
Abstract
Background:
While caesarean section (CS) can be a lifesaving intervention when performed in a timely manner to overcome dystocia or other complications, it is a traumatic event and may increase the risk of post-traumatic stress disorder (PTSD). No attempt has been made to assess prevalence of PTSD after CS specifically. This study aimed to quantify pooled prevalence of PTSD after CS through a systematic review and meta-analysis.
Methods:
MEDLINE, PsycINFO, EMBASE, and CINAHL were searched using PTSD terms crossed with CS terms. Studies were included if they reported the prevalence of PTSD after CS using an instrument based on Diagnostic and Statistical Manual of Mental Disorders-criteria to identify PTSD. The pooled prevalence was then estimated by meta-analysis in overall eligible studies and in subgroups.
Results:
Nine studies were included with a total of 1,134 postpartum women, of which 136 were identified as having PTSD. Pooled prevalence of PTSD after CS was 10.7% (95% confidence interval [CI]: 4.0–20.2). Pooled prevalence of PTSD after emergency CS (10.3% [95% CI: 1.7–24.9]) was higher than that after elective CS (7.1% [95% CI: 0.7–19.4]), but the difference was not statistically significant. Subgroup analysis showed that pooled prevalence of PTSD after CS differed according to study setting, time interval of PTSD assessment, and type of participants. Meta-regression analysis showed that study setting and type of study participants were significant sources of heterogeneity.
Conclusions:
Women with CS apparently have higher rates of PTSD as compared with women without CS. However, the susceptibility to PTSD appears to vary based on emergency/elective CS, study methodology, self-perceived traumatic birth, and country of study. Further targeted research is needed to elucidate the role of these factors in relationship between CS and PTSD.
Introduction
Childbearing is often not a normal physiological process: ∼20%–45% of women perceive their childbirth as having been a traumatic event, which can lead to post-traumatic stress disorder (PTSD). 1 –4 In recent years, PTSD after childbirth has received increasing attention of researchers and clinicians alike. 5 –7 Previous systematic reviews have reported that PTSD affected ∼4.0% of postpartum women. 4 According to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-V), 8 PTSD is an anxiety disorder experienced after a potentially fatal traumatic event. Clinical symptoms of PTSD include intrusive thoughts, avoidance of stimuli associated with the event, increased arousal not present before that event, and negative alteration in cognition and mood associated with the event. 8 PTSD may have a negative impact on women, birth outcomes, mother/baby bonding, and infant emotional development. 9 –12
Caesarean section (CS) is lifesaving when performed in a timely manner to overcome certain types of dystocia or other pregnancy complications. 13 The World Health Organization and the international health care community consider the ideal rate for CS to be 10%–15%. 14 However, rates of CS have been increasing steadily in both developed and developing countries, 14 reaching 30% or 40% in some countries. 15 –19 Higher CS rates may increase the risk of adverse outcomes in both mothers and babies. 13,20 –22 While obstetrical complications in women after CS are well studied, research on the psychological consequences of CS is sparse. 23 Since the first publication by Bydlowski 24 on adverse psychological outcomes in women after pregnancy, researchers have attempted to identify perinatal risk factors for PTSD. CS appears to be one of the main predictors for PTSD. 3 Previous systematic reviews have reported prevalence of PTSD after childbirth; however, none of these reviews evaluated the prevalence of PTSD after CS. The objective of this study is to quantify the pooled prevalence of PTSD after CS based on a systematic review and meta-analysis of the available data on this important health issue.
Methods
This review was conducted following the Preferred Reporting Item for Systematic Reviews and Meta-analyses (PRISMA) statement. 25 The study protocol was registered with the PROSPERO (CRD42018115595) before data extraction.
Search strategy
With the support of two librarians with expertise in conducting systematic reviews on health services delivery, a systematic search of the literature was conducted to identify relevant studies using the following databases: MEDLINE, PsycINFO, EMBASE, and CINAHL. The literature search included all published articles from inception of each database through to November 30, 2018.
A combination of key terms and/or subject headings was applied, including PTSD terms (stress disorders, post-traumatic, posttraumatic stress disorder*, posttraumatic stress disorder*, post traumatic neuros*, posttraumatic neuros*, ptsd) and cesarean-section-related terms (cesarean section, cesarean section*, caesarean section*, cesarean deliver*, caesarean deliver*).
