoid the confounding effect of withdrawal phenomena in patients randomized to the calcium channel-blocker strategy.
ACE, angiotensin-converting enzyme; BP, blood pressure.
Baseline medications also differed between groups (Table 1). One-third of the women with myocardial ischemia, but without prior MI or revascularization were treated with aspirin (37%), as opposed to two-thirds of women with prior MI or revascularization (70%, p < 0.0001).
Medication use and BP control at 24 months
The study and nonstudy BP-lowering drugs prescribed during the trial are summarized in Tables 3 and 4, respectively. While the number of study antihypertensive drugs as well as the mean dose of each agent were similar between study groups, women with prior MI or revascularization more frequently required additional antihypertensive nonstudy drug (53.2% vs. 38.5%, p < 0.0001, Table 4). Compared to baseline therapy, the frequency of antiplatelet treatment increased in women without (from 37% to 50%, p < 0.0001) and decreased in women with prior MI and revascularization (from 70% to 49%, p < 0.0001).
Study Antihypertensive Drug Use and Total Number of Antihypertensive Drugs at 24 Months
Nonstrategy Antihypertensive and Other Drug Use at 24 Months
NSAIDs, nonsteroidal anti-inflammatory drugs.
Over the course of the trial, there were small, but significant differences in SBP and DBP between groups (Fig. 1). Women with prior MI or revascularization had a mean SBP ∼2 mmHg higher from the first follow-up visit to the 18-month visit, and a mean DBP ∼2 mmHg lower throughout follow-up than women without prior MI or revascularization. Adjustment for heart rate, race, and age accounted for the difference in mean SBP (p = 0.82), but the difference in mean DBP remained significant (p < 0.0001).
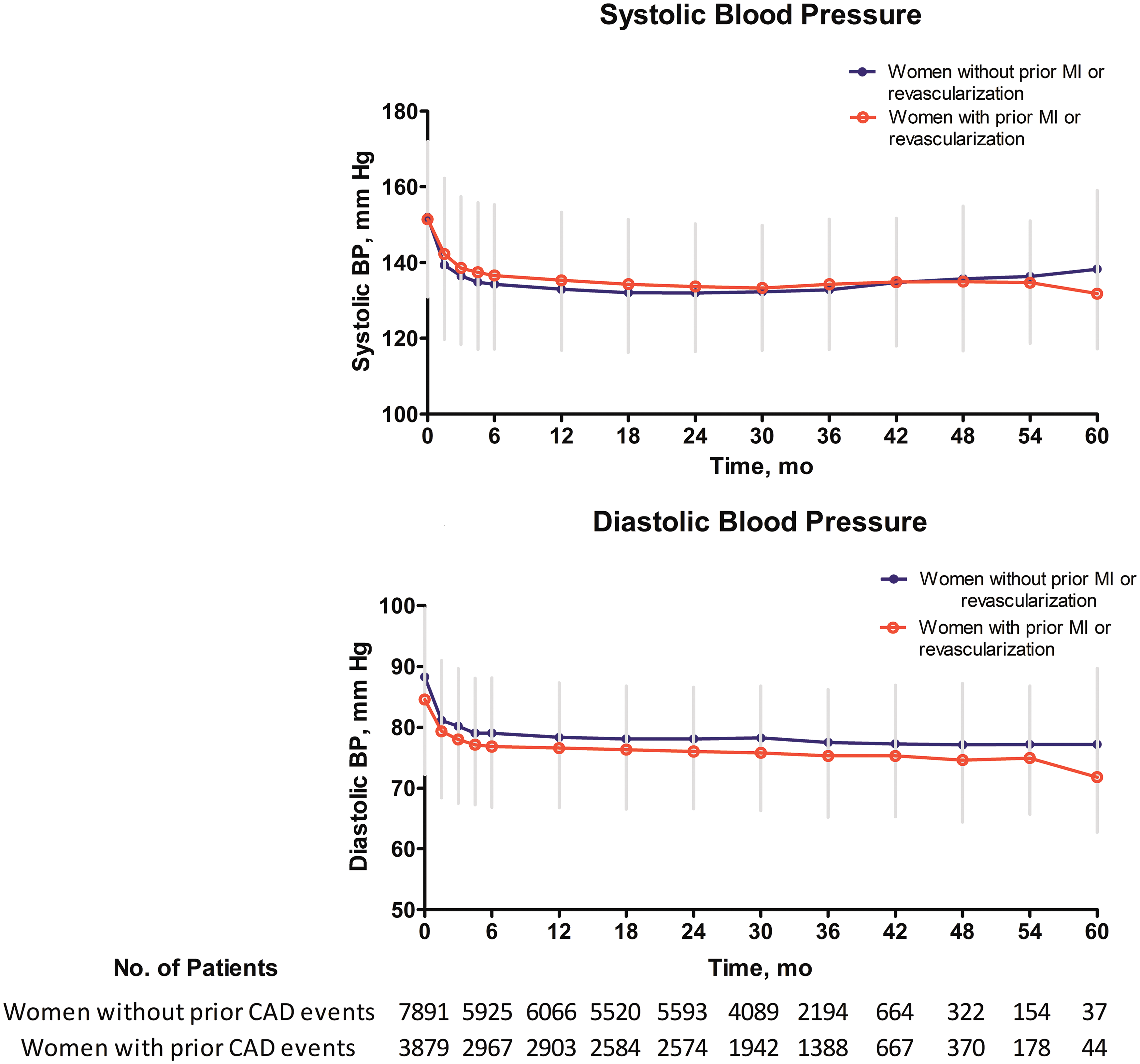
Mean systolic and diastolic blood pressure during the trial. The prespecified blood pressure targets applied in INVEST were according to the recommendations of the sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI) (<140/90 mmHg target, except for patients with heart failure, renal failure, or diabetes, for whom it was <130/85 mmHg). INVEST, INternational VErapamil SR-trandolapril STudy. Color images are available online.
