
Abstract
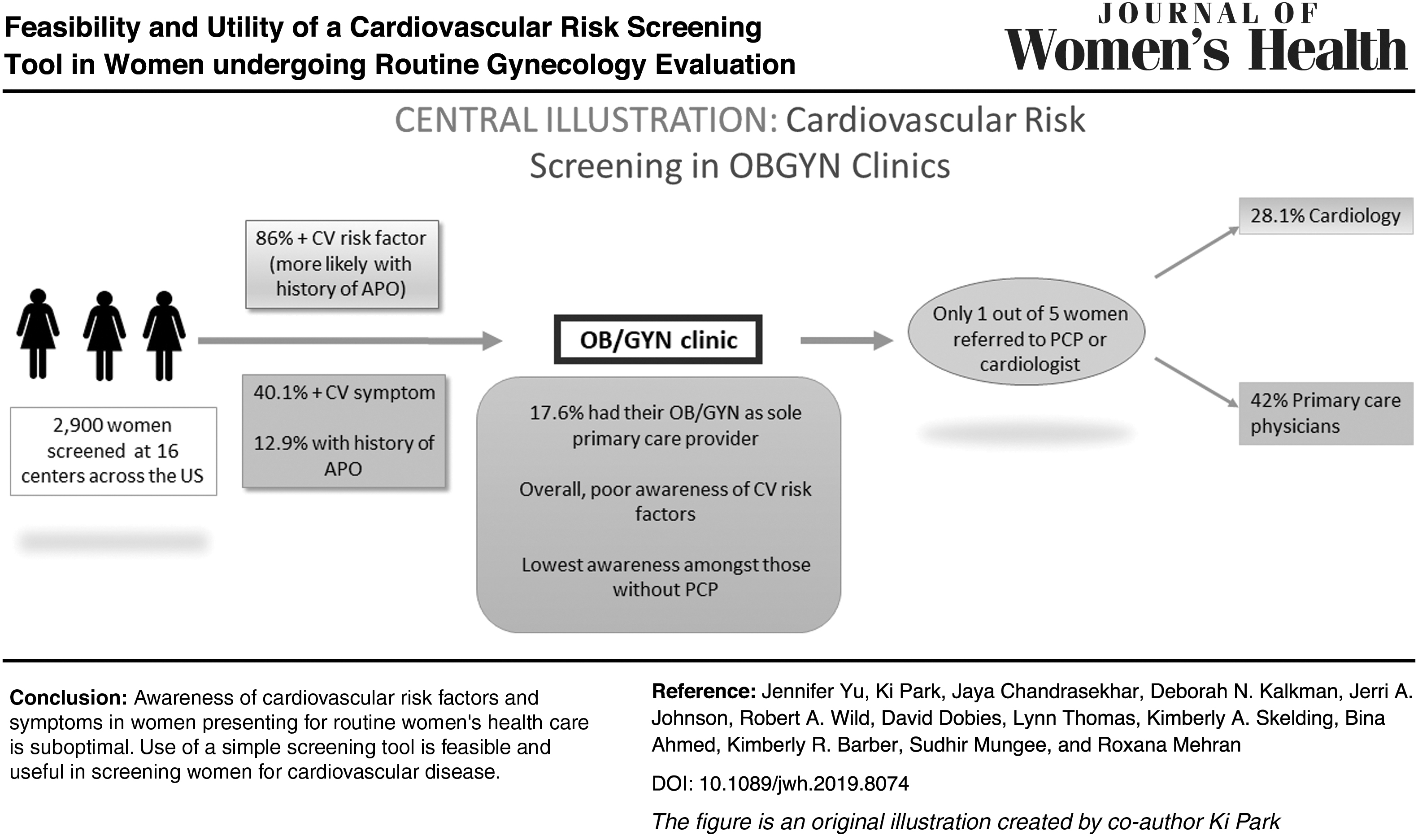
Graphical Abstract
Background:
The goals of this multicenter survey were to examine the prevalence and patient awareness of cardiovascular risk factors, and the association between history of adverse pregnancy outcomes (APO—including gestational hypertension, gestational diabetes, and preeclampsia) and prevalence of cardiovascular risks among women presenting to outpatient obstetrics/gynecology (OB/GYN) clinics.
