
Abstract
Background:
Understanding reasons for birth control method choice may inform interventions that help young women choose the best method for them. The purpose of this study was to examine why young women in the general population select their method of contraception.
Methods:
An online survey was advertised through social media in 2017. After consenting, participants were gated through questions that ensured they were female, within the age range (16–25 years old), lived in the 50 U.S. states, and using intrauterine devices (IUDs), hormonal birth control, or barrier methods specified in the survey. Surveys with incompatible responses were excluded. Satisfaction, plans to discontinue, and primary reason for using current contraceptive method were examined and compared by contraception types using chi-square analyses. Multivariable binary logistic regression was used to examine satisfaction between contraceptive methods and races/ethnicities.
Results:
A total of 2632 responses were included. A high frequency of women using less effective methods (48.6% of nonhormonal birth control) chose them primarily to prevent pregnancy (20.6% of Copper T IUD, 23.0% of hormonal IUD, and 30.9% of Mirena IUD users), while other more effective birth control methods were often chosen primarily for other reasons. Recommendations from family or friends (14.6%) were used by some to make their contraception decision. Black respondents were less likely and Hispanic respondents were more likely to be satisfied with their birth control compared to white women.
Conclusion:
Providers should consider that their young patients may want to better understand benefits and side effects of their birth control outside of pregnancy prevention. Furthermore, young women may utilize their friends and family to make their contraceptive choice, which should be taken into consideration when counseling patients.
Introduction
The unintended pregnancy rate in the United States has been decreasing, but in 2011, 45% of all pregnancies were unintended with the highest proportion occurring in women 15–24 years of age, with inconsistent use of contraception as well as lack of contraceptive use responsible for the majority. 1,2 Long-acting reversible contraceptive (LARC) methods, including intrauterine devices (IUDs) and the implant, are safe and effective birth control methods that have increased slowly in popularity among U.S. females 15–44 years of age. 3 Previous versions of IUDs, such as the Dalkon Shield, were associated with higher risk of pelvic inflammatory disease. 4 Currently available IUDs, however, are safe and effective, even among adolescent patients. 5 –7 Despite proven safety, providers and patients have been slow to adopt these methods as a first line of contraception. The National Survey of Family Growth indicated that IUD use in the United States increased from 8.5% to 11.6% (p < 0.01) and implant use increased from 7.7% to 10.3% (p < 0.05) between 2009 and 2012. 3 Between 2013 and 2015, 2.1% of 15–19 year olds and 11.5% of 20–24 year olds were using a LARC method. 8
Despite increasing rates of LARC use in young, nulliparous patients, the adolescent population continues to utilize other less effective methods such as male condoms, withdrawal, and oral contraceptive pills. 3 Although condoms are important to preventing sexually transmitted infections and should be used during every sexual encounter in combination with other birth control methods, they are not as effective at preventing pregnancy as LARC. It is unfortunate that LARC use is low, particularly among young women, as those methods are more effective at preventing unwanted pregnancies and have higher continuation rates compared with other non-LARC methods. 9 –11 Studies that assessed satisfaction and continuation of LARC methods report high levels of satisfaction and continuation rates among all age groups. 10 While satisfaction with birth control methods has been evaluated, most studies include it as part of a larger clinical study in a well-controlled clinical environment. Less is known about satisfaction in the population of young women who are using birth control outside of clinical studies.
Furthermore, satisfaction with birth control methods is rarely examined beyond asking the patient how satisfied they are with their birth control method. It is also important to understand (1) why a woman chose to use her current method of birth control, (2) reasons for feelings of dissatisfaction, and (3) whether a woman intends to discontinue her method of birth control in the future and the reasons why. Understanding reasons for satisfaction and dissatisfaction with LARC methods will allow providers to counsel their patients more effectively through helping providers better understand their patients' motivations for choosing their birth control method. The purpose of this study is to examine reasons young women (16–25 years old) choose their method of birth control, reasons for dissatisfaction with their birth control method, and why they intend to discontinue their birth control method.
