
Abstract
Background:
Multiparity is a risk factor for cardiovascular disease (CVD). However, the mechanisms of this relationship are unknown. Adipokines may predispose multiparous women to certain cardiometabolic complications that can increase their risk of future CVD.
Materials and Methods:
We studied 973 female participants of the Multi-Ethnic Study of Atherosclerosis free of CVD, who had complete data on parity and adipokines measured at Examination 2 or 3 (randomly assigned). Parity was categorized as nulliparity, 1–2, 3–4, and ≥5 live births. Multivariable linear regression was used to evaluate the association of parity with leptin, resistin, and adiponectin levels.
Results:
The women had mean age of 65 ± 9 years. After adjustment for age, race/ethnicity, study site, education, menopause status, smoking, physical activity, use of hormone therapy, and waist circumference, a history of grand multiparity (≥5 live births) was associated with 11% higher resistin levels (95% confidence interval [CI] 0–23) and 3–4 live births was associated with 23% higher leptin levels (95% CI 7–42), compared with nulliparity. After adjustment for computed tomography-measured visceral fat, the association of 3–4 live births with leptin remained significant. There were no significant associations of parity with adipokines after further adjustment for additional CVD risk factors. Multigravidity (but not parity) was inversely associated with adiponectin levels.
Conclusions:
In a multiethnic cohort of women, greater parity was associated with resistin and leptin; however, this association was attenuated after accounting for CVD risk factors. Dysregulation of adipokines could contribute to the excess CVD risk associated with multiparity. Further studies are needed to determine whether adipokines independently mediate the relationship between multiparity and CVD. Clinical trials registration: The MESA cohort is registered at NCT00005487.
Introduction
Cardiovascular disease (CVD) remains the leading cause of death in women. From 2000 to 2010, there had been a decline in CVD mortality among women in the United States; however, more recently, there has been a concerning plateauing or even a slight rise in CVD mortality among women since 2010. 1 In fact, middle-aged women (aged 45–65 years) experienced the greatest relative increase in heart disease death rates between 2011 and 2017. 2 The adverse trends in slowing and potentially reversing the progress made in CVD mortality are largely related to increasing rates of the cardiometabolic diseases of obesity and type 2 diabetes 1 and the related worsening cardiovascular health of U.S. adults. 3 The trend in the increasing prevalence of obesity is present across all races and considerably higher in women than in men. 1 This worrisome pattern is an indication that more intensive preventive efforts are still sorely needed in women.
In addition to the risk conferred by traditional risk factors, there appear to be other sex-specific factors that may predispose certain women to a higher risk of CVD, including those associated with pregnancy. 4,5 In this regard, several prior observational studies have shown that a greater number of live births (parity) is independently associated with risk of CVD. 6 –10 Notably, the mechanism of increased CVD risk with parity is not fully understood. Prior work from Multi-Ethnic Study of Atherosclerosis (MESA) found that multiparous women, particularly those with history of ≥5 live births, were less likely to have ideal cardiovascular health and had greater body mass index (BMI) at middle to older ages. 11 In addition to the physiological changes that occur during each pregnancy, such as insulin resistance and hormonal changes, multiparous women may also have behavioral changes that lead to a more sedentary lifestyle. Therefore, a focus on individuals with grand multiparity may represent a unique opportunity for preventive action to reduce their CVD risk.
The obesity-related hormones of adipokines, such as adiponectin, leptin, and resistin, play important roles in appetite regulation, glucose metabolism, and inflammatory response. 12 Levels of certain adipokines, such as leptin and resistin, have been found to be increased in the setting of obesity, whereas others, such as adiponectin, are decreased. The dysregulation of adipokines has been demonstrated in various disease processes, including CVD. 12 Some studies have shown a statistically significant association between higher leptin and resistin levels and lower adiponectin levels with incident CVD, heart failure, and coronary artery disease, 13,14 whereas other studies have found these relationships to be attenuated after adjusting for BMI and other CVD risk factors. 15 –18
Additionally, adipokine dysregulation during pregnancy may predispose women to pregnancy-related complications such as gestational diabetes and preeclampsia, which are forerunners of future CVD. 19 –22 Among susceptible individuals, repeated pregnancy-related changes in adipokine metabolism may lead to long-term dysregulation in adipokines, which is detrimental for cardiovascular health. However, the association of adipokines and parity has not been well established, particularly within a diverse population of women.