Materials and Methods:
We surveyed 2,946 female patients attending 16 outpatient OB/GYN clinics across the United States between January 2010 and January 2012. Main outcome measures were self-reported cardiovascular risk factors and symptoms such as angina and dyspnea.
Results:
Mean age of the patients was 51 ± 13.6 years. Cardiovascular risks and symptoms were highly prevalent (86.0% and 40.1%, respectively). Many patients did not know if they had common risk factors such as hypertension, hypercholesterolemia, or diabetes (18.4%, 32.0%, and 17.9%, respectively). Women with a history of APO were slightly more likely to be aware of common risk factors, including abnormal blood pressure (17% vs. 18.6%), high cholesterol (31.7% vs. 32%), and obesity/elevated body mass index (43.9% vs. 49.7%). Compared with patients with no history of APO, patients with APO (n = 380, 12.9%) were more likely to have risk factors (89.5% vs. 83.9%, p = 0.002) and symptoms (45.5% vs. 39.3%, p = 0.02).
Conclusions:
Awareness of cardiovascular risk factors and symptoms among all women surveyed in this study was poor, although awareness for some risk factors was relatively higher among patients with APO. This study demonstrates the feasibility of cardiovascular assessment in OB/GYN clinics using a simple questionnaire and its potential role for early recognition and timely intervention.
Introduction
Cardiovascular disease is the leading cause of mortality among women in the United States. 1 In 2013, cardiovascular disease caused ∼1 death every 80 seconds among women in the United States, which represented over 398,000 deaths. 1 Despite such a significant disease impact among U.S. women, misconceptions regarding cardiovascular symptoms and barriers to care persist among women. In a cross-sectional survey of 2,300 U.S. women aged 25 years and above, only 53% indicated that they would call 9-1-1 if they perceived symptoms of a heart attack, and only 23% reported they would take aspirin. 2
Unique to women, history of adverse pregnancy outcomes (APO), including gestational hypertension, gestational diabetes, and preeclampsia/eclampsia are associated with increased long-term cardiovascular risk. 3 –5 For a large proportion of women (∼35%) in the United States, an obstetrician/gynecologist (OB/GYN) is their only health care provider, 6 which represents an important opportunity for early diagnosis and education regarding cardiovascular risk factors. However, contemporary data on the prevalence of cardiovascular risk factors among women seen for routine care in OB/GYN clinics and their association with previous APO are lacking.
Thus, the objectives of this multicenter study were to survey women presenting to outpatient OB/GYN clinics for their routine care to assess (1) the prevalence of self-reported cardiovascular risk factors and symptoms among women, (2) the level of patient awareness regarding their cardiovascular risk factors, and (3) prevalence of cardiovascular risk factors and symptoms in women with or without a history of APO.
Materials and Methods
Patient population
A screening program was developed in consultation with leaders from the Society of Cardiac Angiography and Interventions–Women in Innovations (SCAI-WIN), American College of Cardiology (ACC) and the American Congress of Obstetricians and Gynecologists (ACOG), along with representatives from Abbott Vascular, which funded the program. Sixteen OB/GYN centers across the United States participated in the study (Appendix Table A1). Study participants were subjects attending the 16 OB/GYN clinics who were given a one page, 30-question survey (Appendix Table A1 and Appendix Fig. A1), which sought to assess traditional and gestational cardiovascular risk factors and any current symptoms. Blood pressure and cholesterol data were abstracted from the medical record if not provided by the patient. After survey completion, results were reviewed with a nurse or physician. The reason for the visit was not collected. A member of the research team, who also explained the Health Insurance Portability and Accountability Act (HIPAA) forms, oversaw the process.
A physician, nurse, or nurse practitioner assessed the survey responses to determine the appropriateness of referral to another health care professional (primary care physician, cardiologist, endocrinologist, nurse practitioner, or physician assistant).