BP control rates at 24 months were lower among women with prior MI or revascularization regardless of the BP threshold applied (Table 5). The highest BP control rates were achieved when considering a <140/90 mmHg threshold (68% vs. 71% in women with and without prior MI or revascularization, respectively, p = 0.0016). BP control according to JNC VI guidelines (≤140/90 mmHg, except for patients with diabetes, chronic kidney disease, and HF, for whom the target was ≤130/85 mmHg) was lower for both groups (57% vs. 64% in women with and without prior MI or revascularization, respectively, p < 0.0001). The lowest BP control rates were seen when analyzing a cutoff of 130/80 mmHg, with no difference between the groups (27% vs. 29%, p = 0.24). Better rates were noted for reaching an SBP target <130 mmHg; however, women with prior MI or revascularization continued to have significantly lower rates of control (40% vs. 45%, p = 0.0001).
Blood Pressure Control Rates at 24 Months
JNC VI recommended BP targets were <140/90 mmHg, with the exception of patients with heart failure, renal failure, or diabetes, for which it was <130/85 mmHg.
DBP, diastolic blood pressure; JNC VI, sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; SBP, systolic blood pressure.
Adjudicated outcomes
In unadjusted analyses, women with prior MI or revascularization were at higher risk for the primary outcome than women with signs of myocardial ischemia, but without prior MI or revascularization (Fig. 2). A total of 1,148 women experienced a nonfatal MI, nonfatal stroke, or all-cause death (629 in the prior MI or revascularization group). All-cause death was the most frequent event, with 922 women dying, of which 495 had prior MI or revascularization. Nonfatal MI occurred in 133 women (86 in the prior MI or revascularization group) and nonfatal strokes in 148 women (83 in the prior MI or revascularization group). Of the 922 deaths due to any cause, 407 were attributable to cardiovascular causes (217 in women with prior MI or revascularization).
