
Abstract
Background:
While racial–ethnic disparities in cesarean delivery rates among nulliparous women delivering a term singleton in the vertex position (NTSV) exist, it remains unclear the extent to which potentially modifiable maternal cardiometabolic risk factors (obesity, maternal hyperglycemia and hypertensive disorders) underlie these disparities. We examined race–ethnicity and risk of NTSV cesarean deliveries and whether the associations were mediated by maternal cardiometabolic risk factors.
Materials and Methods:
A cohort study of 62,048 NTSV deliveries in Kaiser Permanente Northern California. The outcome was cesarean delivery.
Results:
Black, Asian, and Hispanic women were at increased risk of having a NTSV cesarean delivery compared with White women (relative risks and 95% confidence intervals: 1.37 [1.28–1.45]; 1.11 [1.07–1.16]; 1.12 [1.07–1.16], respectively), independent of established risk factors and prenatal care utilization. The extent to which cardiometabolic risk factors mediated the associations between race–ethnicity (each group vs. White, in separate analyses) and NTSV cesarean delivery varied by race–ethnicity. Maternal overweight/obesity (body mass index ≥25.0) mediated the association between Black and Hispanic race–ethnicity and NTSV cesarean delivery (21.1% [15.8–26.4] and 24.7% [14.6–34.8, respectively), but not for Asian race. Maternal hyperglycemia (gestational diabetes mellitus or preexisting diabetes) mediated the association between Asian and Hispanic race and NTSV cesarean delivery (18.5% [9.8–27.2] and 9.8% [5.0–14.7], respectively), but not for Black race. Hypertensive disorders mediated 3.2% (0.70–5.8) of the association between Black race and cesarean delivery, but not for other race–ethnicities.
Conclusion:
Black, Asian, and Hispanic women are at increased risk for NTSV cesarean deliveries. Maternal cardiometabolic risk factors only partially mediate the associations between race–ethnicity and NSTV cesarean deliveries.
Introduction
Cesarean deliveries among low-risk women, defined as nulliparous women delivering a term singleton infant in the vertex position (referred to as NTSV), represent the category of cesarean deliveries, which might not provide medical benefit for the mother or the infant. 1 Thus, the American College of Obstetricians and Gynecologists and Healthy People 2020 both emphasize the need to lower NTSV cesarean delivery rates. 1,2 National data show that NTSV cesarean delivery rates gradually increased over time from 18.4% in 1997 to 25.8% in 2015, 3 suggesting that rates are variable and potentially modifiable.
Studies suggest there are racial–ethnic disparities in cesarean rates among NTSV deliveries, 4,5 with Black women having higher rates compared with non-Hispanic White women, 6 –8 but most previous studies were unable to evaluate other racial–ethnic groups. There is an increasing recognition of the need to reduce racial–ethnic disparities in maternity care, but to inform such strategies we must identify potentially modifiable factors contributing to these disparities. Cardiometabolic risk is defined as a cluster of modifiable risk factors, such as obesity, hyperglycemia, and hypertension that increase an individual's risk for cardiovascular disease and type 2 diabetes. 9 While there are known racial–ethnic disparities in the prevalence of maternal cardiometabolic risk factors (i.e., hyperglycemia, 10 hypertensive disorders of pregnancy, and obesity 11 ), it is unclear if cardiometabolic risk factors are on the pathway linking maternal race–ethnicity to cesarean delivery.
The overall aim of this study was to examine the associations between maternal race–ethnicity and risk of having a NTSV cesarean delivery, accounting for established risk factors, within a large racially- and ethnically diverse integrated health care delivery system. We then estimated the extent to which the associations between maternal race–ethnicity and NTSV cesarean deliveries were mediated by potentially modifiable maternal cardiometabolic risk factors.
Materials and Methods
The study setting was Kaiser Permanente Northern California (KPNC) from January 1, 2008 to December 31, 2012. During this time period, KPNC provided comprehensive medical services through 14 delivery hospitals and over 40 outpatient clinics to over 3 million members located in a 14-county region of Northern California. The demographic make-up of KPNC membership is well representative of the population living in the geographical area served by this large, integrated health care delivery system, except that the KPNC population has slightly lower representation at the extremes of income. 12 KPNC is vertically integrated and all care is provided in a closed system and captured in the electronic health record (EHR), with complete data on all weight measurements, laboratory tests, and medications. Thus, our access to clinical data (not claims data) in an integrated health system allows us to collect high-quality data, including physician diagnoses and medical treatments during pregnancy.