Thus, the aim of this study was to determine if parity is associated with adipokine levels among women of four racial/ethnic groups enrolled in the MESA study and to evaluate whether parity is associated with adipokine levels independent of underlying adiposity. First, we hypothesized that multiparity would be associated with lower adiponectin levels but higher resistin and leptin levels. Second, we hypothesized that this association would be attenuated after adjusting for adiposity measures but would remain significant.
Materials and Methods
Data availability statement
Data from the MESA study can be requested through the National Institutes of Health (NIH) BioLincc Open program at:
Study population
The MESA cohort originally enrolled 6814 men and women aged 45–84 years who were free of CVD at baseline (2000–2002). The participants were enrolled at six field centers in different U.S. communities including Columbia University, New York; Johns Hopkins University, Baltimore; Northwestern University, Chicago; UCLA, Los Angeles; University of Minnesota, Twin Cities; and Wake Forest University, Winston-Salem. Those enrolled in the study were followed continuously for incident CVD events, and after the baseline examination, up to five subsequent study examinations were completed. For this analysis, we included 973 female MESA participants, free of atherosclerotic CVD, who had complete data on parity assessed at the baseline examination (2000–2002), as well as adipokine levels that were measured as part of an ancillary study at either Examination 2 (2002–2004) or Examination 3 (2004–2006). Examination 2/3, the visit with the adipokine level measurement, serves as the baseline visit for this analysis.
The MESA study received institutional review board approval at each participating field center, and informed consent was obtained from each study participant for the main and ancillary MESA studies.
Independent variable (parity)
Both parity (number of live births) and gravidity (number of pregnancies) were assessed by self-report at the MESA baseline examination (2000–2002). A previously defined algorithm in MESA was used to define parity to account for inconsistent or implausible data. 11,23 Parity was categorized consistent with prior studies in MESA: nulliparity (reference), 1–2, 3–4, and ≥5 live births. 11 In a supplemental analysis, we also examined associations with gravidity, using same categorizations: null gravidity (reference), 1–2, 3–4, and ≥5 pregnancies.
Adipokine assessment
In an ancillary study of MESA, a random subset of participants (n = 1970) underwent abdominal computed tomography (CT) scans at either Examination 2 or 3 (randomly assigned) to measure abdominal aortic calcification. 24 In a subsequent ancillary study related to body composition, adipokine levels were measured among these same participants from stored frozen serum samples obtained at the respective visits (2 or 3) of their CT scan. 25 The adipokines, adiponectin, leptin, and resistin, were analyzed using a Bio-Rad Luminex flow cytometry (Millipore, Billerica, MA, USA) at the Laboratory for Clinical Biochemistry Research (University of Vermont, Burlington, VT, USA), as previously reported. 26,27 The coefficients of variation for these assays ranged from 6% to 13%.
Body composition assessment
Using the abdominal CT data acquired as part of the aforementioned ancillary study at Examination 2 or 3, visceral adipose tissue (VAT) was measured as the total adipose tissue in the abdominal cavity and subcutaneous adipose tissue (SAT) was measured as the total adipose tissue outside the abdominal cavity but not within muscle tissue. VAT and SAT were measured from the average of two CT slices obtained at L2–L3 and adjusted for height, as previously performed. 25
At each study visit, using a standard protocol, the participant's waist circumference was measured at the level of the umbilicus with a measuring tape and rounded to the nearest 0.1 cm, as a measure of central adiposity. Additionally, participant's current height and weight were measured, and BMI was calculated as weight divided by squared height (kg/m2).