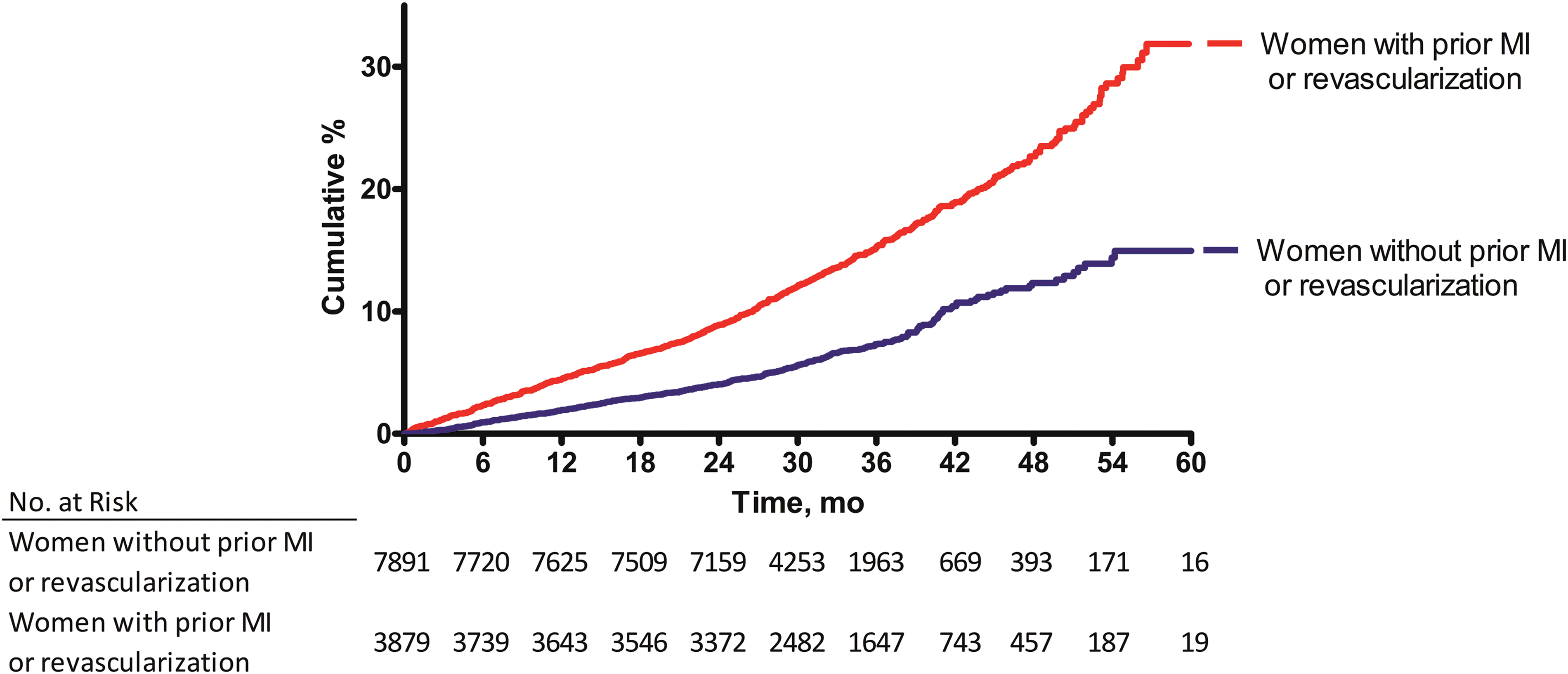
The primary outcome by risk group. Cumulative incidence of the primary outcome, which was first occurrence of death (all cause), nonfatal MI, or nonfatal stroke. MI, myocardial infarction. Color images are available online.