We identified 73,459 singleton live birth deliveries to nulliparous women 15–45 years of age at delivery between 2008 and 2012 at a KPNC delivery hospital. We matched the cohort to the California birth certificate record to obtain demographic information. During the study period, all live births within KPNC were linked with the California birth certificate data and records were probabilistically matched based on a variety of variables (i.e., name, date of birth, birth hospital, paternal last name). Chart review was conducted for those without a high probabilistic match and we successfully matched 98.9% of births.
NTSV cesarean delivery
Cesarean delivery was defined based on International Classification of Diseases, 9th Edition (ICD-9) codes available in the EHR: 74.xx (excluding 74.3 and 74.91) and ICD-9 diagnosis: 669.7. To restrict to NTSV deliveries we then excluded women delivering at <37 weeks' gestation (n = 5,919), multiple births (n = 614), and contraindications for a vaginal delivery, including breech, traverse, and malposition (n = 4,825). An additional 53 women were missing information on race–ethnicity leaving a final analytic cohort of n = 62,048. Cesarean deliveries identified by ICD-9 codes were then also verified against the California birth certificate record and the KPNC infant cohort database 13 (∼98.9% were validated based on at least two sources). A new operating scheduling database in 2010 allowed us to identify elective procedures as women who were scheduled according to the database. A validation of 100 randomly selected cesarean deliveries found that 95% of cases were correctly identified as elective or urgent when comparing clinical documentation with EHR data. 14 For the 36,440 deliveries occurring after 2009 (58% of the entire cohort) we were able to categorize the 9,059 cesarean deliveries as urgent or elective.
Race–ethnicity
The use of race–ethnicity as an exposure has been widely discussed in the causal inference literature. VanderWeele and Robinson 15 point out that because of the nonmanipulable nature of race–ethnicity, it is impossible to define a counterfactual framework in which a hypothetical intervention on race–ethnicity could be applied. To address this challenge, they suggest interpreting the “effect of race” as the extent to which a racial–ethnic inequality could be eliminated by intervening on a downstream risk factor that can be modified. Thus, in our study, we considered maternal race–ethnicity to represent the constellation of factors that make up the lived experience of being a woman of a certain race–ethnicity in the United States. Furthermore, we used causal mediation analysis to assess the magnitude of the disparity that would remain under an intervention on potentially modifiable cardiometabolic mediators. In accordance with such a framework, which is premised upon counterfactual manipulability of the mediator, we address the question “What would a Black woman's NTSV cesarean section risk have been had she had the same body mass index (BMI) as a White woman?” 16,17
Race–ethnicity was obtained from the EHR or the State of California birth certificate records to obtain information on self-reported maternal race and ethnicity. Maternal race and ethnicity were categorized as non-Hispanic Black, Hispanic, Asian, and Other versus non-Hispanic White (reference group, hereafter referred to as White) to be comparable to past studies of racial–ethnic differences in cesarean section rates by race–ethnicity.
Maternal cardiometabolic risk factors
Maternal hyperglycemia
We first searched the KPNC Diabetes Registry 16 to identify women with preexisting diabetes. We then searched the KPNC Gestational Diabetes Mellitus and Pregnancy Glucose Tolerance Registry, 18 which classifies women without preexisting diabetes by glucose values obtained from a 50-g glucose challenge test (hereafter referred to as the screening test); for those with an abnormal result (≥140 mg/dL), a follow-up 100-g, 3-hour oral glucose tolerance test (hereafter referred to as the diagnostic test) is undergone. At KPNC, 94% of women delivering live-born singletons undergo the recommended screening test for gestational diabetes mellitus (GDM). 18 GDM was defined as two or more oral glucose tolerance test values meeting the Carpenter and Coustan criteria 19 (fasting, 95 mg/dL; 1-hour, 180 mg/dL; 2-hour, 155 mg/dL; 3-hour, 140 mg/dL). Women with GDM were further categorized by severity: women with GDM who required medication treatment in addition to diet therapy were defined as severe GDM. For mediation analyses, women were categorized as GDM (Yes vs. No) and preexisting diabetes (Yes vs. No). We then examined any maternal hyperglycemia defined as either preexisting diabetes or GDM versus none. Among women with GDM, we explored whether severe GDM (Yes vs. No) or timing of diagnosis (<20 weeks vs. 20 weeks or later) mediated the associations.
Maternal overweight/obesity
Prepregnancy body weight was assessed by a measured weight within 12 months before pregnancy obtained from the EHR. Prepregnancy BMI was calculated as the maternal weight (kilograms) divided by height (meters) squared. BMI categories were created based on the World Health Organization International Classification. 20 For the mediation analysis, BMI was categorized as overweight or obese (≥25.0 kg/m2; Yes/No) and as obese (≥30.0 kg/m2; Yes/No) in separate analyses.