Other covariates
At each study visit, participants underwent questionnaires and physical examinations performed by trained staff. For this analysis, we used information obtained at Examination 2 or 3, the same visit that their adipokine levels were measured. The covariates in this study were chosen a priori and include age, race/ethnicity, study site, education, cigarette smoking status, physical activity, menopause status, waist circumference, BMI, VAT, SAT, systolic blood pressure, hypertension medication use, total cholesterol, high-density lipoprotein cholesterol (HDL-C), use of lipid-lowering medications, and diabetes status.
Questionnaires elicited information about the participant's age, race/ethnicity, education, smoking status, and menopause status. Medication use was assessed by inventory. The total amount of moderate and vigorous physical activity was estimated in metabolic equivalent minutes per week using a 28-item Typical Week Physical Activity Questionnaire. 26
Systolic and diastolic blood pressure readings were measured in the seated position with a Dinamap automated device, and the last two of three blood pressure readings were averaged. Diabetes was defined by a fasting blood glucose level ≥126 mg/dL, self-reported diagnosis of diabetes, or the use of diabetes medications.
Participants were also asked (at the baseline examination) about their self-reported weights when they were 20 and 40 years old. Using their current measured height (Examination 2 or 3) and their self-reported weights at ages 20 and 40, their BMIs at ages 20 and 40 were estimated. This calculation assumes that participants' heights have been stable over their adult lifetime, which may not be accurate, but this assumption has been used in prior MESA analyses. 28 Self-reported waist circumference from earlier life periods was not available.
Statistical analyses
Baseline characteristics of women by parity groups were described, with continuous variables presented as means with standard deviation if normally distributed and medians with interquartile range if non-normally distributed, and categorical variables as frequencies with percentages. We used the analysis of variance, Kruskal–Wallis, Fisher's exact, and chi-square tests to compare the differences between continuous and categorical variables as appropriate.
We used progressively adjusted linear regression to evaluate the association of parity categories with each adipokine level separately. Since some of the adipokine measurements are skewed and do not follow a normal distribution, the adipokine levels were naturally log transformed for regression analysis. Our models were as follows: Model 1 adjusted for the demographic factors of age, race/ethnicity, and study site. Model 2 adjusted for Model 1 variables plus menopause status, education, cigarette smoking, and physical activity. We explored adiposity in two parallel models. Model 3a adjusted Model 2 variables plus waist circumference. Model 3b adjusted for Model 2 covariates plus VAT and SAT. Model 4 adjusted for Models 3a and 3b variables plus the additional CVD risk factors of systolic blood pressure, use of antihypertensive medications, total cholesterol, HDL-C, use of lipid-lowering medications, and diabetes status (which includes use of diabetes medications).
We performed several additional sensitivity analyses as follows: (1) we adjusted for BMI instead of waist circumference in Model 3a; (2) we excluded women with heart failure before Examination 2 or 3 (n = 20); (3) we excluded premenopausal women (n = 58); and (4) we evaluated the association between gravidity, which is the number of total pregnancies, with adipokine levels.
The analyses were performed using the STATA 15.0 version (StataCorp LP, College Station, TX, USA). p-Values were two-sided, and significance level was set at 0.05.
Results
Baseline characteristics
The characteristics of the 973 female participants in this study are presented in Table 1. The mean age of the participants at Examination 2 or 3 was 65 ± 9 years. Among the study population, 17.2%, 40.3%, 29.5%, and 13.1% had a history of 0, 1–2, 3–4, and ≥5 live births, respectively. The participants were 38% White, 23% Black, 13% Chinese, and 26% Hispanic adults. Hispanic participants were more likely to have five or more live births, compared with other race/ethnicities. Women with grand multiparity (≥5 live births) were significantly less likely to have an education higher than a bachelor's degree. Women with grand multiparity also engaged in less physical activity and were more likely to be in menopause. Women with grand multiparity not only had a greater waist circumference and higher BMI at the current examination but also reported a higher BMI at ages 20 and 40.
Characteristics of Women by Parity in the Multi-Ethnic Study of Atherosclerosis
Data are presented as mean (SD), number (%), or median (IQR).