Methods
An online survey was developed using the SurveyMonkey Platinum platform to measure contraception users' satisfaction with their primary method of birth control, reasons for choosing their method of birth control, and reasons for dissatisfaction with it. The SurveyMonkey platform used allowed for complex skip patterns and word substitutions in questions based on previous responses. Contraception users were recruited through advertisements posted on Facebook, Instagram, SnapChat, Reddit, GoogleAds, and Twitter between April 21, 2017, and July 28, 2017. Recruitment advertisements were focused on IUD users (Supplementary Fig. S1). Potential participants accessed the survey through the link provided. Participants could not use the same internet protocol (IP) address to take the survey more than one time, and similar IP addresses to those that had already taken the survey were also excluded. IP addresses were not recorded with the survey responses to maintain confidentiality. Participants who chose to leave their e-mail address after completing the survey were compensated with a code for a $5 Amazon gift certificate. E-mail addresses could not be linked to responses. No e-mail address was compensated more than one time. The University of Texas Medical Branch Institutional Review Board approved this study.
First, participants viewed the consent form, and were excluded if they indicated that they did not want to participate in the study (n = 36). Due to lack of consent, we were unable collect further information about nonconsenters. The survey included gated measures, which excluded the following: males (n = 168), not within the age range (16–25 years old, n = 136), who did not live in the 50 U.S. states or DC (n = 23), and women not using IUDs, hormonal birth control, or barrier methods specified in the survey (n = 26). The age range of 16–25 years was selected as this group has a high rate of unintended pregnancies, and thus are an important target for increasing the use and continuation of contraception. We also excluded respondents who had incompatible responses for this study (n = 352). For example, those who indicated that they were currently 16 years old, but who also responded that they had sex for the first time after the age of 16.
Analyses of the resulting data were stratified into five groups of contraception users, including hormonal contraception (oral birth control pills, the birth control implant, the birth control shot, the birth control patch, or the vaginal ring), Copper T (CuT) IUD users, levonorgestrel intrauterine systems (hormonal IUD group included Skyla, Liletta, or Kyleena users), Mirena users, and nonhormonal contraception (cervical cap, a diaphragm, condoms only, the sponge, or spermicide). Mirena was included as a separate method because it is the only hormonal IUD that has been approved by the Food and Drug Administration (FDA) for the treatment of heavy menstrual bleeding, and thus could have biased the responses if grouped with other levonorgestrel IUD user responses. The birth control implant was included in the hormonal contraception group because of its low frequency in this sample (16.2%).
The online survey included standard demographic questions, including race/ethnicity, age, state of residence, education level, and household income. For race/ethnicity, which was included in the survey as an item with multiple possible responses, all participants who reported “Hispanic” were included as Hispanics. We categorized Asian/Pacific Islander, biracial, and all other reported race/ethnicities in the “other” category.
Participants were also asked to describe their current relationship status and how long respondents had been in their current relationship, if they were in one. In addition to including common options, respondents could specify their relationship type by selecting “other” and typing in their response. Length of relationship was categorized as “less than 1 year,” “1–2 years,” and “3+ years.” Missing items were not included in the analyses. However, participants were included for all items that they responded to.
Items about sexual behavior were also included to provide more context on the respondents. Items focused on sexual behavior included the following: whether participants had ever had vaginal sex, age at first sex (oral, anal, or vaginal), and number of lifetime male sexual partners. All questions about sexual behavior could be skipped by respondents. Missing responses to the question on age at first sex were combined with the “never had sex” response. Responses of “never had sex” and “1 partner” were collapsed for number of lifetime male sexual partners to improve ability to compare categories, as there were very few who reported they had never had sex.
Questions about gravidity and health conditions were also included. Respondents who reported that they never had vaginal sex skipped the question about gravidity and were recorded as zero pregnancies. For health conditions, participants had the option of selecting 1 of 15 relatively common health conditions in response to the question, “Has a doctor ever diagnosed you with any of the following conditions?” Health conditions that were included on the survey were as follows: obesity, cancer, type I diabetes, type II diabetes, chronic fatigue syndrome, immunosuppressed, hypertension, anxiety, kidney disease, anemia, fibromyalgia, migraine headaches, HIV positive, depression, and autoimmune disease. In addition to being able to select that they had not ever been diagnosed with any of the conditions included in the survey, they could also specify “other” conditions in a free-text box after selecting “other.” Participants who did not respond to this question were considered to have no health conditions.