Maternal hypertensive disorders
Preexisting hypertension was based on ICD-9 codes: 642.0, 642.1, 642.2, and 642.7. Gestational hypertension was based on ICD-9 code 642.3 and 642.9 and Preeclampsia/Eclampsia was based on ICD-9 codes 642.4, 642.5, and 642.6. For mediation analysis, we examined gestational hypertension (Yes/No) and/or preeclampsia (Yes/No) versus none and preexisting hypertension (Yes/No) separately. We also examined any hypertensive disorder defined as gestational hypertension, preeclampsia, or preexisting hypertension versus none.
Other covariates and precision factors
Maternal age at delivery was extracted from the EHR. A self-administered Early Start Program Prenatal Substance Use Screening Questionnaire is completed at entry into prenatal care and recorded in the EHR, from which we obtained maternal alcohol intake, smoking, and illegal drug use during pregnancy. 21 Maternal education was obtained from the EHR and confirmed against the California birth certificate data.
Prenatal care utilization
Trimester when prenatal care was initiated was extracted from the EHR. Type of insurance coverage plan type in which patients were enrolled (private vs. MediCal) was obtained from the EHR system. Precision factors included were year of delivery and medical facility where the delivery occurred.
Statistical analysis
Overall, the crude overall proportion of NTSV cesarean deliveries was calculated by dividing the number of eligible cesarean deliveries by the total number of eligible first birth singleton live births in the vertex position during the study period. Univariable and multivariable Poisson regression with robust standard errors were used to provide crude and adjusted estimates of relative risks (RRs) and 95% confidence intervals (CIs) for NTSV cesarean delivery risk associated with risk factors. 22 RR estimates were adjusted for maternal age, education, and trimester when prenatal care initiated, insurance coverage type, alcohol, smoking, illegal drug use during pregnancy, delivery year, and medical facility to account for possible changes in the demographics and underlying risk factors for NTSV cesarean deliveries during the study period.
Mediators are variables that are on the causal pathway between an exposure and outcome variable, and explain part of the effect of an exposure on outcome. 23,24 We employed the counterfactual approach to mediation analysis proposed by VanderWeele and Vansteelandt, 24 as this method allows for the decomposition of the total effect into a direct effect (main effect of exposure on outcome not through the mediator) and the indirect effect (the effect of the exposure on the outcome through the mediator). 24,25 Furthermore, the counterfactual mediation approach allows for valid inferences under the assumptions that there are measured covariates controlling for confounding of the relationships between the (1) exposure and outcome, (2) mediator and outcome, (3) exposure and mediator, and (4) that none of the mediator–outcome confounders is affected by the exposure. 24 –26