Selection process
Titles and abstracts of all articles retrieved using the search criteria defined above were screened independently by two authors (Y.C. and X.Y.) to determine if they met the predetermined inclusion/exclusion criteria; full-text screening was then performed to identify studies to be included in the present review. Any disagreements regarding eligibility were resolved by discussion with a third author (R-H.X.).
Inclusion/exclusion criteria
Studies were included in this systematic review if they met the following criteria: (1) the study design was observational; (2) target population were women who had undergone CS (for studies including both CS and vaginal deliveries, only CS deliveries were included in the meta-analysis); (3) PTSD lasted ∼1 month after birth; (4) the instrument used to identify PTSD was based on the DSM criteria (or equivalent); (5) information about the sample size and the prevalence of PTSD among women after CS was provided; and (6) the full article was written in English. Studies were excluded if they were abstracts, interviews, commentaries, reviews, or book chapters. Studies reporting PTSD symptoms in relation to psychiatric disorders such as anxiety, depression, and pregnancy loss such as spontaneous abortion, miscarriage, or stillbirth were also excluded.
Data extraction
Two investigators (Y.C. and X.Y.) independently extracted relevant data from eligible articles using standard forms. The following data were recorded from each eligible study: last name of the first author, publication year, country of study, age of study participants, study setting, study design, instrument used to identify PTSD, time interval from childbirth to PTSD assessment, type of study participants, number of CSs, and number of PTSDs after CS. The instruments used to identify PTSD were categorized into self-report questionnaires and structured interviews. The self-report questionnaires included different sections to assess all DSM-IV-TR criteria (A-F), specifically, Impact of Event Scale (IES)-15, Traumatic Event Scale (TES), and Post-traumatic Stress Diagnostic Scale (
Quality assessment
Risk of bias and quality of study were assessed using Newcastle Ottawa Scale (NOS), a scoring tool used to assess quality of evidence and risk of bias for nonrandomized studies included in the systematic review. 26 Using a set of preprepared and piloted tested guidelines, two authors (Y.C. and X.Y.) assessed the quality of study in the following domains: sample selection (maximum five points; considering representativeness of the sample, sample size, nonrespondents, exposure (risk factor), ascertainment), comparability (maximum two points; based on the extent to which confounding factors are controlled), and outcome measures (maximum three points; outcome ascertainment, statistical analysis). The total NOS score can range from 0 to 10 points, with a higher score indicating higher quality.
Data analysis
Data analysis was conducted using the “meta” and “metaphor” modules in R Version 3.4.1. 27 Heterogeneity across studies was assessed using the Higgins I 2 statistic. In case of significant heterogeneity (I 2 ≥0), the random-effects model of Der-Simonian and Laird was used to obtain the pooled prevalence of PTSD; otherwise, in case of no inconsistency in risk estimates (I 2 = 0), a fixed-effects model was used. 28
Subgroup analysis was carried out to identify the pooled prevalence according to the instruments used to identify PTSD (self-report questionnaire vs. structured interview), study setting (hospital vs. community health care center), time interval between childbirth and PTSD assessment (4–8 weeks vs. >8 weeks vs. 4 weeks to >12 months postpartum), and type of study participants (women with self-perceived traumatic birth vs. general postpartum women). The significance of differences within each subgroup was compared using the chi-square test.
When significant heterogeneity was observed, mixed-model meta-regression analysis was conducted to explore the influence of potential moderators of heterogeneity using the restricted maximum-likelihood method. Effect moderators considered in the models included the following: instrument used to identify PTSD, study settings, time interval between childbirth and PTSD assessment, type of study participants, and quality of eligible studies.
Sensitivity analysis was performed by serially removing each study and by excluding low-quality studies to show their corresponding effects on the stability and strength of the pooled results. 29,30 Potential publication biases were assessed graphically using funnel plots and statistically (p < 0.1) using Egger's tests. 28
Results
Search results
A total of 334 studies were initially identified through electronic search. After removal of duplicate articles and title/abstract screening, 30 studies were selected for full-text review. Of these 30 studies, 18 were excluded due to lack of information about the prevalence of PTSD after CS, 1 was excluded for not using the instrument based on DSM-IV criteria to identify PTSD, 1 was excluded because it was an interview, and 1 was excluded because PTSD did not last 1 month after birth. Nine eligible studies 3,31 –38 were included in the final analysis (Fig. 1).
