
Abstract
Case Report
A 28
What is your next step in management?
A. Electrodiagnostic studies.
B. Surgery.
C. Watch and wait.
D. Splint and steroid injection.
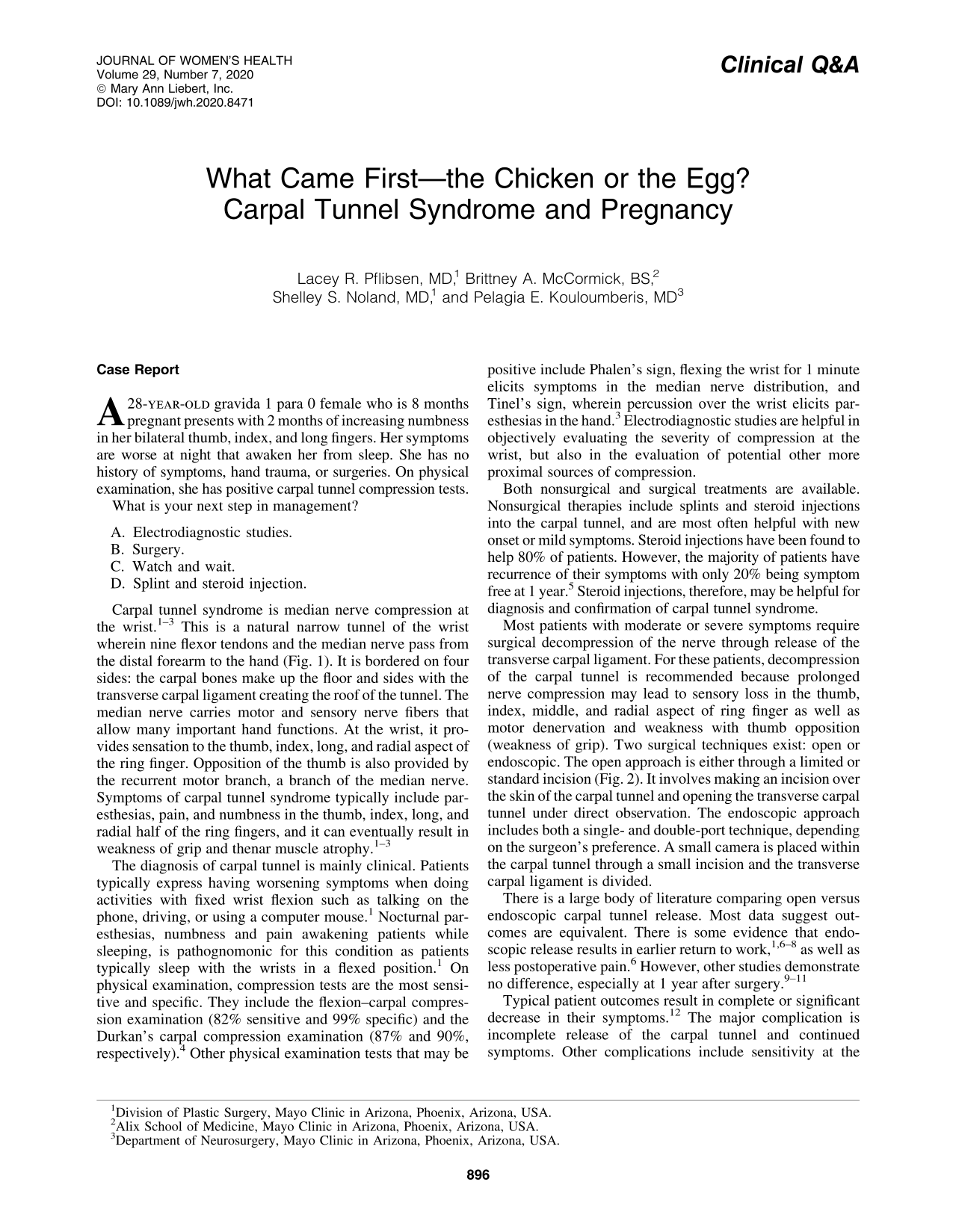
Carpal tunnel syndrome is median nerve compression at the wrist. 1 –3 This is a natural narrow tunnel of the wrist wherein nine flexor tendons and the median nerve pass from the distal forearm to the hand (Fig. 1). It is bordered on four sides: the carpal bones make up the floor and sides with the transverse carpal ligament creating the roof of the tunnel. The median nerve carries motor and sensory nerve fibers that allow many important hand functions. At the wrist, it provides sensation to the thumb, index, long, and radial aspect of the ring finger. Opposition of the thumb is also provided by the recurrent motor branch, a branch of the median nerve. Symptoms of carpal tunnel syndrome typically include paresthesias, pain, and numbness in the thumb, index, long, and radial half of the ring fingers, and it can eventually result in weakness of grip and thenar muscle atrophy. 1 –3
Anatomy of the carpal tunnel. Used with permission of Mayo Foundation for Medical Education and Research, all rights reserved.