We conducted analyses 24,25 to examine the extent to which the effect of race–ethnicity (Black vs. White; Asian vs. White; and Hispanic vs. White, etc.) on NTSV cesarean delivery is mediated by cardiometabolic risk factors. Figure 1 shows the conceptual model for our hypothesized mediation pathway. We performed our analysis according to methods developed by Valeri and VanderWeele 27 and elaborated by VanderWeele 28 to decompose the total effect of race–ethnicity on NSTV cesarean section into the effect of race–ethnicity (Black vs. White; Asian vs. White; Hispanic vs. White) mediated through a cardiometabolic risk factor (e.g., Obesity-Yes/No) (natural indirect effect) and the effect of race–ethnicity not mediated through the cardiometabolic risk factor (natural direct effect). The fraction of the total effect mediated by cardiometabolic risk factors was expressed as a percentage. We aimed to determine whether the mediating effects of cardiometabolic risk factors on the maternal race–ethnicity and NTSV cesarean delivery was independent of other variables identified as potential confounders, including socioeconomic and behavioral determinants (maternal age, education, trimester of prenatal care initiation, insurance type, smoking, alcohol, drug use) and precision factors (year of delivery and medical facility). We then performed a sensitivity analysis using a method that describes the strength of the confounder–outcome relationship and the approximate strength of the confounder–mediator relationship that, together, would be required to explain away the indirect effect. 29
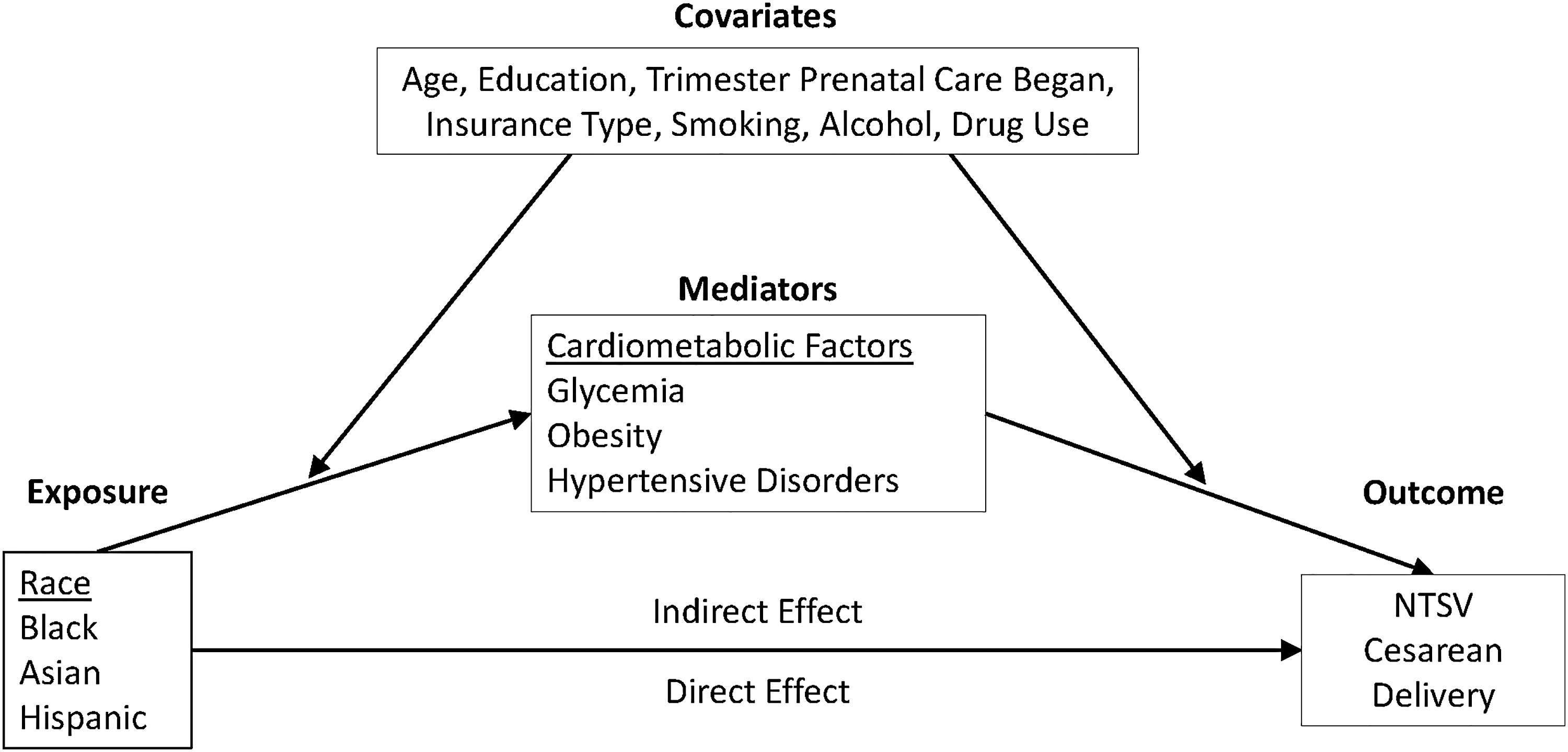
Directed acyclic graph: the concept model for the mediation analysis.
Analyses 24,25 were performed with SAS v9.4 (SAS, Cary, NC). This study was approved by the KPNC Institutional Review Board and the State of California Committee for the Protection of Human Subjects.
Results
The study population was racially- and ethnically diverse: 40.3% non-Hispanic white, 23.5% Asian/Pacific Islander, 7.3% Black, 23.4% Hispanic, and 5.5% other race–ethnicity (Table 1). Table 1 shows the characteristics of the cohort. On average, the mean age of the cohort was 28.0 (±5.9), 45.4% had college or more education, 97.5% had private medical insurance, 88% had their first prenatal visit in the first trimester, and 4.2% smoked during pregnancy. Twenty-two percent of the cohort was overweight and 16% was obese. GDM occurred in 6% of pregnancies and 27.1% of GDM women required medication and 12.8% were diagnosed before 20 weeks' gestation. 0.7% of the cohort had preexisting diabetes, 4.2% had gestational hypertension, 4.7% had preeclampsia, and 2.0% had preexisting hypertension.
Cohort Characteristics, Kaiser Permanente Northern California, 2008–2012
Assessed among the 3,734 women with gestational diabetes.
BMI, body mass index; SD, standard deviation.