Definitions
For the purposes of this study, APO was defined as patients who reported a history of gestational diabetes, gestational hypertension, and/or preeclampsia/eclampsia. Traditional cardiovascular risk factors were hypertension (reported or measured blood pressure ≥140/90 mmHg), high cholesterol (self-reported cholesterol >200 mmHg or on cholesterol treatment), diabetes (self-reported or on medications), any cigarette smoking history (current and ex-smokers), and family history of premature cardiovascular disease (<55 years of age for first degree male family members, <65 years for first degree female family members). Additional lifestyle-related risk factors were body mass index (BMI) >25 and sedentary lifestyle (<30 minutes of exercise on most days). Cardiovascular symptoms included chest pain, shortness of breath, palpitations, claudication, syncope, and fatigue.
Statistical analysis
Descriptive and comparative statistics were conducted. Categorical variables are presented as n/N (%) and were compared using the Pearson's chi-squared test. Continuous variables are presented as mean ± standard deviation (N) and were compared using Student's t-test. A two-tailed p-value <0.05 was considered significant for all statistical comparison. All statistical analyses were performed using STATA version 12.1 (StataCorp LP, College Station, TX).
Role of the funding source
The design and conduct of the study, including survey collection and management, were funded by Abbott Vascular. Data analysis was performed through Mount Sinai.
Results
Study population
In this survey, 2,946 female patients were screened between January 2010 and January 2012. The mean age of the population was 51 ± 13.6 years (Table 1); 49.0% of women were postmenopausal per self-report and 23.6% of these patients were on hormone replacement therapy. Three hundred and eighty patients (12.9%) had a history of APO with gestational diabetes (9.0%), gestational hypertension (9.9%), and/or preeclampsia/eclampsia (4.5%); 108 of the 380 APO patients (28.4%) had a history of two or all three of these gestational risks. Compared with patients without APO, the APO group was younger (49.4 ± 9.7 vs. 51.0 ± 14.1, p = 0.04). No differences in the proportion of postmenopausal patients were noted 49% versus 45%, (p = 0.11). Tables 1 and 2 show the overall prevalence of cardiovascular risk factors and symptoms and the differences in frequencies between patients with and without APO.
Patient Characteristics and Cardiovascular Risk Factors
SI conversions: To convert cholesterol to mmol/L, multiply by 0.0259.
APO, adverse pregnancy outcome; BMI, body mass index; BP, blood pressure; CAD, coronary artery disease; HRT, hormone replacement therapy; MI, myocardial infarction; TIA, transient ischemic attack.
Prevalence of Cardiovascular Symptoms
Including chest, jaw, shoulder, and neck discomfort.
Overall prevalence of cardiovascular risk factors and symptoms
The prevalence of cardiovascular risk factors was high with 86.0% of patients reporting at least one cardiovascular risk factor (Fig. 1A). In particular, lifestyle-related risk factors were common, with one of every four patients reporting being overweight, and 50% reporting a sedentary lifestyle (Table 1). Overall, 40.1% of the patient population reported any of the following symptoms, including exertional chest pain (7.7%), chest pain at rest (8.7%), shortness of breath (14.1%), palpitations (13.0%), claudication/leg pain on walking (9.4%), and syncope/unexplained fainting (1.7%) as shown in Table 2. Of all, 21.1% of patients reported fatigue.