The diagnosis of carpal tunnel is mainly clinical. Patients typically express having worsening symptoms when doing activities with fixed wrist flexion such as talking on the phone, driving, or using a computer mouse. 1 Nocturnal paresthesias, numbness and pain awakening patients while sleeping, is pathognomonic for this condition as patients typically sleep with the wrists in a flexed position. 1 On physical examination, compression tests are the most sensitive and specific. They include the flexion–carpal compression examination (82% sensitive and 99% specific) and the Durkan's carpal compression examination (87% and 90%, respectively). 4 Other physical examination tests that may be positive include Phalen's sign, flexing the wrist for 1 minute elicits symptoms in the median nerve distribution, and Tinel's sign, wherein percussion over the wrist elicits paresthesias in the hand. 3 Electrodiagnostic studies are helpful in objectively evaluating the severity of compression at the wrist, but also in the evaluation of potential other more proximal sources of compression.
Both nonsurgical and surgical treatments are available. Nonsurgical therapies include splints and steroid injections into the carpal tunnel, and are most often helpful with new onset or mild symptoms. Steroid injections have been found to help 80% of patients. However, the majority of patients have recurrence of their symptoms with only 20% being symptom free at 1 year. 5 Steroid injections, therefore, may be helpful for diagnosis and confirmation of carpal tunnel syndrome.
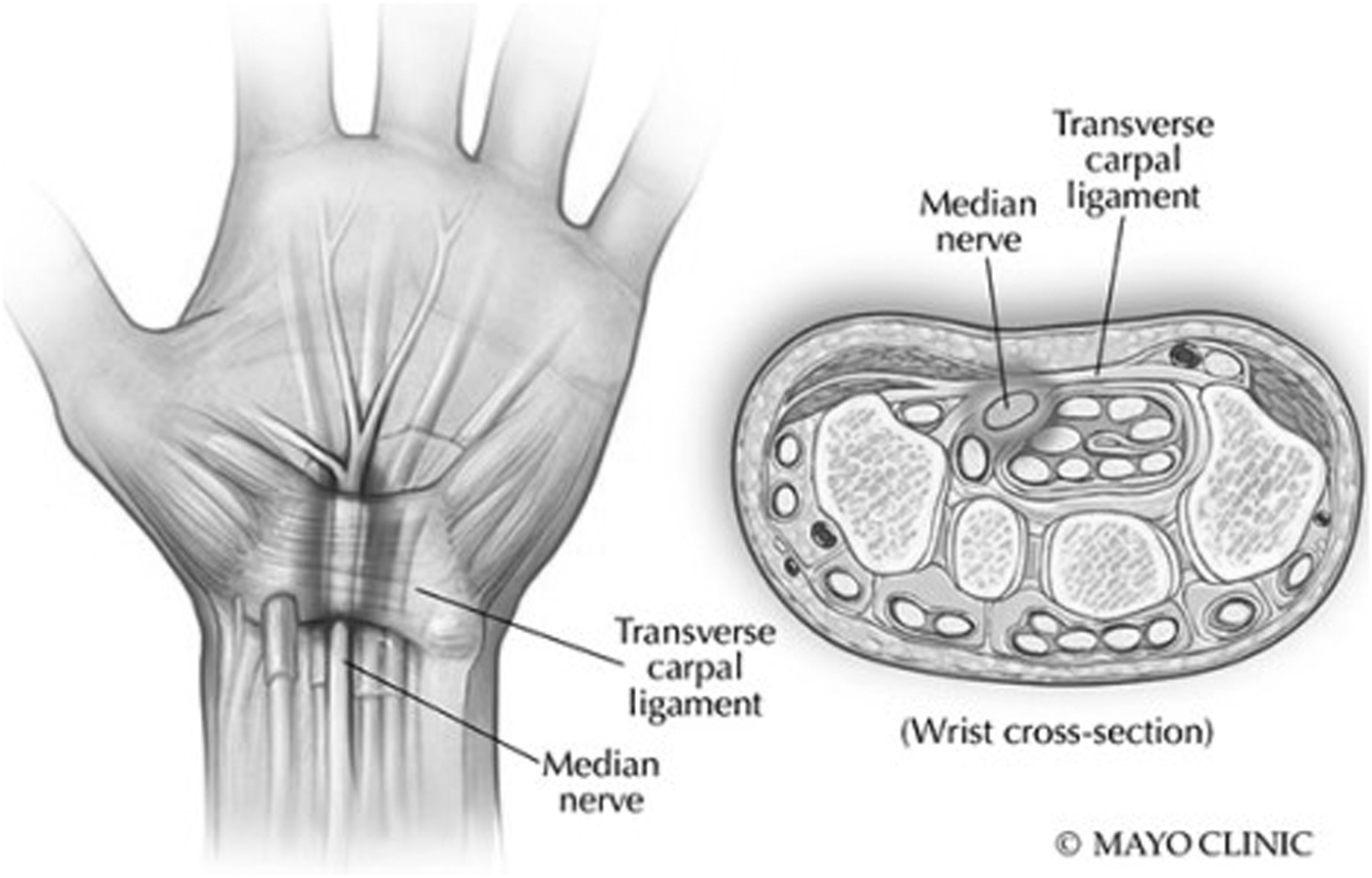