Responses to questions about satisfaction, plans to discontinue current contraceptive method, and primary reason for using current contraceptive method were examined. Primary reason for using birth control included 16 preselected responses drawn from the literature, and an “other” response with a free-text box that prompted respondents to specify their primary reason. 12 –17 We also included “my mother recommended it” because we wanted to know whether mothers potentially played a strong role in birth control choice. Respondents could only select one response to this question. After listing their primary reason, respondents could then list other reasons they decided to use their current birth control method, including the same possible responses as in the previous question. Respondents could skip questions about why they chose their current method. Respondents were asked how satisfied they are with their current birth control method. The responses included a 5-point Likert scale, from “Very satisfied” to “Very dissatisfied.” Those who responded that they were “Very satisfied” or “Satisfied” skipped the question, “Why aren't you satisfied with {{Q7}}? (Check all that apply.)” Participants could choose 1 or more responses from a list of 15 or select “other” and include their response in a free-text box. Respondents could not move forward until they responded to the satisfaction question.
All respondents were asked how likely they were to replace their current method with a different type of birth control method in the next 1–2 months. Responses consisted of a 5-point Likert scale that ranged from “Very likely” to “Very unlikely.” Those who responded “Very likely” and “Likely” were asked about their reason for wanting to discontinue. The other respondents were then asked how likely it would be for them to replace their current method with a different type of birth control in the next year. Responses consisted of a 5-point Likert scale that ranged from “Very likely” to “Very unlikely.” Those who responded “Very likely” and “Likely” were asked about their reason for wanting to discontinue. For reasons related to discontinuation, participants could select more than one response, and could enter a reason in a free-text box if they selected “other.”
Statistical analyses
Characteristics were compared by contraception group using chi-square tests. We did not use Exact tests where cell sizes were <5. However, as a sensitivity analysis, we collapsed responses with cell sizes <5 with similar responses, such as “very likely” and “likely.” All associations between categorical variables were conducted using chi-square tests. Fisher's exact tests were used to confirm chi-square tests for any categorical variable, including cell counts <5. Multivariable logistic regression models were used to examine the association between contraception group and satisfaction after controlling for age and race/ethnicity. All analyses were conducted using SAS statistical software, version 9.4 (Cary, NC).
Results
Respondents resided in all 50 U.S. states (Supplementary Fig. S2). This sample consisted of 19% Hispanic, 68% non-Hispanic white, 8% black, and 4% other race/ethnicity females (Table 1). Six percent were 16–17 year olds, 50% 18–21 year olds, and 44% 22–25 year olds. Respondents were highly educated, with 66% educated beyond high school. Close to two-thirds were currently attending school, with 50.2% attending college and 16.6% attending high school (not shown in table). Most were in a relationship with a partner whom they were not living with, followed by those who lived with a partner. Most (62%) had been in their current relationship for 1–2 years. Most respondents reported having had vaginal sex (93%). Frequencies varied by birth control method, with 99% of nonhormonal birth control users reporting they ever had vaginal sex and 86% of hormonal birth control users reporting they ever had vaginal sex. Age at first sex of any type also varied according to current birth control method. Fifty-nine percent of nonhormonal birth control users reported having sex between 14 and 17 years of age, while 31% of hormonal IUD users reported their first sexual encounter during the same age interval.
Characteristics of Internet Sample (n = 2632)
p-value confirmed with Fisher's exact test.
IUD, intrauterine device.
Fifty-eight percent of hormonal contraception users reported oral birth control pills as their primary contraception method (Table 2). Close to 21% of the sample were CuT IUD users, while 27% were hormonal IUD users. Mirena users made up 13% of the sample, and 23% were nonhormonal birth control users. More than 90% nonhormonal birth control users used condoms only as their primary form of birth control.
Birth Control Method (n = 2632)
Bolded items are a % of the total sample, and types of birth control are a % of preceding bolded item.