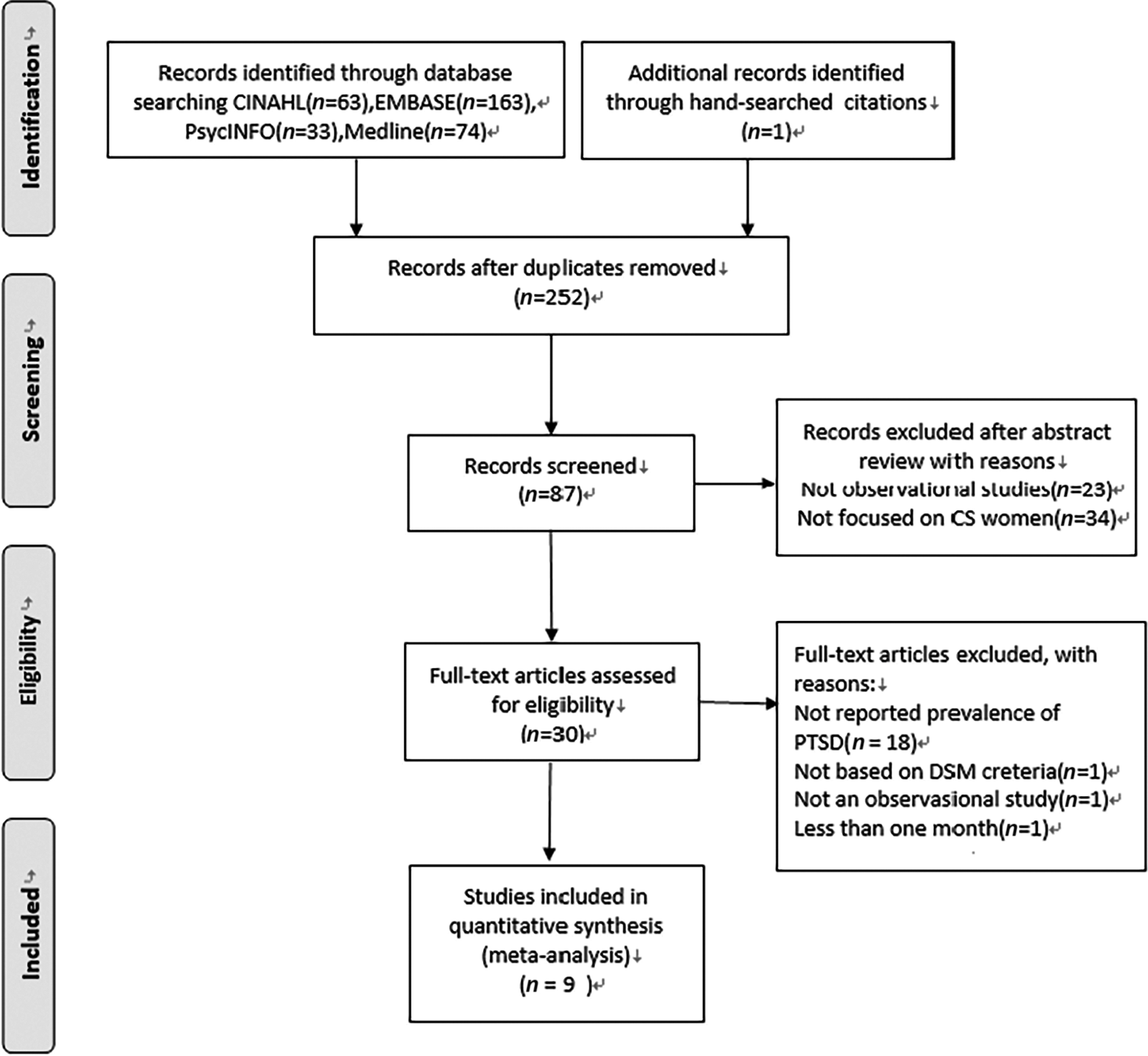
Systematic review flow chart. CS, caesarean section; DSM, Diagnostic and Statistical Manual of Mental Disorders; PTSD, post-traumatic stress disorder.