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range, MET, metabolic equivalent; SAT, subcutaneous adipose tissue; SD, standard deviation; VAT, visceral adipose tissue.
Relationships of parity and adipokines
A box plot for the unadjusted adipokine levels for each parity group is shown in Figure 1 and median levels reported in Table 2. Women with grand multiparity had higher leptin and resistin levels and a trend for lower adiponectin levels, compared with other parity groups.
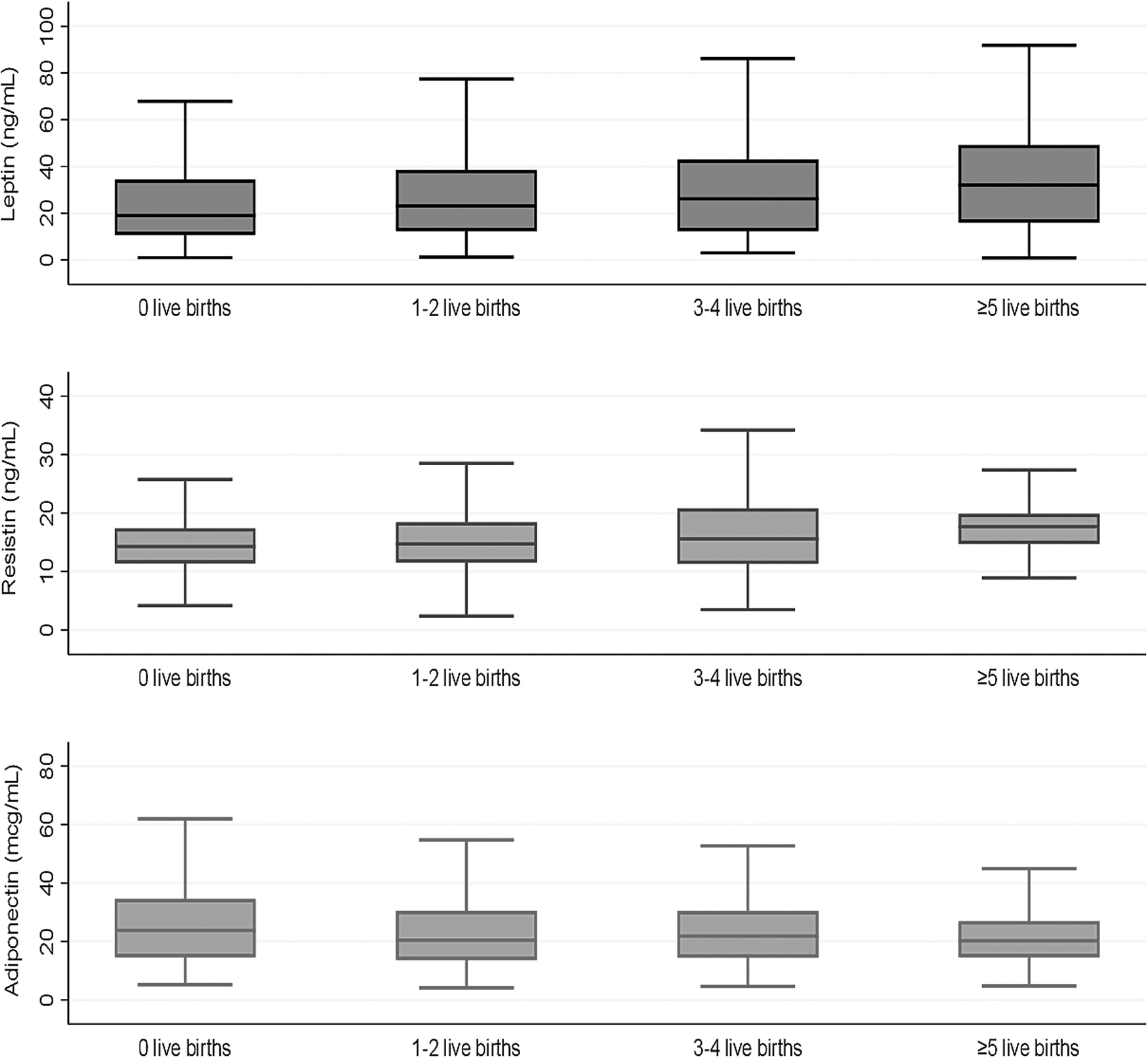
Box plots of adipokine levels by parity categories. The lower and upper boundaries of the rectangles denote the 25th and 75th percentiles while the horizontal line within the rectangles is the median. Lines extend from the rectangles to the smallest and largest values within 1.5 × interquartile range.