When asked about the primary reason for choosing their current method of birth control, 32% of all respondents reported they wanted to prevent pregnancy. In total, 30 responses were missing and 11 cited other reasons beyond those that could be selected. We found that there were differences in the frequency of responses (p < 0.001) by method. While 48.6% of nonhormonal birth control users and 42.2% of hormonal birth control users reported that they wanted to prevent pregnancy, this reason was cited by only 20.6% of CuT IUD users, 23.0% of hormonal IUD users, and 30.9% of Mirena IUD users (Fig. 1). For CuT IUD users, they most frequently wanted to improve sexual relationships with their partner (26.6%). Improving sexual relationships was also important to many women who used hormonal IUDs and Mirena (11.4% and 14.6%, respectively). Having a recommendation from family or friend or hearing good things about their primary form of contraception was listed as a primary reason for choosing their method for 14.6% of all respondents. This was the primary reason mentioned by 20.4% of CuT IUD users, 17.8% of hormonal IUD users, and 12% of Mirena users. Doctor's recommendation was reported as the primary reason for choosing their birth control for only 5% of the sample. Of those who typed in reasons, six hormonal birth control users, two CuT IUD users, one hormonal IUD user, and two Mirena users had other reasons. Primary reasons in free-text boxes included the following: would forget to take a pill every day, health reasons, sexual relationships not the main reason, no hormones, protect against sexually transmitted infections (STIs), severe premenstrual dysphoric disorder (PMDD) treatment, wanted to regulate their period, felt that politics would limit birth control choice, and recommended by her boyfriend.
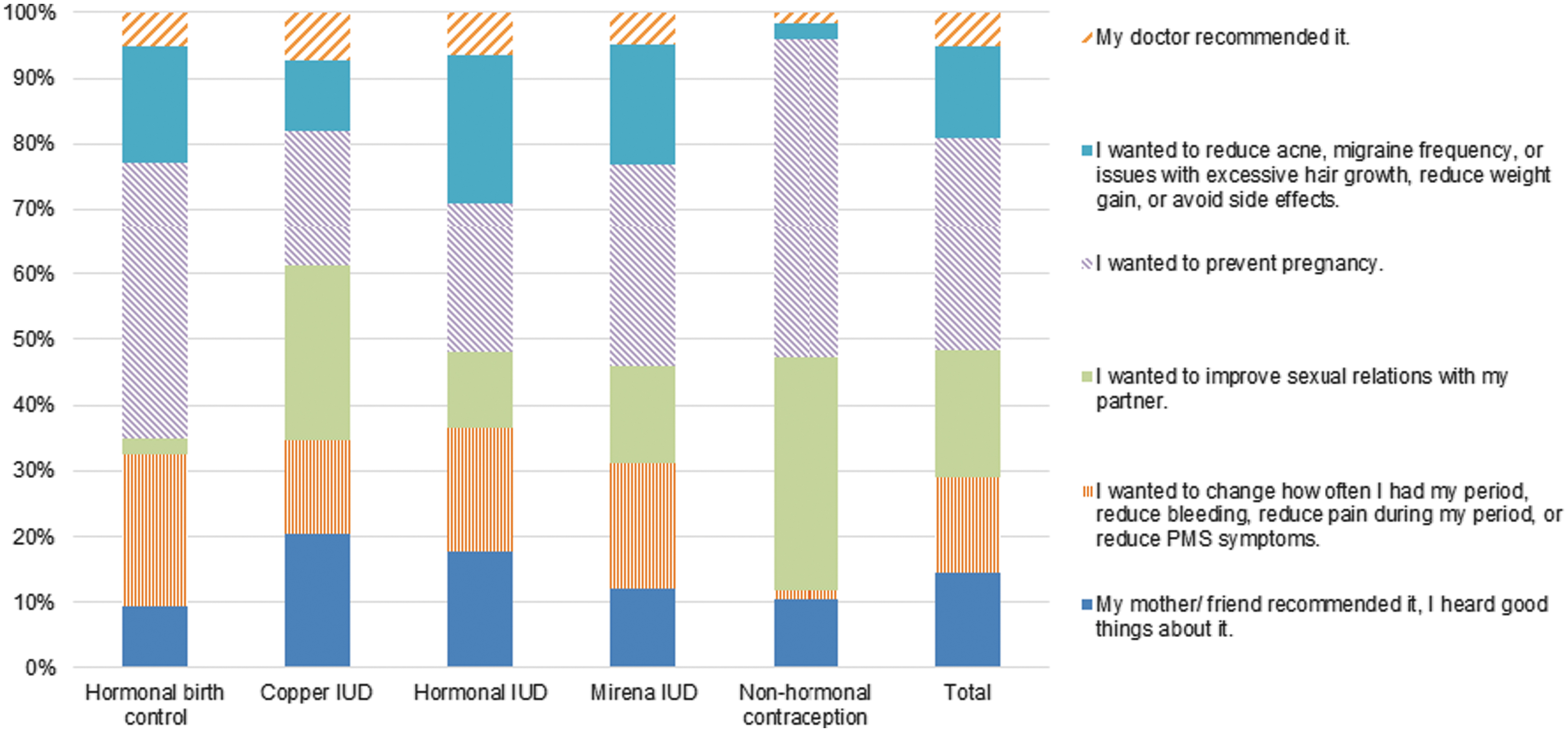
Comparison of primary reasons for choosing method of birth control (n = 2632).