Overall, the proportion of cesarean deliveries was 23.5% among our NTSV cohort. The crude NTSV cesarean delivery proportions were 22.6%, 27.3%, 25.2%, 22.2%, and 24.1% for non-Hispanic White, Black, Asian, Hispanic, and Other women, respectively (Fig. 2). For the subset with information on type of cesarean, the crude proportion of urgent NTSV cesarean delivery was 19.8%. The urgent NTSV cesarean delivery proportions were 18.4%, 24.0%, 21.8%, 18.8%, and 19.6% for non-Hispanic white, Black, Asian, Hispanic and Other women, respectively. The crude elective delivery proportion was 5.7%. The crude elective delivery proportions were 5.9%, 6.8%, 5.8%, 5.0% and 6.2% for non-Hispanic white, Black, Asian, Hispanic, and Other women, respectively (data not shown).
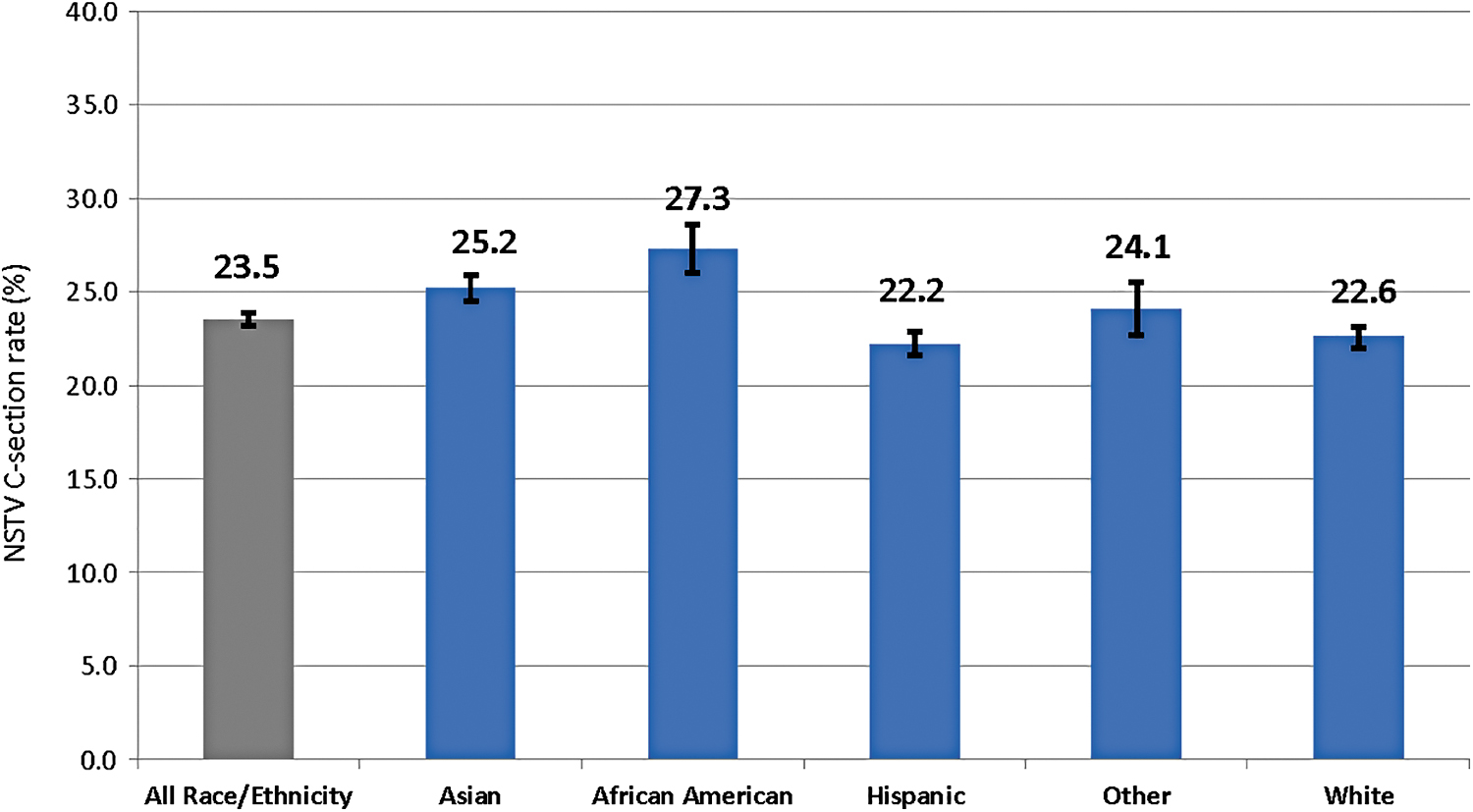
The crude proportion of nulliparous term singleton vertex cesarean deliveries by maternal race–ethnicity.