Characteristics of selected studies
The nine eligible studies included in this review were published between 2002 and 2017 from seven countries: Nigeria, Iran, Sweden, Turkey, Switzerland, Israel, and Canada. Among the nine studies, the sample size ranged from 42 to 217 with a total of 1,134 women, of whom 136 were identified as suffering from PTSD. Three studies were conducted in community health care centers and six in hospitals. Five studies used exclusively self-report questionnaire to identify PTSD (one of them used TES that met all DSM-IV criteria for PTSD) and four used exclusively structured interview. Two studies recruited women who perceived birth as a traumatic event and seven recruited women from general obstetric population. Seven studies identified PTSD in the period of 4–8 weeks postpartum, one study identified PTSD at >8 weeks postpartum, and one study identified PTSD from 4 weeks postpartum to >12 months (Table 1).
Characteristics of Included Studies
CAPS, the Clinician Administered PTSD Scale; CS, caesarean section; IES, the Impact of Event Scale; M.I.N.I., the MINI International Neuropsychiatric Interview; N/A, not available; NWS, the National Women's Study PTSD module; PDS, the Post-traumatic Stress Diagnostic Scale; PSS-I, the Post-traumatic Symptom Scale-Interview; PTSD, post-traumatic stress disorder; SD, standard deviation; TES, the Traumatic Event Scale.
Table 2 presents the results of quality assessment according to NOS. 26 All the studies included in this review were of fair quality with total score ranging from 4 to 7.
A Quality Assessment of Included Studies
The pooled prevalence of PTSD after CS
Figure 2 summarizes the prevalence of PTSD after CS, which varied widely from 2.1% to 42.5% among studies, with the highest in an Iranian population 34 and the lowest in a Canadian population. 36 The pooled prevalence for all studies was 10.7%, with 95% confidence interval (CI) 4.0–20.2.
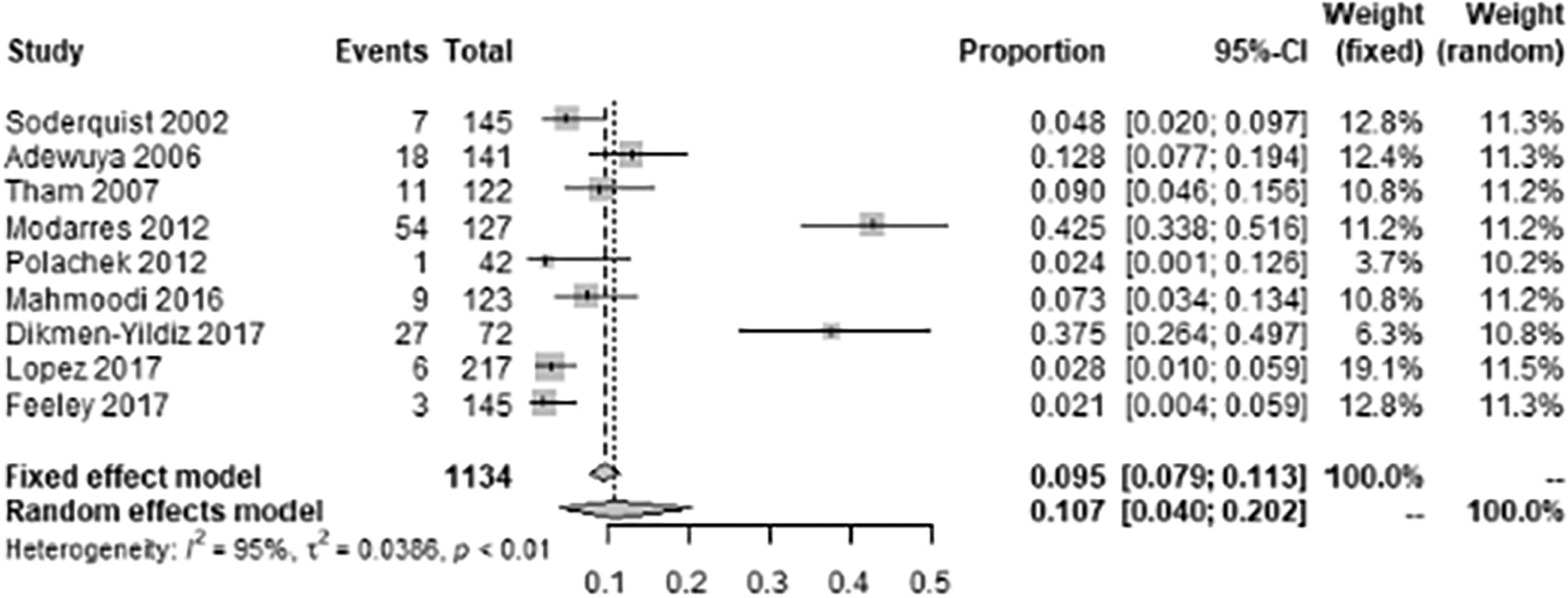
Forest plot showing prevalence of PTSD among women after caesarean section.