Multivariable-Adjusted Association Between Parity and Serum Adipokines Among Women in the Multi-Ethnic Study of Atherosclerosis
Results are presented as percent difference (95% CI) calculated from [Exp (β) − 1] × 100. Median (IQR) for overall cohort: leptin, 25.1 (12.8–42.6) ng/mL; resistin, 15.2 (11.9–19.4) ng/mL; adiponectin, 21.5 (14.2–30.9) mcg/mL. Nulliparity is reference. Statistically significant results are given in bold. Model 1 adjusted for age, race/ethnicity, and study site. Model 2 adjusted for Model 1 covariates, education, cigarette smoking, physical activity, menopause status, and current use of hormone therapy. Model 3a adjusted for Model 2 covariates and waist circumference. Model 3b adjusted for Model 2 covariates, VAT, and SAT. Model 4 adjusted for Models 3a and 3b, systolic blood pressure, use of antihypertensive medications, total cholesterol, HDL-C, use of lipid-lowering medications, and diabetes (including diabetes medications).
CI, confidence interval.
Table 2 also shows the adjusted percent differences in adipokine levels for women with greater number of live births, compared with nulliparous women. After adjustment for demographics of age, race/ethnicity, and study site (Model 1), a history of grand multiparity (≥5 live births) was associated with 12% higher resistin levels (95% confidence interval [CI] 2–24) and 26% higher leptin levels (95% CI 3–55), as well as 3–4 live births was associated with 26% higher leptin levels (95% CI 7–48), compared with nulliparity. After further adjustment for education, menopause status, smoking, physical activity, use of hormone therapy, and waist circumference (Model 3a), a history of grand multiparity (≥5 live births) was associated with 11% higher resistin levels (95% CI 0–23) and 3–4 live births was associated with 23% higher leptin levels (95% CI 7–42), compared with nulliparity. After adjustment for CT-measured visceral fat (Model 3b), the association of 3–4 live births with leptin remained significant (16% relative difference [95% CI 1–34]), but the other associations were attenuated. There were no significant associations of parity with adipokines after further adjustment for additional CVD risk factors, such as blood pressure, diabetes, and lipids (Model 4). We did not find any statistically significant association of parity with adiponectin, although direction of association was inverse.
We performed a series of additional exploratory analyses. BMI was used in the models instead of waist circumference, and findings were generally similar to the overall main results (Supplementary Table S1). The association between parity and adipokines excluding women with heart failure before Examination 2 or 3 (n = 20) is shown in Supplementary Table S2, and again was similar to main analyses. The association between parity and adipokines excluding women who were premenopausal (n = 58) is shown in Supplementary Table S3, and was also similar to the main analyses. In another supplemental analysis, we also examined the association of gravidity with adipokine levels (Supplementary Table S4). Interestingly, compared with women who had never been pregnant (null gravidity), gravidity was inversely associated with adiponectin levels even in fully adjusted model (Model 4), although no clear dose–response relationship was elucidated.