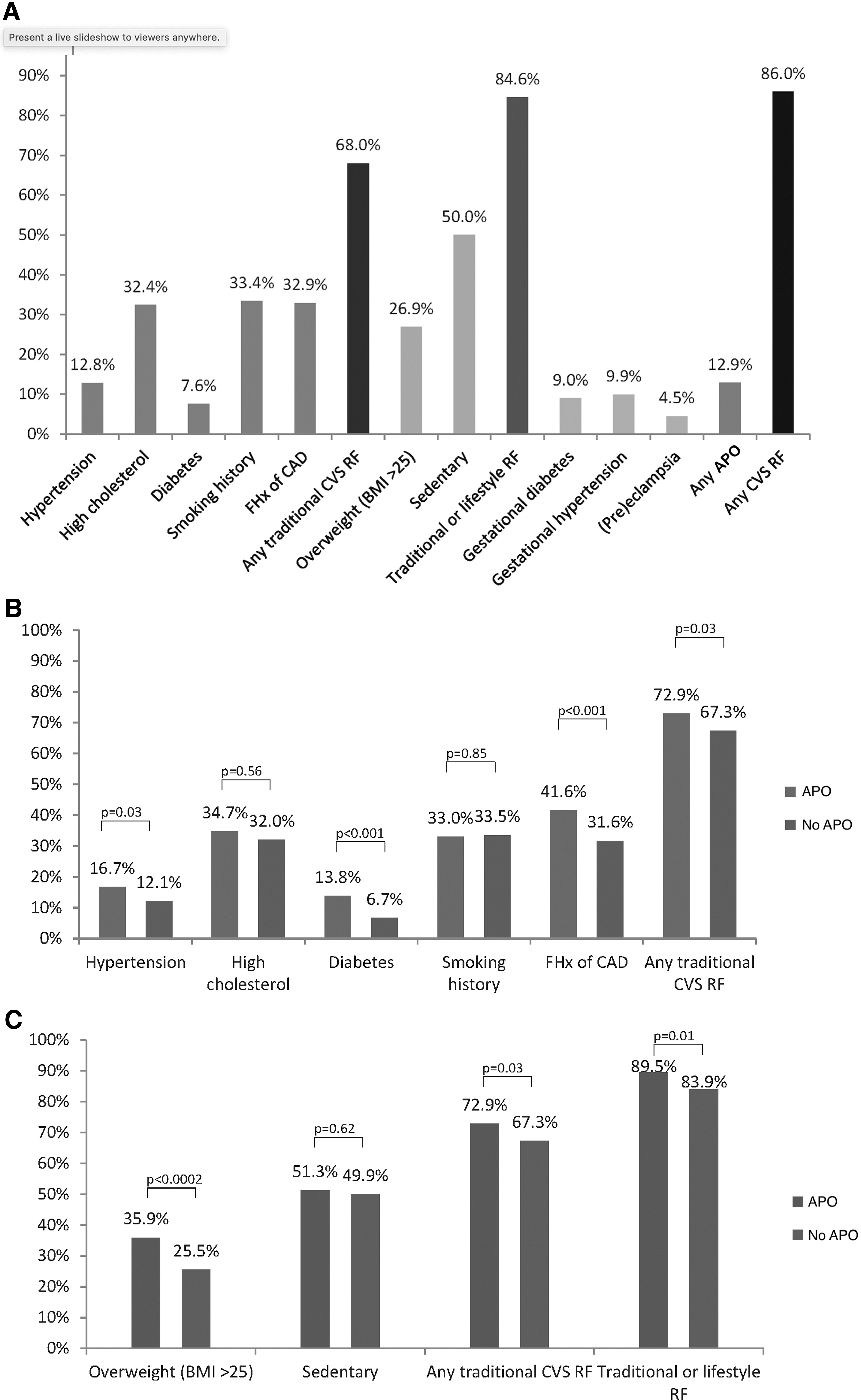
The APO group was more likely to have risk factors such as elevated BMI, diabetes mellitus, prehypertension, hypertension, and family history of premature cardiovascular disease, compared with the no APO group (Table 1). Traditional and lifestyle-related risk factors such as hypertension, high cholesterol, and sedentary status were both increased among APO patients (any traditional risk factor, 72.9% versus 67.3%, p < 0.001; any traditional or lifestyle-related risk factor, 89.5% versus 83.9%, p = 0.002, Fig. 1B, C). Of note, the prevalence of current cigarette smoking was 9.5% versus 8.7%, (p = 0.57) and sedentary lifestyle was 51.3% versus 49.9%, (p = 0.62) regardless of a history of APO. More patients in the APO group experienced cardiovascular symptoms compared to the no APO group (45.5% vs. 39.3%, p = 0.02).