Table 3 shows the pooled prevalence of PTSD to be 10.3% (95% CI: 1.7–24.9) and 7.1% (95% CI: 0.7–19.4), respectively, after emergency CS and elective CS.
The Pooled Prevalence of Post-Traumatic Stress Disorder After Emergency Caesarean Section and Elective Caesarean Section
Among 9 eligible studies, 6 and 5 studies were additionally extracted data for Emergency and Elective CS, respectively.
CI, confidence interval.
Subgroup analysis
The pooled prevalence of PTSD after CS was 9.1% (95% CI: 1.3–22.9) and 12.1% (95% CI: 2.8–26.6), respectively, for PTSD cases identified by structured interview and self-report questionnaire. The pooled prevalence of PTSD after CS was 18.9% (95% CI: 3.7–42.2) and 7.3% (95% CI: 2.0–15.6), respectively, in women recruited from community health care centers and from hospitals. The pooled prevalence of PTSD was 40.7% (95% CI: 34.0–47.6) and 5.5% (95% CI: 2.9–8.7), respectively, in women with self-perceived traumatic birth and in women from general postpartum population. The pooled prevalence of PTSD was 12.0% (95% CI: 3.3–25.2), 9.0% (95% CI: 4.6–15.6), and 4.8% (95% CI: 2.0–9.7), respectively, for PTSD assessed at 4–8 weeks postpartum, >8 weeks postpartum, and 4 weeks to >12 months postpartum (Table 4).
Subgroup Analysis of the Pooled Prevalence of Post-Traumatic Stress Disorder After Caesarean Section
Meta-regression analysis
Meta-regression analysis found study setting and type of study participants as significant moderators for heterogeneity (p < 0.05) (Table 5).
Meta-Regression Analysis of the Effects of Potential Moderators
Sensitivity analysis and publication bias
Sensitivity analysis showed that after one-by-one removal of the nine eligible studies, the pooled prevalence of PTSD after CS varied from 7.9% (95% CI: 3.4–14.1) to 12.2% (95% CI: 4.5–23.0), with the corresponding I 2 statistic varying from 90% to 96%. Specifically, after removing one study that identified PTSD from 4 weeks to >12 months and one study that identified PTSD after 3 months postpartum, the pooled prevalence of PTSD identified from 4 to 8 postpartum weeks was 12.0% (95% CI: 3.3–25.2) and the I 2 statistic was 96% (Fig. 3).