Discussion
In this cohort of middle-aged to older female participants included in the MESA study, we found that a history of grand multiparity was associated with higher resistin and 3–4 live births was associated with higher leptin levels after accounting for sociodemographics, lifestyle factors, menopause status, hormone use, and central adiposity assessed by waist circumference. After accounting for visceral fat assessed directly by CT, this association remained only significant for 3–4 live births with leptin. However, once additional CVD risk factors were included in the model such as diabetes, blood pressure, and lipids, there were no longer any statistically significant associations, suggesting that cardiometabolic risk factors may be mediating factors in the association between parity and adipokines. While we did not find a statistically significant association of parity with adiponectin, multigravidity was inversely associated with adiponectin. To the best of our knowledge, this is the first study that examined the relationship between multiparity and later life adipokine levels in a multiethnic community-based cohort. Our results provide supporting evidence that adipokines may play a potential role in the relationship between multiparity and CVD risk, although their independent risk beyond their association with adiposity remains uncertain.
Cardiometabolic diseases are increasing in the U.S. population, and obesity is greater in women than in men across all race/ethnicities. 1 In 2013–2016, the prevalence of obesity was 36% in men and 40.4% in women, and for severe obesity (BMI ≥40 kg/m2), the prevalence was 5.5% in men and 9.8% in women. We have previously shown that multiparous women had poorer cardiovascular health in mid to older ages and were more likely to have elevated BMI compared with nulliparous women. 11 One explanation is that women may gain weight with each subsequent pregnancy, but adipokine dysregulation as a result of physiological changes the body undergoes after each pregnancy may be another potential mechanism. Breastfeeding influences maternal weight and maternal adipokine levels, 29 which is another potential confounding factor in this relationship; unfortunately, maternal breastfeeding history was not ascertained in the MESA cohort to explore this further.
The literature has provided evidence suggesting that multiparity increases CVD risk. 6 –9 In one study, this association was found to be J-shaped with multivariable-adjusted hazard ratios for incident CVD for 1 live birth of 1.09 (1.03–1.15) and for ≥5 live births of 1.47 (1.37–1.57), compared with women with a history of 2 live births. 8 Other studies have shown a linear relationship. However, the mechanism of this relationship is still unknown. During pregnancy, there are normal physiological changes that influence the cardiovascular risk factors of lipids, glucose, and weight, along with additional stressors such as endothelial dysfunction, inflammation, and hemostatic processes. These factors and stressors could be compounded over time for women who experience multiple pregnancies.
In obese individuals, adipokine dysregulation leads to various complications such as insulin resistance that can contribute to CVD. 30 Given the role of adipose tissue and its hormones in regulating metabolism and energy homeostasis, adipokines have also been implicated in playing a role in both normal and complicated pregnancies. 31,32 Adipokine levels during pregnancy can affect maternal weight gain, although this relationship is likely bidirectional. Even among non-obese women, higher leptin levels have been associated with gestational weight gain. 33 Adipokine dysregulation may predispose to pregnancy-related complications such as gestational diabetes and preeclampsia. 19 –22 In turn, among susceptible individuals, repeated pregnancy-related changes in adipokine metabolism may lead to long-term dysregulation in adipokines, which is detrimental for cardiovascular health.
Thus, adipokines are a potential mechanism to explain the increased risk of parity with CVD. However, before this work, the association of parity history with later life adipokines had not been well established, particularly among diverse populations of women. In the San Diego Filipino Women's Health Study conducted among women with at least 1 live birth, adiponectin levels were inversely associated with obesity and were significantly lower in the medium parity (3–5 live births) and grand multiparity (≥6 live births) compared with low parity (1–2 live births). 34 However, age-adjusted leptin levels did not differ by parity categories in that study. The association of parity with adipokine levels among other racial/ethnic groups warranted further study, which is why we undertook this analysis in a multiethnic cohort. In our study, we found that there was not a significant interaction with race/ethnicity (p-interaction >0.05).