Only 16% (426/2632) of the total sample listed a doctor's recommendation as at least one of the reasons that they chose their current birth control method. Women in the hormonal contraception group had the highest frequency of responding that a provider's recommendation was at least one reason they chose their birth control method (26.1%), followed by CuT IUD users (18.9%), hormonal IUD users (15.6%), Mirena IUD users (15.6%), and nonhormonal birth control methods (8.1%; Supplementary Fig. S3). Friend's recommendation was selected as one of the reasons for choosing their current method of birth control by 38.8% (1022/2632) of the sample. Most of those who chose friend's recommendation as one of the reasons for using their current contraception, however, were using a nonhormonal form of birth control at 56.9% (350/615), followed by CuT IUD users at 49.9% (275/551).
Satisfaction with the current method of birth control was high, with only 7.6% of the total sample reporting dissatisfaction or being neither satisfied nor dissatisfied (Supplementary Fig. S4). Satisfaction varied by birth control type (p < 0.001) with nonhormonal birth control users having the highest frequency of participant satisfaction (97.2%), followed by CuT IUD users (93.4%), hormonal IUD users (90.3%), Mirena users (89.5%), and hormonal contraception users (89.4%). The most frequent reasons for lack of satisfaction were related to change in mood (Supplementary Table S1).
There were significant differences in intention to replace current contraception with a different type in the next 1–2 months by contraception method (Table 3). Participants using hormonal contraception had the highest proportion (14.4%) report that they were very likely or likely to replace their contraception in the next 2 months, followed by hormonal IUD users (13.1%), Mirena users (10.2%), CuT IUD users (9.5%), and then nonhormonal contraception users (1.5%). However, nonhormonal contraception users had the highest proportion (56.6%) that was uncertain whether they would replace their contraception in the next 2 months. There were also significant differences in intention to replace their birth control method in the next year by contraception method. The highest proportion of participants who were likely to change their birth control method in the next year was among those using hormonal contraception (7.7%), followed by Mirena users (5.5%), other hormonal IUD users (4.2%), CuT IUD users (3.8%), and then by non-hormonal contraception users (0.9%). Sensitivity analyses that combined “very likely” with “likely” responses, and compared them by contraception method using chi-square analyses revealed no difference in the p-value for intention to discontinue either in 1–2 months or 1 year.
How Likely is it that You will Replace {{Q7}} with a Different Type of Birth Control Within the Next 1–2 Months?
{{Q7}} appeared as the type of birth control method that the respondent reported using on the survey.
Compared to women who used hormonal birth control, CuT IUD users had higher odds of reporting that they were satisfied or very satisfied with their current method (Table 4). Nonhormonal contraception users, however, had close to six times the odds of reporting satisfaction with their birth control method compared to hormonal birth control users. Young black women had lower odds of reporting that they were satisfied or very satisfied compared to white women. However, Hispanic women were more than twice as likely to report that they were satisfied compared to non-Hispanic white women.