Awareness of cardiovascular risk factors
A significant number of patients reported that they “did not know” whether they had a history of various cardiovascular risk factors (Table 1 and Fig. 2A). High proportions of patients in both APO and no APO groups were unaware of their blood pressure (17.0% vs. 18.6%, p < 0.001), cholesterol levels (31.7% vs. 32.0%, p = 0.56), diabetes status (18.5% vs. 17.8%, p < 0.001), and that their BMI was in the overweight range (43.9% vs. 49.7%, p < 0.001; Fig. 2B).
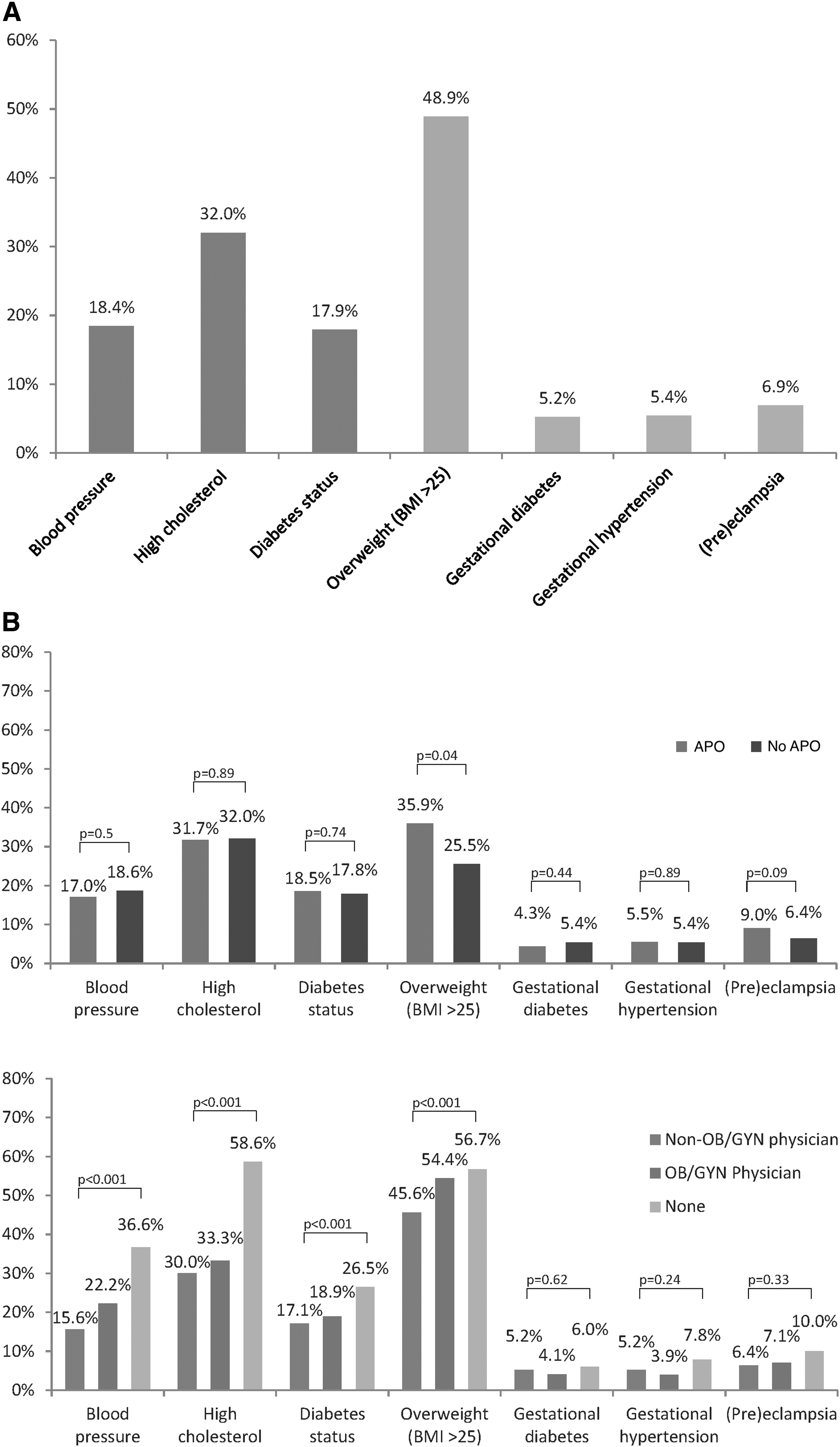
With respect to nonpregnancy-related cardiovascular risk factors, patients who reported having a non-OB/GYN physician primary health care provider were most likely to be aware of their risks, followed by patients with an OB/GYN specialist providing primary care, and then patients with no primary health care provider (Fig. 2C).