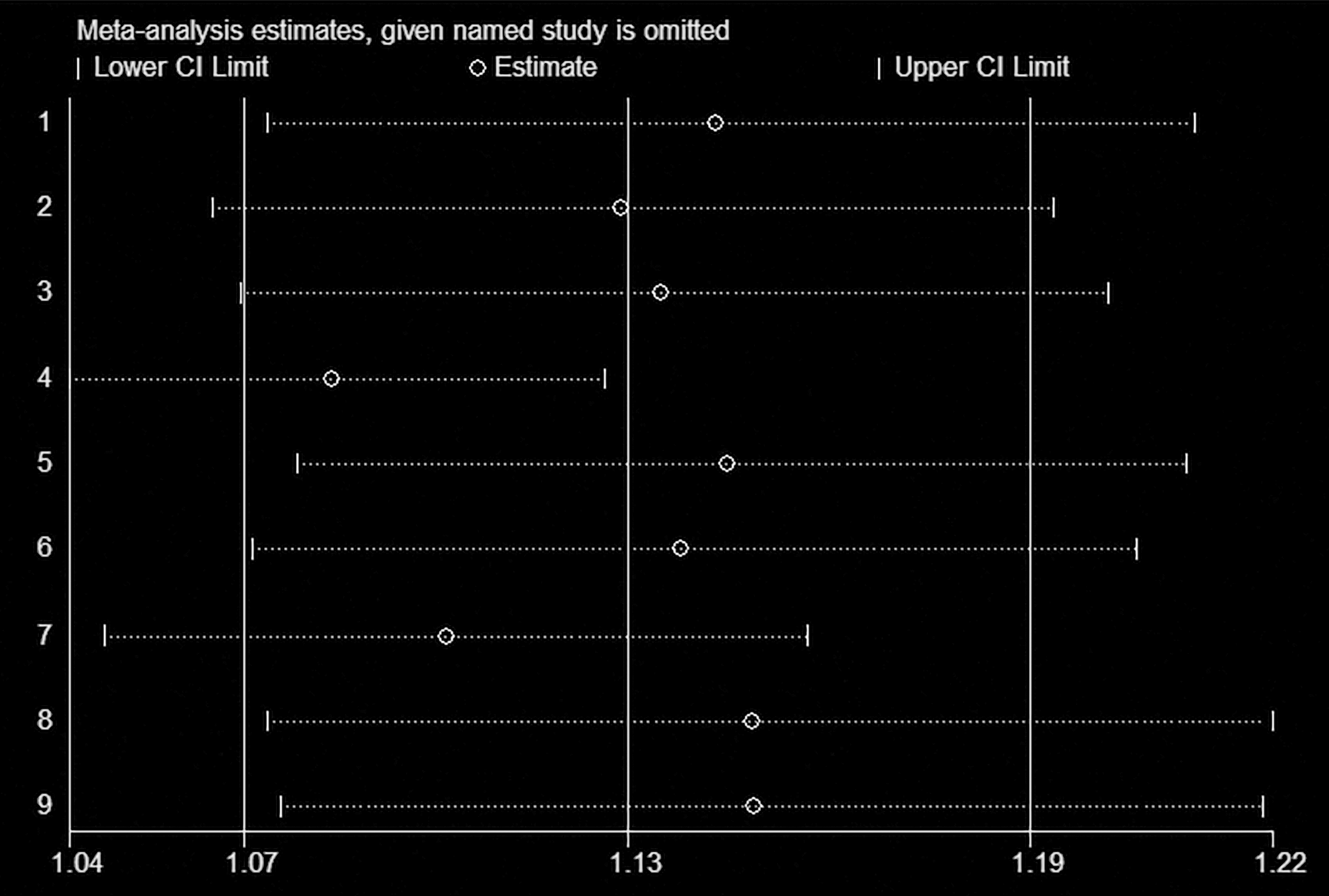
Sensitivity analysis of the eligible studies. CI, confidence interval.
Figure 4 presents Egger's funnel plot. Evidence of publication biases was not found in this meta-analysis, with p value for the Egger's rank test being 0.43.