After adjustment, the incidence for the primary outcome and all secondary outcomes was significantly higher among women with prior MI or revascularization (Fig. 3). Women with prior MI or revascularization had an HR of 1.53 (95% CI 1.34–1.74) for the primary outcome, an HR of 1.42 (95% CI 1.23–1.64) for all-cause death, an HR of 2.40 (95% CI 1.64–3.51) for nonfatal MI, and an HR of 1.56 (95% CI 1.10–2.21) for nonfatal stroke. Risk of the primary outcome was also greater among women with prior MI or revascularization than those without across a variety of subgroups (Fig. 4). However, there were significant interactions between risk group and age, risk group and LVH, and risk group and race with regard to the magnitude of risk difference, comparing those with prior MI or revascularization to those without. Specifically, women with LVH and prior MI or revascularization were at significantly greater risk of the primary outcome than those with prior MI or revascularization, but without LVH. Likewise, non-white women with prior MI or revascularization were at significantly greater risk than white women with prior MI or revascularization.
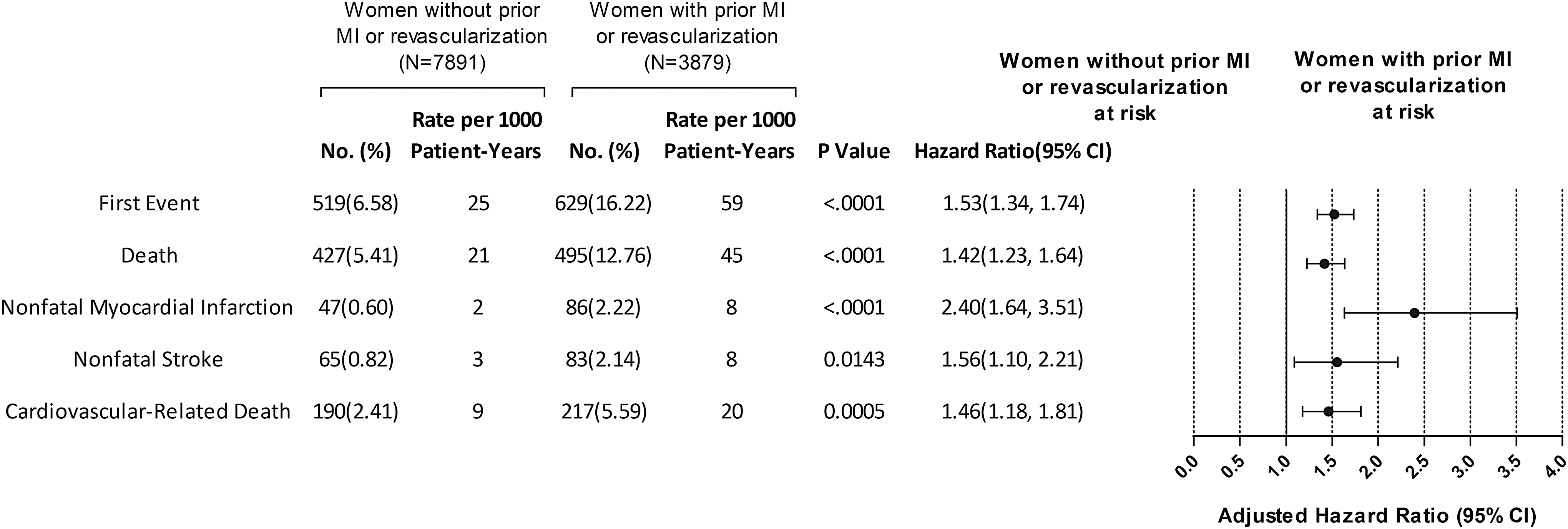
Primary and secondary outcomes by risk group. CI, confidence interval.