Black, Asian, and Hispanic women were at increased risk of having a NTSV cesarean delivery compared with white women (RRs and [95% CIs]: 1.37 [1.28–1.45]; 1.11 [1.07–1.16]; 1.12 [1.07–1.16], respectively), independent of established risk factors and prenatal care utilization (Table 2). Black, Asian, and Hispanic women were also at increased risk for urgent NTSV cesarean deliveries (1.44 [1.32–1.57]; 1.15 [1.09–1.22]; 1.15 [1.08–1.22]), whereas only Black women had a significant increased risk of having an elective NTSV cesarean delivery (Table 2).
Crude and Adjusted Risk Ratios for Nulliparous Term Singleton Vertex Cesarean Deliveries
Among the subset of 36,440 with information on type of cesarean delivery.
Adjusted model included all variables in this table and maternal age, maternal education, trimester when prenatal care initiated, insurance coverage type, alcohol, smoking, illegal drug use during pregnancy, delivery year, and medical facility.
We examined whether maternal cardiometabolic risk factors mediated the association between race–ethnicity (each racial–ethnic group vs. White, in separate analyses) and NTSV cesarean delivery (Table 3). Black and Hispanic race were associated with higher risk of NTSV cesarean delivery compared with White race–ethnicity, as indicated by the direct and total effects. Maternal BMI defined as either overweight (BMI ≥25.0) or obesity (BMI ≥25.0) was a mediator of the association between race–ethnicity and NTSV cesarean delivery, mediating 21%–25% among Black women and 19%–25% among Hispanic women, and maternal BMI was not a significant mediator for Asian or other racial–ethnic groups. For hyperglycemia, Asian and Other race was associated with higher risk of NTSV cesarean delivery compared with White race–ethnicity, as indicated by the direct and total effects. GDM was a significant mediator for Asian 13.7%, Hispanic 6.6%, and other racial–ethnic groups 9.3%, but was not a mediator for Black race–ethnicity Preexisting type 2 diabetes mediated 4.4% of the Hispanic race–ethnicity and NTSV cesarean delivery, but was not a mediator for other racial–ethnic groups. Any maternal hyperglycemia (GDM or preexisting diabetes) mediated the association between race–ethnicity and NTSV cesarean delivery for Asian 18.5%, Hispanic 9.8%, and other racial–ethnic groups 11.9% but not for Black women. Any hypertensive disorder (gestational hypertension, preeclampsia or preexisting hypertension) mediated just 3.2% of the association between Black race and NTSV cesarean delivery and that was driven by preexisting hypertension, 2.7%. Hypertensive disorders did not mediate associations for other racial–ethnic groups (Table 3).
Mediation Effect of Each Metabolic Risk Factor on the Association Between Race–Ethnicity a and Cesarean Delivery
Adjusted for maternal age, education, trimester of prenatal care initiation, insurance type, smoking, alcohol, drug use, and year of delivery and medical facility.
No mediation.
GDM, gestational diabetes mellitus; HTN, hypertension; RR, relative risk; CI, confidence interval.
Similar results were observed for the subset who experienced an urgent NTSV cesarean delivery (data not shown). Among women with GDM, we explored whether timing or severity of GDM further mediated associations but found no significant mediation by timing or severity (data not shown). In a sensitivity analysis, we estimated the magnitude of the unmeasured mediator-outcome confounding required to explain away the observed indirect effect (Supplementary Table S1). For example, to completely explain away the observed indirect effect of maternal obesity on the Black race and NSTV cesarean delivery estimate (1.06), an unmeasured confounder associated with both maternal obesity and NTSV cesarean with a risk ratio of ∼1.30-fold, above and beyond the measured covariates, could suffice, but weaker confounding could not. To shift the confidence interval to the null, an unmeasured confounder associated with both maternal obesity and NTSV cesarean section with approximate risk ratios of 1.26-fold, above and beyond the measured covariates, could suffice, but weaker confounding could not (Supplementary Table S1).
Discussion
In an integrated health care delivery system, where all women had access to medical care and care was delivered by the same clinical teams, we observed racial and ethnic disparities in risk of having a NTSV cesarean delivery, independent of established risk factors. Black, Hispanic, and Asian women, all had a higher risk of having a NTSV cesarean delivery even after accounting for established risk factors. We also found racial–ethnic disparities in the mediating effects of maternal cardiometabolic risk factors on the association between race–ethnicity (each racial–ethnic group vs. White, in separate analyses) and NTSV cesarean delivery. Being overweight or obese mediated 21%–25% of the association between Black and Hispanic race–ethnicity and NTSV cesarean delivery but being overweight or obese was not a significant mediator of the association between Asian race and NTSV cesarean delivery. In contrast, maternal hyperglycemia mediated 12%–18% of the association between Asian and Hispanic race–ethnicity, but maternal hyperglycemia was not a significant mediator of the association between Black race–ethnicity and NTSV cesarean delivery. Hypertensive disorders only mediated 3% of the association between Black race–ethnicity and NTSV cesarean delivery but were not significant mediators for other racial–ethnic groups.