Leptin, adiponectin, and resistin are among the adipokines that are hypothesized to be most important in regulating cardiovascular health. Higher leptin levels have been associated with increased CVD risk in some studies but not others, and with an attenuation of the magnitude of the relation after accounting for BMI in some studies. 15 –17 We found 3–4 live births and ≥5 live births to be associated with higher leptin levels, although the latter was no longer significant after taking into account adiposity. This may be due to increased leptin leading to excessive weight gain during each pregnancy, especially in the second trimester. 35
In general, higher adiponectin levels are associated with lower CVD risk. 14,18 However, Sattar et al. found that adiponectin levels only had a moderate association with coronary heart disease. 18 In our study, we found no significant association of multiparity and adiponectin levels, although relationships were generally inverse. Other studies have indicated that obesity was associated with lower adiponectin levels throughout pregnancy. 36 This suggests that any link between parity and adiponectin is largely driven by weight. In contrast to parity, we did find an inverse association of gravidity with adiponectin, compared with women who had never been pregnancy, although a dose relationship with number of pregnancies could not be clearly elucidated. The mechanism explaining this association is uncertain and may reflect hormonal and health differences if the women were nulligravid due to infertility rather than by choice.
In contrast to leptin and adiponectin, resistin is known to be consistently associated with CVD. 13 In this study, we found that multiparity was significantly associated with higher resistin levels when adjusting for demographic risk factors and waist circumference (but not CT measured VAT). However, this link may be mediated through traditional risk factors as associations were attenuated in more fully adjusted models. Further studies include observing adipokine levels throughout time are needed to establish temporal relationship between each pregnancy and adipokine measurement and subsequent CVD status.
Strengths and limitations
Our study was conducted to glean insight into the relationship between parity and adipokine levels and whether such relationships were independent of adiposity. The strengths of this study include using a well-characterized cohort of women with the ability to adjust for important CVD risk factors, including demographics, waist circumference, CT measures of visceral fat, as well as diabetes status and medications.
However, our findings must be considered in the context of several limitations. First, this was a cross-sectional study, so neither temporality nor causality can be determined. Adipokine levels were only measured at one visit, so their changes over time cannot be evaluated. Second, although we adjusted for a number of socioeconomic and lifestyle factors, there is a chance of residual confounding by other risk factors. Third, we performed multiple comparisons and did not adjust p-values for multiple testing, but our work was meant to be hypothesis generating to be confirmed in additional study. Fourth, adipokine levels were only available in a subset of women in MESA, which reduced the statistical power for interaction testing by subgroups. Fifth, prepregnancy weights were not available, and weights at ages 20 and 40 were self-reported. Sixth, data on interpregnancy intervals were not available. Nor was there any information regarding adverse pregnancy outcomes such as preeclampsia or preterm birth. Finally, we did not have information about whether nulliparity or null gravidity was by choice or due to other health conditions that are associated with metabolic dysregulation (e.g., polycystic ovary syndrome). Despite these limitations, we hope that the results of this study serve as supporting evidence to garner work in this area to elucidate the relationship between multiparity and adipokine regulation.
Conclusions
In a multiethnic U.S. cohort of women, we showed that multiparity is associated with resistin and leptin, but most relationships were attenuated after considering visceral fat and other CVD risk factors, which may represent mediators in this relationship. Further studies are needed to determine whether adipokines independently mediate the relationship between multiparity and CVD.
Footnotes
Acknowledgments
The authors thank the other investigators, the staff, and the MESA participants for their valuable contributions. A full list of participating MESA investigators and institutions can be found at
Authors' Contributions
C.P.R. and E.D.M. designed the study and wrote the initial draft. O. Ogunmoroti performed the statistical analysis. M.A.A. secured grant funding for the measurement of adipokines and visceral fat by CT. R.Q., O. Ogunmoroti and O. Osibogun, C.E.N., J.E.T., A.S.M., A.G.B., and M.A.A. all provided critical revisions for important intellectual content. All authors approved of the final draft for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
E.D.M. is supported by the Amato Fund for Women's Cardiovascular Health at Johns Hopkins. C.P.R. is supported by the Dean's Research Fund at Johns Hopkins University Medical School. A.S.M. is supported by National Insitutes of Health (NIH)/National Heart Lung and Blood Institute (NHLBI) Training Grant T32HL007024. R.Q. is supported by an NIH T32 training grant (5T32HL007227). The MESA study is supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, and N01-HC-95169 from the NIH/NHLBI, by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from NCATS, and R01- HL088451. There is no relationship with industry.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.