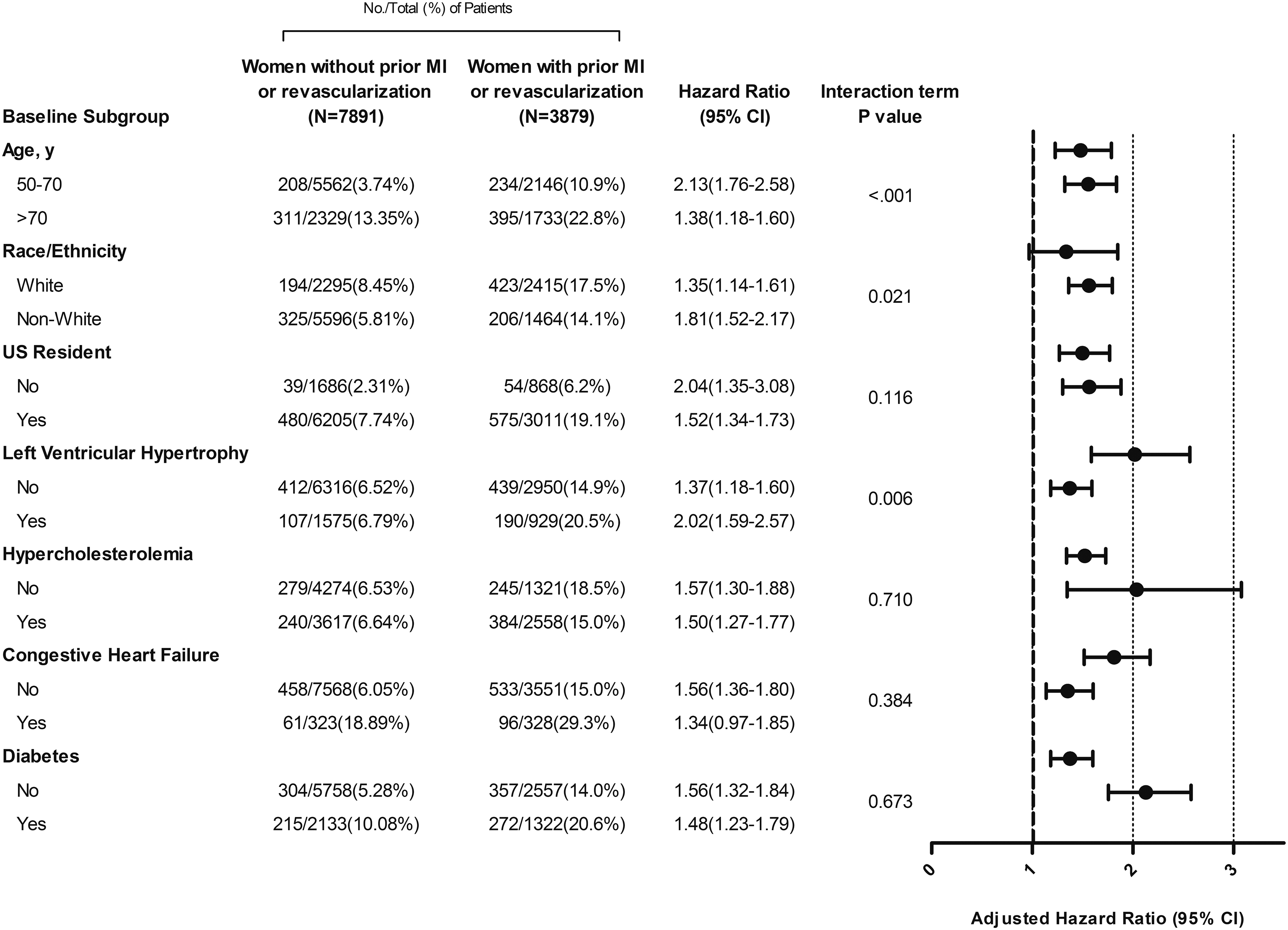
The primary outcome in subgroups defined by baseline patient characteristics.