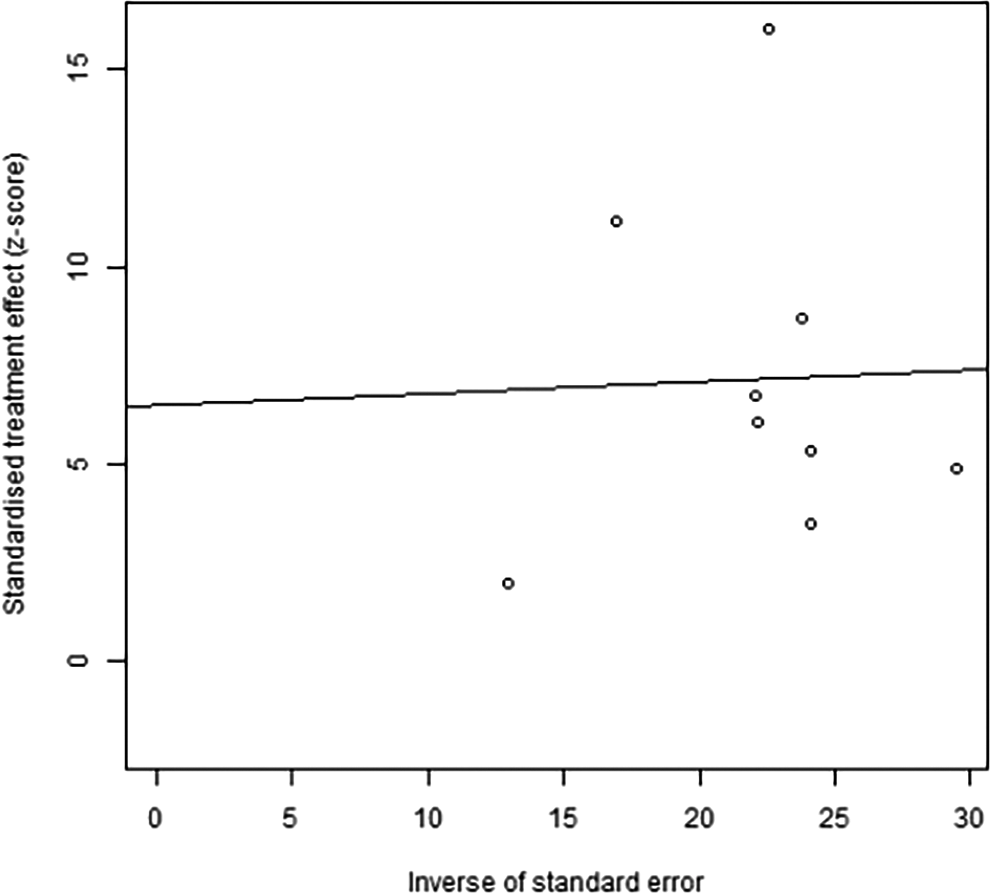
Egger's funnel plot of the eligible studies.
Discussion
Main findings of the study
Our systematic review and meta-analysis found that the pooled prevalence of PTSD after CS was 10.7% (95% CI: 4.0–20.2). In addition, the prevalence of PTSD after emergency CS tended to be higher than after elective CS. Subgroup analyses identified significant differences in the pooled prevalence of PTSD after CS based on study setting, time interval between childbirth, PTSD assessment method, and type of study participants.
Strengths and limitations
To our knowledge, no previous systematic review/meta-analysis has attempted to estimate the pooled prevalence of PTSD after CS. The present meta-analysis included all studies published on this topic in English to date. Our analysis made comparisons between emergency CS and elective CS. Furthermore, subgroup and sensitivity analyses were conducted to explore study heterogeneity. Statistical analysis did not reveal evidence of publication bias.
There are several limitations to this systematic review. First, the sample size was small, comprised of a total of 1,134 postpartum women, thereby complicating the interpretation of the results of the subgroup analysis. Second, the meta-analysis included only studies that identified PTSD using the instruments according to the DSM criteria, hindering generalization of the findings to the DSM-V criteria. Third, the heterogeneity of the papers based on variable methods of selection of study population, PTSD assessment tools, and time from CS to PTSD assessment resulted in wide range of prevalence estimate in pooled analysis, which may make it difficult for clinicians to directly correlate with their own clinical population. Finally, we could not adjust for potential confounders in meta-analysis due to heterogeneity in the content and format of available data in original studies.