Health care providers and referral for additional/specialized care
One hundred and seventy women (7.0%) surveyed in the study did not have a primary care provider. For an additional 450 women (17.6%), their OB/GYN specialist was also their primary care provider. 1,412 (76.3%) had a non-OB/GYN primary care provider (Table 3). There were no significant differences between the APO and no APO groups regarding the primary health care provider.
Primary Care Providers and Referrals to Additional Health Care Providers
OB/GYN, obstetrics/gynecology.
Overall, 20.9% of patients were referred for further care (Table 3). The majority of the referrals were to primary care physicians 42% (142/338) and to cardiologists 28.1% (95/338). The APO group were more likely to be referred than the no APO group (28.7% vs. 19.6%, p = 0.002).
Discussion
The main findings of this study are highlighted in the Central Illustration and include (1) 86.0% of community patients attending OB/GYN clinics presented with some risk factor for cardiovascular disease and 40.1% presented with at least one cardiovascular symptom. While patients with APO were more likely to have cardiovascular risk factors and symptoms than patients with no-APO, the prevalence was high in both groups underscoring the potential benefit of conducting early screening. (2) There was a significant lack of awareness regarding cardiovascular risk factors among women surveyed. (3) Participants with no primary care provider other than their OB/GYN specialist or with no primary care physician at all demonstrated the lowest levels of awareness, suggesting possible underdiagnosis and undertreatment of cardiovascular risk factors. (4) Despite the high prevalence of risk factors, only one-fifth of those screened were referred to an additional health care provider, most commonly, a primary care physician or a cardiologist.
The current study demonstrated that OB/GYN office screening using a focused survey for cardiovascular risk factors was feasible and could be an important tool for early cardiovascular risk assessment for a significant number of women.
APO and cardiovascular risk
Hypertensive disorders of pregnancy and pregnancy-induced diabetes mellitus are associated with increased long-term cardiovascular risk. 7,8 Preeclampsia affects 3%-5% of all pregnancies worldwide. 9 In our study, 12.9% of subjects had reported an APO, 4.5% preeclampsia, and 9% reported gestational diabetes. Preeclampsia and eclampsia have been shown to be associated with increased risk of cardiovascular disease (hazard ratio [HR] 2.28), cerebrovascular disease (HR 1.76), and hypertension (HR 3.13). 8 Preeclampsia also increases long-term risk for heart failure (relative risk [RR] 2.11) and cardiovascular death (RR 2.10). 10 More recently, there has been increasing data linking other APO such as preterm birth and intrauterine growth restriction with adverse cardiovascular outcomes, after adjusting for lifestyle and other traditional cardiac risk factors. 11 Hypertensive disorders of pregnancy and premature ovarian insufficiency are risk enhancing factors in the 2018 ACC/AHA guidelines. 12,13
Current guideline recommendations
The 2011 American Heart Association guidelines recommend that physicians obtain a pregnancy history and consider both preeclampsia and gestational diabetes as risk factors for later life maternal cardiovascular disease. 14 The guidelines also recommend appropriate postpartum referral by the obstetrician to a primary care physician or cardiologist, for careful risk factor screening, monitoring, and treatment. 14 Despite this, our study demonstrated that patients with APO surveyed here were no more likely to have a non-OB/GYN primary care physician than patients with no APO.