Discussion
The INVEST study, due to robust enrollment of women, provided an opportunity to examine the impact of aggressive antihypertensive treatment on BP control and to assess the risk of adverse outcomes across the spectrum of CAD. The antihypertensive strategy used in INVEST remains relevant in the current era. The hypertensive women with CAD, who had prior MI or revascularization, represented an objectively characterized subgroup with significantly worse outcomes than women with other signs and symptoms of myocardial ischemia. Even after controlling for confounders, women with prior MI or revascularization had a 53% increased relative risk for the primary outcome, translating into 42% increased relative risk of all-cause death, a 140% increased relative risk for nonfatal MI, and a 56% increased relative risk for nonfatal stroke, despite achieving high rates of BP control. These data, together with the latest AHA Heart Disease statistics, 3 support the notion that hypertensive women with CAD differ from men in terms of risk of death and other serious adverse events, even when BP is aggressively treated and fairly well controlled.
INVEST has proven that adequate BP control with intensive medical therapy is achievable, with women reaching the older target of 140/90 mmHg BP more frequently than those in ALL-HAT 23 (70% vs. 55.8% at 24 months of treatment). This is also superior to BP control rates in the community, which were estimated around 32% between 1999 and 2000 and 48% most recently by the National Health and Nutrition Examination Survey. 24 Compared to the <140/90 mmHg target, the lower JNC VI BP targets were more difficult to achieve in INVEST women with prior MI or revascularization (58% and 68%, respectively, p < 0.0001) than in those without (64% and 71%, respectively, p < 0.0001), despite more intensive, maximally tolerated antihypertensive therapy with both study and nonstudy drugs. Thus, our data reinforce the question raised by SPRINT investigators regarding the feasibility of a lower SBP target in clinical settings not covered by their eligibility criteria, such as patients with severe hypertension and diabetes. 13 Women enrolled in INVEST were at higher risk than those included in SPRINT: mean SBP was 11 mmHg higher (151 mmHg vs. 140 mmHg, respectively), 28% had type 2 diabetes, and all had CAD. Although the ACCORD trial showed that SBP thresholds of <120 mmHg were achievable in type 2 diabetics with increased cardiovascular risk, 25 we have previously shown that patients with hypertension, CAD, and diabetes, and tight BP control do not have improved outcomes. 26 Our current analysis adds the knowledge that lower BP targets are more difficult to achieve in women after an MI or myocardial revascularization than in women with other signs and symptoms of myocardial ischemia.
Analysis of the differences in baseline characteristics between the two groups of women provides clues regarding outcome differences among INVEST women. Ethnicity varied significantly between groups, with women without prior MI or revascularization being mainly Hispanic (52%) and women with prior MI or revascularization being mainly white (62%). These findings are supported by epidemiological reports contemporary to the INVEST study, which showed Hispanic women had about 20% less risk of dying from cardiovascular disease than white women, 27 and by coronary imaging studies, which demonstrated significantly lower frequency of obstructive CAD and of coronary artery calcification. 28 LVH has been shown to independently predict CAD events 29 and HF development. 29,30 In INVEST, presence of LVH at baseline further increased the excess risk associated with prior MI or revascularization (Fig. 4). This is significant, as hypertension is the main driver of LVH, and treatment of hypertension has been shown to induce regression of LVH 30 as well as to reduce the risk of progression to HF. 31 Diabetes was more frequent among women with prior MI or revascularization (34% vs. 27%, p < 0.000), and diabetic women had a higher incidence of the primary outcome regardless of CAD event group. This is in accordance with prior literature showing BP control is less effective in patients with type 2 diabetes. 32
In view of these findings and considering women's unique cardiovascular risk profile that combines both traditional and nontraditional risk factors, 2,13 we believe that equipoise persists regarding the efficacy of new BP guidelines to improve outcomes in women with CAD. Further research is necessary to establish the ideal BP targets for patients, and especially for women, with CAD.
Conclusions
Among hypertensive women with CAD enrolled in INVEST, a history of prior MI or revascularization was associated with an increased risk of adverse outcomes. Adequate BP control was achievable at high rates; however, BP was less amenable to treatment in women with more severe CAD, despite more intensive BP-lowering therapy. These results emphasize the need for future investigation regarding adequate BP targets, as well as the feasibility of BP control in hypertensive women with CAD, to improve health outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.