Interpretation
Our study findings suggest that the pooled prevalence of PTSD among women who had CS was much higher than that for overall postpartum women in general. A previous systematic review of 59 studies originating from 23 countries with a total sample size of 24,267 women on all births including vaginal and CS births reported a mean prevalence of PTSD related to childbirth of 4.0% (95% CI: 2.77–5.71) in community samples. 4 This suggests that CS, especially emergency CS, is a main traumatic event. The result is also consistent with a previous study that mode of birth contributed much more to the variance in experiencing a traumatic birth than pre-existing psychiatric morbidity or prior traumatic events. 33
Elective CS is usually performed when there are medical indications such as placenta previa and pre-eclampsia, and elective CS could reduce the risk of perinatal mortality and morbidity. 15,17,39,40 Emergency CS, on the contrary, is often performed for women with no indication for a scheduled CS, but with problems such as dystocia and fetal distress during labor and delivery. 14,41 Although not statistically significant, the finding that the pooled prevalence of PTSD after emergency CS was higher than that after elective CS warrants further exploration. 35 Emergency CS is associated with more adverse, unpleasant childbirth experiences that may increase the risk for development of postpartum PTSD, 35 while elective CS may be a relief and benefit for pregnant women, especially for women with health problems, previous pregnancy complications, or adverse pregnancy experiences. 42
Although the structured interview is considered as a “gold standard” for diagnosis of PTSD, some of the widely used screening tools such as the TES and IES-R have high specificity and sensitivity. 31,32 Dai et al. synthesized data from 13 studies and found that the pooled prevalence of PTSD among road traffic accident survivors assessed using structured interviews was lower than that obtained using self-report questionnaires, 43 which is consistent with our finding that the pooled prevalence of PTSD after CS was higher in studies that used self-report questionnaires than those that used structured interview. Polachek et al 33 suggested that the DSM-IV criteria for diagnosis of PTSD may be too strict and may have excluded some persons with PTSD. On the contrary, a false-positive diagnosis and label of PTSD may have long-term adverse effects on women, their families, and health care system. To explore the long-term effects of this kind of wrong diagnosis for women and their families will help manage patients.
Subgroup analysis in our study that the pooled prevalence of PTSD among women with self-perceived traumatic birth was much higher than that in women from the general postpartum population. The results from our sensitivity analysis indicated that the type of study participants may affect the stability of the pooled prevalence. Also, meta-regression analysis showed that the type of study participants was a significant moderator for heterogeneity. Birth trauma is an event occurring during the labor and delivery process that involves actual or threatened serious injury or death to the mother and/or the infant. 38 Previous studies have shown that CS, especially emergency CS, is significantly related to traumatic stress symptoms, and that traumatic birth experience is a common reaction and a risk of PTSD, 2,44,45 which is consistent with our findings. However, a traumatic birth may not necessarily result in PTSD, and a substantial proportion of women with traumatic birth experience may recover. 37 Thus, continued screening and timely intervention for a traumatic birth after CS may be necessary for promoting recovery or preventing the worsening of PTSD symptoms after CS.
A significant difference in the pooled prevalence of PTSD after CS in different time periods after childbirth was observed, which is also consistent with previous studies. 36,37 PTSD may resolve naturally. 31,46 In addition, affective symptoms (depression and anxiety combined) emerged as robust predictor of birth-related PTSD trajectories at 4–6 weeks postpartum. 37 However, as few naturally recovered cases were observed after 6 months, PTSD cases persisting after that time are likely to continue as chronic cases and require treatment. 46
Subgroup analysis also found that the pooled prevalence of PTSD was significantly higher in studies from three community health care centers in Nigeria 38 and in Iran. 34,35 Different cultural backgrounds, baseline maternal characteristics, and maternity care experiences provided to these women may explain this higher prevalence of PTSD in the three community health care centers in these two countries in our systematic review. 34,35,38
Conclusions
Women with CS apparently have higher rates of PTSD as compared with women without CS. However, the susceptibility to PTSD appears to vary based on emergency/elective CS, study methodology, patient's self-perception of traumatic birth, and country of study. Further targeted research is needed to elucidate the role of these factors in relationship between CS and PTSD.
Footnotes
Acknowledgments
We thank all authors of the eligible articles and the two research librarians, Lindsey Sikora and Risa Shorr from the University of Ottawa and Ottawa Hospital Research Institute, for assistance in designing the literature search.
Authors' Contributions
R.-H.X. made substantial contributions to the conception and design of the review. Y.C., X.Y., T.G., Y.L., L.G., and W.C. participated in the acquisition of the data. Y.C., X.Y., T.G., and Y.L. contributed to the analysis and interpretation of the data. Y.C. and X.Y. drafted the article. R-H.X., I.C., D.K., and S.W.W. revised the article critically for important intellectual content. S.W.W. and R-H.X. approved the version of the article to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work has been partly supported by Canadian Institute of Health Research (FDN-148438), Southern Medical University (LC2019ZD019), and Nanhai Hospital of Southern Medical University (YNKT201802).