Patient awareness of cardiovascular risks was equally suboptimal in patients with and without APO, with almost one in five patients unaware of their blood pressure or diabetes status in each group. The prevalence of modifiable lifestyle risk factors such as current smoking and sedentary lifestyle were also similar in both groups, despite guideline recommendation for aggressive lifestyle interventions in patients with APO. Our data suggest the need for improved referral, education, and long-term care of this high-risk group. After this pilot study was completed, a recent presidential advisory statement endorsed by the American Heart Association and the American College of Obstetrics and Gynecology further stressed the importance of such collaborative initiatives between OB/GYN specialists and cardiologist. 15
While specific cardiovascular screening in OB/GYN clinics may improve early diagnosis and treatment in high-risk patients with history of APO, the high prevalence of risk factors and symptoms observed in our study suggests that more routine screening of women may be warranted. In our study, 20.9% of patients were subsequently referred to another care provider, and 28.1% of these patients were referred to a cardiologist. In the context of the high prevalence of cardiac risk factors (86.0%) and symptoms (40.1%), this referral rate seems inadequate. This may be explained by the lack of specific recommendations included with our survey; thus guidelines on “triggers” or thresholds for subsequent referral may improve referrals. In addition, integration of risk factor triggers to prompt that recommendation for lipid and hypertension screening into existing electronic medical record systems would assist in risk modification. Standardized use of automated cardiac risk assessment using the contemporary Pooled Cohort Equation should also be routine and use in conjunction with data collected on pregnancy complications. This would translate data obtained from screening into active risk modification efforts.
Gender disparities in the delivery of health care for U.S. women have long been reported. Previous studies have shown that women are less likely to receive preventive recommendations, such as lipid-lowering therapy, aspirin, and lifestyle advice compared to men. 16,17 Hypertensive women are less likely to achieve blood pressure control. 18 Historically, primary care physicians have been poorly informed regarding the significant gender differences in coronary heart disease and gender disparities in cardiac care. 19 Although national guidelines for the prevention of coronary heart disease in women have since been published, there is limited information on their uptake in routine clinical practice. 2 The low rates of patient awareness in our study suggest a clear need for increased efforts to improve patient education and health care delivery for female patients.
Primary care at OB/GYN clinics
Multiple studies have sought to assess how effectively OB/GYNs provide primary care services. A large database study of well-woman preventive care visits noted that almost half of all women's prevention visits occurred with OB/GYNs; however, the primary focus of these visits was reproductive health based. 20 Conversely, in a study by Rosser and colleagues of real-life U.S. clinical practices, 66.8% of women surveyed (n = 498) reported that their OB/GYN did not discuss their heart health. 21 Additional studies have shown disparate rates of cardiovascular risk screening between OB/GYNs and primary care providers. 22
Consistent with these findings, our study also showed that patients with no primary care physician other than their OB/GYN physician had lower awareness of their risk factors. In our study, almost 75% of patients had a non-OB/GYN physician, which may reflect an improvement over time compared to older studies. In addition, survey data also demonstrate suboptimal recognition of adverse pregnancy conditions as a cardiovascular risk factor among general providers and obstetricians. 22 Further education will help across a broad range of specialties and levels of care.
Previous research has shown that young, minority women are more likely to visit an OB/GYN as their primary care provider. 6 Yet, only 20% of these women reported that their OB/GYN physician cared for all of their health needs, and only 33% remembered discussing cardiovascular disease with their OB/GYN physician. 6 While we did not collect ethnicity data, these studies in concert with our findings further emphasize the potential for improvement through the mobilization of OB/GYN practices to identify women at risk.
Strengths and limitations
Our study demonstrated that a focused survey that takes less than 10 minutes, which was easily be completed by the patient in the waiting room, identified cardiovascular disease risk factors. Because many women have no primary care provider other than their OB/GYN physician, these outpatient facilities may present an opportunity to identify risk factors for cardiovascular disease and refer to the appropriate specialist.