Most patients with moderate or severe symptoms require surgical decompression of the nerve through release of the transverse carpal ligament. For these patients, decompression of the carpal tunnel is recommended because prolonged nerve compression may lead to sensory loss in the thumb, index, middle, and radial aspect of ring finger as well as motor denervation and weakness with thumb opposition (weakness of grip). Two surgical techniques exist: open or endoscopic. The open approach is either through a limited or standard incision (Fig. 2). It involves making an incision over the skin of the carpal tunnel and opening the transverse carpal tunnel under direct observation. The endoscopic approach includes both a single- and double-port technique, depending on the surgeon's preference. A small camera is placed within the carpal tunnel through a small incision and the transverse carpal ligament is divided.
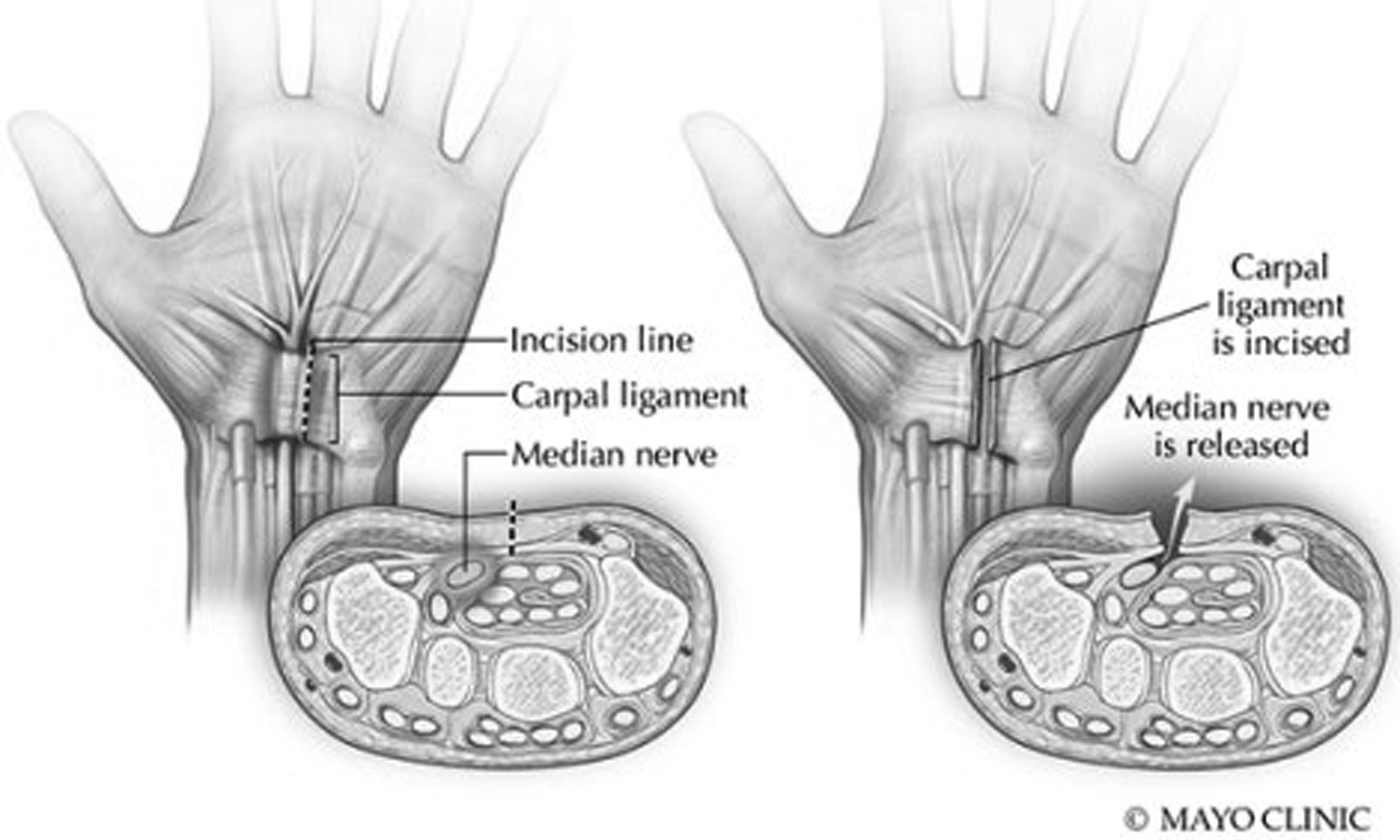
Open carpal tunnel release technique. Used with permission of Mayo Foundation for Medical Education and Research, all rights reserved.
There is a large body of literature comparing open versus endoscopic carpal tunnel release. Most data suggest outcomes are equivalent. There is some evidence that endoscopic release results in earlier return to work, 1,6 –8 as well as less postoperative pain. 6 However, other studies demonstrate no difference, especially at 1 year after surgery. 9 –11
Typical patient outcomes result in complete or significant decrease in their symptoms. 12 The major complication is incomplete release of the carpal tunnel and continued symptoms. Other complications include sensitivity at the incision site (pillar pain) or arm (complex regional pain syndrome), surgical site infection, and injury to surrounding structures such as tendons, nerves, and arteries. The risk of these complications is typically <1%–2%. 13
Answer: The Best Answer Is D