Our finding that Black and Hispanic women are at greater risk of having a NTSV cesarean delivery is consistent with prior studies 5,30 ; however, prior studies did not observe the increased risk among Asians found in our study. A study of birth certificate data from the state of Massachusetts found an increased risk of NTSV cesarean delivery among Blacks and several subgroups of Hispanic women. 4 Our study in a large and racially ethnic diverse integrated health system was uniquely able to examine the risk of NTSV delivery among multiple racial–ethnic groups, including Asians. We found an increased risk of cesarean delivery among NTSV women among all racial–ethnic minority groups. Among the subset of our cohort with information on the type of cesarean delivery, we found that Black, Asian, and Hispanic women were all at increased risk of having an urgent delivery, which is associated with more adverse perinatal outcomes compared with elective cesarean deliveries. 31
Being overweight or obese mediated more than 20% of the association between race–ethnicity and NTSV cesarean delivery for Black and Hispanic women but was not a significant mediator for Asian women. 32 –40 Even when a BMI cutoff of 23.0 kg/m2 was used for Asian woman, as has been recommended, 41,42 BMI was not a significant mediator among Asian women (data not shown). The underlying etiology behind why increasing maternal BMI increases cesarean delivery risk is unclear, but it has been suggested that obese women may have more labor complications due to having a longer active labor phase and decreased cervical dilation rate, which may prompt providers to perform a cesarean delivery. 43,44 Unfortunately, we did not have detailed information on labor course (dilation or timing) and therefore we could not explore whether the effect that BMI had on labor course differed by race–ethnicity. In addition, while BMI is readily available in the EHR, it does not measure etiologically important measures of adiposity. Asian women have been shown to have a higher concentration of visceral adipose tissue compared with other racial–ethnic groups. 45 It is possible there are biological differences in adiposity among overweight/obese women that impacts labor course and delivery. It is also possible that when caring for women with overweight/obesity provider practice varies by race–ethnicity. Both the shared decision-making process and the patient–provider relationship may vary with and without race concordance between the patient and provider contributing to decision making. Unfortunately, we did not have information on provider practice styles and patient–provider race concordance, which may have been contributing factors.
Maternal hyperglycemia was a significant mediator of the association between Asian race and Hispanic race and NTSV cesarean delivery (18% and 12%, respectively). However, maternal hyperglycemia was not a significant mediator of the association between Black and NTSV cesarean delivery. Asian women have a higher prevalence of GDM, even at very low BMI thresholds, compared with Black or White women. 46 Hispanic women have a higher prevalence of GDM compared with Black and White women but lower than Asian women. 46 The diagnosis of high-risk conditions like diabetes and GDM may lead to provider practice style differences (e.g., provider fear of shoulder dystocia) such that women diagnosed are treated differently 47 and decisions to go to NTSV cesarean delivery made sooner. When caring for women with hyperglycemia it is again possible that provider practice style varies by race–ethnicity. There may also be racial–ethnic disparities in a patient's adherence to treatment regimens and degree of glycemic control achieved. However, among women with GDM we did not see a significant mediating effect of GDM severity (defined as requiring insulin or early diagnosis). There may also be biological differences in the etiology of maternal hyperglycemia that varies by race–ethnicity. It is increasingly recognized that there are physiological subtypes of GDM, predominant insulin sensitivity defects with higher BMI and predominant insulin secretion defects, 48 but it is currently unclear if these subtypes vary by race–ethnicity. Finally, infants of women with preexisting diabetes or GDM are more likely to have overgrowth in the insulin-sensitive tissues in the shoulder and chest leading to increases in shoulder dystocia 49 possibly impeding a vaginal delivery. The impact of GDM on fetal growth may vary by race–ethnicity.
Maternal hypertensive disorders per se were not significant mediators of the associations between race–ethnicity and NTSV cesarean delivery for Asian and Hispanic women and only mediated 3% of the association among Black women. The cluster of cardiometabolic risk factors (obesity, hyperglycemia, and hypertension) commonly occur together. However, the statistical approach used to estimate mediation only allowed us to examine one cardiometabolic risk factor at a time of the association between race–ethnicity (each group vs. White, in separate analyses) and NTSV cesarean delivery. It appears that maternal overweight/obesity (for Hispanic and Black) and hyperglycemic disorders (for Hispanic and Asian) were more significant mediators of the associations between race–ethnicity and NTSV cesarean delivery than hypertensive disorders.