Our analyses were restricted to women who visited one of the participating outpatient OB/GYN clinics. As with any survey, our study is subject to ascertainment bias as well as possible underreporting related to subject recall bias. Demographic information concerning ethnic background, socioeconomic status, and occupation were not collected. We did not assess for premature ovarian insufficiency. We did not assess for intrauterine growth restriction or preterm delivery history. The reason for the OB/GYN clinic visit was not recorded. This could underestimate prevalence of screening, which for the most part is addressed during an annual visit in most OB/GYN practices. The proportion of women who actually completed the questionnaire out of all those in which it was given to is unknown and a potential source of bias as patients with symptoms may have been more likely to respond. In addition, women presenting to an OB/GYN clinic may not be representative of a general population sample as these patients may be seeking specialized care for specific gynecologic conditions. Despite these limitations, our data suggest that cardiovascular screening in an outpatient OB/GYN setting using our simple one-page questionnaire may lead to improvement of the diagnosis, education, and management of cardiovascular risk factors for women at risk.
Conclusions
Cardiovascular risk factors and symptoms were prevalent among women receiving routine care in the outpatient OB/GYN clinics we surveyed, regardless of a history of APO. Many of the women were unaware of their cardiovascular risk factors and the importance of additional heart health screening and management. We found a need for improved screening, and we demonstrated the feasibility of cardiovascular risk assessment in the setting of our participatory community-based OB/GYN clinics. Improved screening may enhance the early detection of cardiovascular issues in women and aid in the timely delivery of prevention and education among women.
Footnotes
Acknowledgments
We acknowledge and thank Karen Stark, Tracy Moroney, Shadi Shalakhti, Shazib Khawaja, Mark Campbell, Ollie Harper, Jayne King, Caitlyn Geisler, Birgit Vogel, Vijay Kunadian, Sameer Bansilal, Samantha Sartori, Raj Vadde, Melissa Aquino, Michele A. Couri, Beth R. Malasky, Ali R. Homayuni, Kleanthis Theodoropoulos, and Stacey Prentis for contributing patients to the study and for assistance with collecting data for analysis.
Author Disclosure Statement
Roxana Mehran has received Institutional Research Grant support from The Medicines Company, Bristol-Myers Squibb/Sanofi-Aventis, and Lilly/Daiichi Sankyo; consulting fees from Abbott Vascular, AstraZeneca, Boston Scientific, Covidien, CSL Behring, Janssen Pharmaceuticals, Maya Medical, Merck, Regado Biosciences, and Sanofi-Aventis. Johnson & Johnson and Regado serve on the advisory board for Covidien, Janssen Pharmaceuticals, and Sanofi-Aventis and an equity/shareholder for Endothelix, Inc., Jerri A. Johnson is an employee of Abbott Vascular. The other authors have no disclosures. Robert A. Wild has received Institutional Research Grant support from Amgen, AbbVie, Esperion, and NICHD, not related to this investigation.
Funding Information
No funding was received for this article.
Appendix
Enrolling Site
| Kimberly Skelding | Geisinger Medical Center, Danville, PA |
| Suhdir Mungee | HeartCare Midwest, Peoria, IL |
| Karen Stark | Scottsdale Health, Scottsdale, AZ |
| David Dobies and Kimberly Barber | Genesys Regional Medical Center, Grand Blanc, MI |
| Tracey Moroney | John C Lincoln System, Phoenix, AZ |
| Lynn Thomas | Sanford Hospital, Sioux Falls, SD |
| Shadi Shalakhati | Methodist University Hospital, Memphis, TN |
| Ali Homayuni | Cardiovascular Institute of Mississippi, McComb, MS |
| Shazib Khawaja | Tanner Heart Center, Carrollton, GA |
| Stacy Prentiss | Good Samaritan Hospital, Downers Grove, IL |
| Beth Malasky | Idaho Heart Care, Boise, ID |
| Bina Ahmed | University of New Mexico, Albuquerque, NM |
| Mark Campbell | Wesley Medical Center, Hattiesburg, MS |
| Ollie Harper | Jackson State University, Jackson, MS |
| Jayne King | St David's, Austin, TX |
| Caitlyn Geisler | Seton Heart Institute, Austin, TX |