Logistic Regression Describing Association Between Respondent Characteristics and Satisfaction with Current Birth Control Method
Bolded values indicate significance at p < 0.05
Outcome = “Satisfied” or “Strongly Satisfied” compared to “Dissatisfied,” “Strongly Dissatisfied,” or “Neither Satisfied nor Dissatisfied.”
Discussion
The highest proportion of women in this study, who considered pregnancy prevention as their primary reason for using birth control, was using the least effective types of birth control, such as condoms. A higher frequency of these women also reported having had any type of sex at a younger age than the other birth control types. In addition, many were younger at the time of the survey, and thus are at higher risk for unintended pregnancy. Male condoms have a high probability of failure, at 12.6% after 12 months, compared to LARC with a failure probability of 1.4% during the same amount of time. 11 This is concerning, as the women who were using less effective methods of birth control more commonly listed pregnancy prevention as their primary reason for choosing their method compared to those using LARC. This indicates there is a need for intervention among women choosing less effective methods. Furthermore, young women who use LARC need to be encouraged to use condoms, as they protect against sexually transmitted infections.
Since satisfaction is known to be high among all age groups using LARC, increasing awareness for benefits other than efficacy may be important to potential users. Reasons for discontinuation other than dissatisfaction have been found in other studies. Women who perceived their contraceptive method changed their sexual experience in a negative way were more likely to discontinue their method within 1 year than women who perceived no change or a positive change. 18 Therefore, it is important to discuss expectations and questions regarding sexual experience when discussing a patient's choices for birth control. Providers may not communicate about contraception in an effective manner. For example, providers may not ask all of their patients about their intention to get pregnant or what their preference is for birth control. 19 In addition, providers may fail to determine whether their patients have questions in close to half of contraceptive counseling clinic visits. 19
This study demonstrates that women seek birth control for reasons other than pregnancy prevention and may not choose a method primarily due to their healthcare provider's recommendation. In fact, 15% of the total sample replied that the primary reason they chose their current birth control method was because their mother or friend had recommended it, or had heard good things about it, compared to 5% who replied that their doctor recommended it. In a study of African-American females, they reported the importance of family and friends in the contraceptive decision, indicating that this is an important source of information. 20 Furthermore, for teenagers, inclusion of an adult in the contraception decision is important for pregnancy prevention. 20 A high proportion of the Copper IUD group indicated that improving partner relationships was the primary reason they chose their current birth control, highlighting that women may involve their partners in their decision-making regarding birth control. This has also been found previously. In a sample of women from Texas, 55% of young women indicated that they shared decision-making for contraception with their partners, especially among those who reported using condoms consistently. 21
We found that young black women were less likely to report they were satisfied with their contraception method, while Hispanic women were more likely to report satisfaction with their contraception method compared to white women, even after controlling for contraception type. It is possible that satisfaction could be related to how women make the decision about their methods. Utilizing information from family, friends, or sources other than their healthcare provider may cause women to choose a method that is not specialized to their unique circumstances, as counseling by a health provider is an important component of continued contraception use. 22
We also found that sexual experience is an important reason for choosing a type of contraception, as 19% of the sample in this study reported improving sexual relationships with their partner as a primary reason for choosing their current birth control method. The perception of contraception as detracting from the sexual experience resulted in higher rates of early discontinuation compared to women who reported no difference in sexual experience in another study. 18 Programs that are aimed at increasing LARC use should consider social norms as well as patient expectations when providing them with information about contraception choices. Furthermore, more information is needed to better understand why young black women would be less likely to report satisfaction with their birth control method compared to young white women, whereas young Hispanic women were more likely to report satisfaction.
Most women were satisfied with their birth control. Only 7.6% of the total sample reported dissatisfaction or being neither satisfied nor dissatisfied with their birth control method. Interestingly, satisfaction varied by birth control type with nonhormonal birth control users having the highest rate of satisfaction (97.2%). However, despite satisfaction being high among nonhormonal birth control users, studies have shown, in the past, high rates of method discontinuation among women using these methods of birth control. 9 It has also been found that younger women may be more likely to discontinue their birth control method than older women. In a study of long-term utilization of IUDs, women 30 years and older were less likely to have discontinued use of their IUD than younger women across 48 months. 23 More information is needed to better understand reasons for discontinuing birth control in this group, particularly among adolescents and young women, other than dissatisfaction with the method.