Most of the racial–ethnic disparities in NTSV cesarean deliveries appear to operate through pathways other than cardiometabolic risk factors, given our observed small indirect effects in all of our analyses. This suggests that other factors were contributing to the observed racial–ethnic disparities in NTSV cesarean delivery. The decision to perform a cesarean delivery is multifactorial. One of these factors is that the obstetric care provider could be vulnerable to unconscious (implicit) racial bias regarding treatment decisions; this bias has been shown to exist in other areas even when providers do not portray conscious (explicit) bias. 32 Patients, themselves, may have fears or biases about perceived risk to themselves or their baby, which may influence their decision making. Perceived racism and discrimination can negatively impact communication and may impact the quality of care received, especially among Black women. 50 Unfortunately, our study relied on EHR data and was unable to assess patient-reported experiences with their prenatal care. There may also be racial–ethnic differences in biological risk factors, such as placental functioning, 33 –35 the shape of the pelvis, 36,37 hormonal factors impacting labor duration, 38 risk of “nonreassuring fetal testing,” 39 and underlying maternal life stress. 40 We found possible racial–ethnic disparities in the mediating effects of cardiometabolic risk factors on the association between race–ethnicity and NTSV cesarean delivery. Future studies are needed to quantify other potential mediators of the associations between maternal race–ethnicity and NTSV cesarean delivery.
The strengths of this study include the large racially and ethnically diverse population of women, the integrated health care delivery system, which ensures access to medical care, care delivery by the same clinical team, and the high-quality EHR data. This enabled us to examine the mediating effects of maternal cardiometabolic risk on the associations between race–ethnicity and NTSV cesarean deliveries. We found associations were similar among women undergoing urgent cesarean delivery, for the subset of our cohort with information on the type of cesarean section.
However, the study also had several limitations. We lacked information on provider and patient shared decision making for cesarean delivery and information on labor course and characteristics. We categorized all Asian women into one category, but our Asian population included subgroups of Asian women from India, China, Japan, Korea, and Southeast Asia. We know that there are variations in Asian subgroups with respect to culture, socioeconomic status, health status, and GDM risk and there may have been variations in the mediating effects of GDM on race–ethnicity and risk of cesarean delivery as well. 10 We defined race–ethnicity based on self-reported data in the medical chart, however the construct of race–ethnicity is difficult to define and likely encompasses differences in cultural factors and lived experiences, including structural racism, perceived discrimination, stress, as well as dietary preferences more than any biological differences, and we were unable to assess these cultural differences. While we recognize several of the covariates (e.g., education, Medicaid status, smoking, etc.) included in our models may be part of the total causal effect of race–ethnicity resulting from the experience of structural racism, we aimed to determine if the observed racial–ethnic disparities were mediated by cardiometabolic risk factors independent of these other socioeconomic and behavioral determinants. Also, by focusing on the potentially modifiable outcome of NTSV, we likely underestimated some of the “total effect” of race–ethnicity on cesarean deliveries overall, since racial–ethnic minority women have higher rates of preterm birth, 51 which would exclude them from the NTSV cesarean definition. Finally, our sensitivity analysis showed that it is possible that the mediating effects we observed for maternal BMI, hyperglycemia, and hypertensive disorders could be explained by unmeasured confounding.
Conclusion
Potentially modifiable maternal cardiometabolic factors mediated some of the association between race–ethnicity and NTSV cesarean delivery and to varying degrees depending on race–ethnicity. This highlights the importance of optimizing care among reproductive-aged women to improve maternal metabolic risk profile among women entering pregnancy. However, further understanding how maternal race–ethnicity influences the complex decision-making processes that take place in clinical care is critical to reduce the disparities observed in cesarean rates among low-risk women in an integrated health care delivery system. Even after controlling for the many known risk factors and prenatal care utilization, we still could not account for the observed racial–ethnic disparities. Future work needs to clarify the role of provider practice style (i.e., provider attitudes and behaviors), patient factors (i.e., tolerance for labor), and the patient–provider interactions (i.e., implicit bias and race concordance) to further elucidate the reasons for the unexplained racial–ethnic disparities in cesarean deliveries among low-risk NTSV deliveries.
Footnotes
Author Contributions
M.M.H. conceptualized and designed the analysis, obtained funding, and drafted the article. F.X. contributed to acquisition and interpretation of data analyses. S.B.S. contributed to the critical revision of the article. C.P.Q. contributed to the data analysis and critical revision of the article. T.A.F. contributed to the study design, interpretation of the data analyses, and critical revision of the article. M.M.H. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Kaiser Permanente Health Policy and Disparities Research Program grant to Dr. M.M.H.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.