In a patient who is not pregnant, the argument could be made to perform surgical decompression immediately although steroid injection, splint, and electrodiagnostic studies are also all reasonable treatment options. However, during pregnancy, carpal tunnel syndrome is approached differently. The true prevalence of carpal tunnel syndrome during pregnancy is unknown but some studies show that the incidence is as high as 62%, and most commonly presents during the third trimester. 14 –18 The cause is unknown but likely due to hormonal changes and edema (increased total body water during pregnancy). 14,19 Since the carpal tunnel creates a natural bottleneck of the upper extremity, the fluid changes experienced during pregnancy are enough to illicit symptoms through this already narrow tunnel.
Carpal tunnel syndrome usually occurs in the third trimester and typically resolves after delivery. Therefore, the recommended treatment included nonsurgical modalities such as behavior modification, splints, and steroid injections. 15 Steroid injections can be very helpful for temporary relief. However, it is contraindicated in the hyperglycemic patient, as it elevates systemic blood sugar. Overall, the consensus is that surgery is rarely indicated in the pregnant patient. 16,17
Most patients experience resolution of symptoms postpartum with pain scores reduced significantly within 2 weeks. 20 Despite improvement of symptoms in the majority of patients after child birth, 49% of patients complain of continuous symptoms and 11% are still wearing a splint at 3 years postpartum. 18 It is possible that these patients had subclinical carpal tunnel syndrome before pregnancy. If symptoms are not improving within 2 weeks after childbirth, surgical decompression should be considered.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.