Among study participants who were not satisfied, mood-related symptoms and bad side effects were common reasons for dissatisfaction. Combined oral contraceptives have been found to be associated with mood changes in a clinical trial. 24 Specifically, the use of these methods was associated with anxiety, irritability, and mood swings during the intermenstrual phase, particularly among women who had reported previous negative experiences with combined oral contraceptives. 24 The use of levonorgestrel IUDs has not been found to be associated with depressive symptoms in past studies. 25 However, more research on the association between these devices and mood, particularly among subgroups that have previously experienced negative mood-related effects from other hormonal contraceptives, is needed.
Women using hormonal contraception, hormonal IUDs, or Mirena frequently reported that they were unlikely or very unlikely to replace their birth control with another method in this study. Women using the Mirena IUD (14%) as well as other hormonal IUD users (12%) indicated that regulating their menstrual cycle was important. Mirena was approved by the FDA in 2009 to treat heavy periods for those who choose intrauterine contraception. Compared to other hormonal methods of birth control, the levonorgestrel IUD has been determined to be the most effective method of reducing menstrual bleeding in women with abnormal uterine bleeding, with a 71%–95% reduction in blood loss. 26 Therefore, helping patients to understand how Mirena may decrease bleeding during their periods may be another important factor that patients, even those with normal menstrual cycles, may be interested in better understanding.
Variations in characteristics and sexual behaviors, such as we found in our sample, could affect the receptiveness of different messages related to birth control choice. For example, understanding what type of contraception is needed among multiethnic women and how best to reach them is needed. Currently, new ways of reaching young multiethnic women are being developed as it is recognized that continuing messages about birth control are needed after the high school years. An app developed for 18–20-year-old Hispanic and black women was associated with a lower frequency of reporting recent sex without hormonal or LARC birth control methods. 27 It is also important to develop age-appropriate messages so that younger women can be more informed about using LARC. Most of the 16–17 year olds in this sample used nonhormonal contraception. Unfortunately, there are several barriers to using LARC in this age group, such as cost, misunderstanding among providers about the safety of IUDs, lack of training, and continuing education of providers, as well as lack of availability of LARC. 28,29 Addressing these factors may also help younger patients get easier access to LARC, in addition to other methods.
The strength of this study is that it included a sample of young women from across the United States., with representation from each state. The survey software limited responses so that an IP address could only be used one time. Some limitations are that this survey was biased toward internet users who had access to the internet and had social media accounts, or used Google search engine, as that is where the advertisements were placed. Participants may have also had higher education levels than the standard population for the age range included, indicating selective participation. This may have limited generalizability for those with little to no access to the internet. This survey was marketed to IUD users, and thus may contain selection bias for participants interested in IUDs or who had used them previously. The frequency of some contraception user groups, such as birth control implant users, was low and could not be evaluated separately. Cost was not included in responses related to reasons for choosing their current method. However, no woman included cost as a reason for selecting their current method in the free-text boxes. In addition, these results may not be generalizable to young women who are not sexually active. Furthermore, this study included only current contraception users. Therefore, it may be biased toward women who prefer their current contraception method. Future studies should ask about previously discontinued methods to help address this bias. Although we used satisfaction measures used in the contraceptive literature, it is possible that these measures do not adequately assess satisfaction. Future studies should evaluate wording and contexts of satisfaction to ensure questions are adequately measuring this construct.
These results indicate that providers who encourage young patients to consider LARC methods should consider that they may want to better understand what benefits and side effects their birth control may have, other than those related to pregnancy prevention. Furthermore, intervention efforts focused on providing information through social and family contacts, as well as encouraging current LARC patients to discuss their experiences with others, could help to improve LARC usage. Sharing resources through health providers is an important way to distribute information, but utilizing family and friend networks to reach out to younger women could also help to increase the use of these methods.
Footnotes
Author Disclosure Statement
Dr. J.M.H. was supported by an Investigator Initiated Research grant funded by Bayer HealthCare during the conduct of this study. For the remaining authors, no competing financial interests exist.
Funding Information
This study was supported by an Investigator Initiated Research grant funded by Bayer HealthCare.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.