
Abstract
Background:
Characterizing estradiol among women with HIV may have implications for breast cancer and cardiovascular disease risk but has not been adequately explored. We quantified differences in total (E2), free (FE2) estradiol, and sex hormone binding globulin (SHBG) by HIV and viral suppression status.
Methods:
Women from a substudy (2003–2006) within the Women's Interagency HIV Study (IRB approved at each participating site) were included if they reported: a period in the last six months, were not pregnant/breastfeeding, no oophorectomy, and no exogenous hormone use in the prior year. Serum was collected on days 2–4 of the menstrual cycle. We assessed differences in biomarkers at 25th, 50th, and 75th percentiles by HIV and viral suppression status using weighted quantile regression.
Results:
Among 643 women (68% with HIV) median age was 37 years. All E2 percentiles were significantly (p < 0.05) lower in women with suppressed viral load versus women without HIV (4–10 pg/mL). The 25th and 50th percentile of E2 were 4–5 pg/mL lower in women with unsuppressed viral load compared to women without HIV (p < 0.05). The 25th and 50th percentile of SHBG was significantly higher in women with unsuppressed viral load compared to women without HIV (10 and 12 nmol/L, respectively). There were no consistent differences in estradiol or SHBG by suppression status.
Conclusions:
There were no differences in FE2 but significantly lower E2 and higher SHBG among women with HIV versus without HIV. Further research is merited in a large contemporary sample to clarify the clinical implications of these findings.
Introduction
There is evidence that people living with HIV experience gonadal and hormonal dysfunction. 1,2 Understanding the impact of HIV on endogenous sex steroid hormones in women, particularly estrogen, is critical because these hormones modulate the immune system3 and are implicated in the development and progression of chronic comorbidities, including breast cancer, 4 –9 cardiovascular disease, 10,11 kidney disease, 12,13 liver disease, 14 bone disease, 15,16 and central nervous system disorders. 17,18 For instance, few studies have demonstrated breast cancer risk is lower comparing women with versus without HIV, and estrogen suppression has been hypothesized as a potential mechanism. 19 –21
As women with HIV have life expectancies approaching those of the general population, and the age distribution shifts toward postmenopause, 22 –24 these comorbidities are increasingly relevant and whether women are experiencing estrogen suppression will inform reproductive health care.
Earlier research lends credence to potential estrogen suppression in women with HIV: studies have often demonstrated that women with HIV are more likely to experience amenorrhea compared with women without HIV. 25,26 The mechanisms that could lead to estrogen suppression in women with HIV are likely multifactorial, possibly driven by higher use of opioids that suppress ovulation, 27 –30 higher prevalence of smoking, 31 stress, 32,33 weight loss, and the proinflammatory state associated with HIV. It is also possible that there is interaction between the HIV virus and estrogen, with one study finding that viral load dropped a median of 0.16 log10 copies/mL from the early follicular phase to the mid-luteal phase within the menstrual cycle. 34
Epidemiological research investigating estrogen suppression with biomarker data in women with HIV is sparse. Prior studies examining estradiol (the most biologically active and abundant form of estrogen before menopause) 35 are equivocal. 36 –41 Of importance, these studies were limited in sample size and did not account for relevant covariates contributing to potential differences in estrogen levels such as body mass index (BMI), smoking, opioid use, and among women with HIV, treatment, or immune status. Previous works did not all consistently measure estradiol when it is most stable during the menstrual cycle.
These analyses also did not consider the role of sex hormone binding globulin (SHBG) or assess free estradiol. When estradiol circulates in the blood, it is usually bound to albumin, or more commonly SHBG. While bound to SHBG, it cannot enter cells, activate receptors, or carry out its function. The remaining estradiol (free estradiol) can interact with cells and their receptors, carrying out its function. Thus, free estradiol, as opposed to total estradiol, is most relevant to adverse health outcomes. Finally, prior works have not explored whether HIV viremia is associated with estradiol concentrations or the directionality of that association (whether HIV viremia impacts estradiol or vice versa).
Thus, our objective was to quantify differences in total and free estradiol as well as SHBG between women with and without HIV, and among women with HIV by viral suppression status using a large sample of U.S. women with and without HIV who are sociodemographically comparable.
Methods
Study population
Data for this study were collected by the Women's Interagency HIV Study (WIHS), now the Multicenter AIDS Cohort Study/WIHS Combined Cohort Study. The WIHS is a multicenter prospective, interval cohort study of women with and at high risk for HIV in the United States. 42 Established in 1993, there are six consortia comprising multiple sites across the country. Study visits are conducted every 6 months, including a structured interview (assessing medical history, antiretroviral therapy [ART], lifestyle factors, and health care utilization), physical and gynecologic examinations, HIV status and HIV viral load, and biological specimen collection. There have been four recruitment waves since the inception of the WIHS.
The data are maintained by the Department of Epidemiology at the Johns Hopkins Bloomberg School of Public Health. For all participants, written informed consent was ascertained, and the study was approved by institutional review boards from each participating site.
Cis-gender women (assigned female sex at birth) participating in the sex steroid substudy nested within the WIHS were eligible for our study. 36,39 The sex steroid substudy took place from visits 18 to 25 (2003–2006), during which serum samples were collected to assess cycle-specific sex steroid hormones (estradiol, inhibin-B, SHBG, and follicle-stimulating hormone [FSH]) to assess the effect of HIV on the age of onset of diminishing ovarian reserve. Samples were collected among women once between days 2 and 4 at the start of her menstrual cycle (the early follicular phase, when estradiol concentrations are stable). Women were eligible if they reported having a period the past 6 months, and had no history of unilateral or bilateral oophorectomy, no breastfeeding in the last 6 months, were not currently pregnant, and no exogenous hormone use (including hormonal contraceptives and hormone replacement therapy) in the past 12 months.
Women were included in our analysis who met these inclusion criteria, had complete data regarding inclusion criteria, and had an estradiol measurement (n = 643). Women were additionally excluded if they: (1) self-reported being menopausal (defined as no reported period in the last 12 months) (n = 6), (2) did not have HIV viral load measured at the substudy visit (n = 2); (3) had a high level of estradiol (>350 pg/mL, [n = 1]); and (4) were missing covariates included in regression analyses (n = 9) (Fig. 1). The threshold of 350 pg/mL was utilized to remove women who may have misreported their eligibility for inclusion in the sex steroid substudy, as these values are indicative of possibly being pregnant/breastfeeding or taking exogenous hormones.
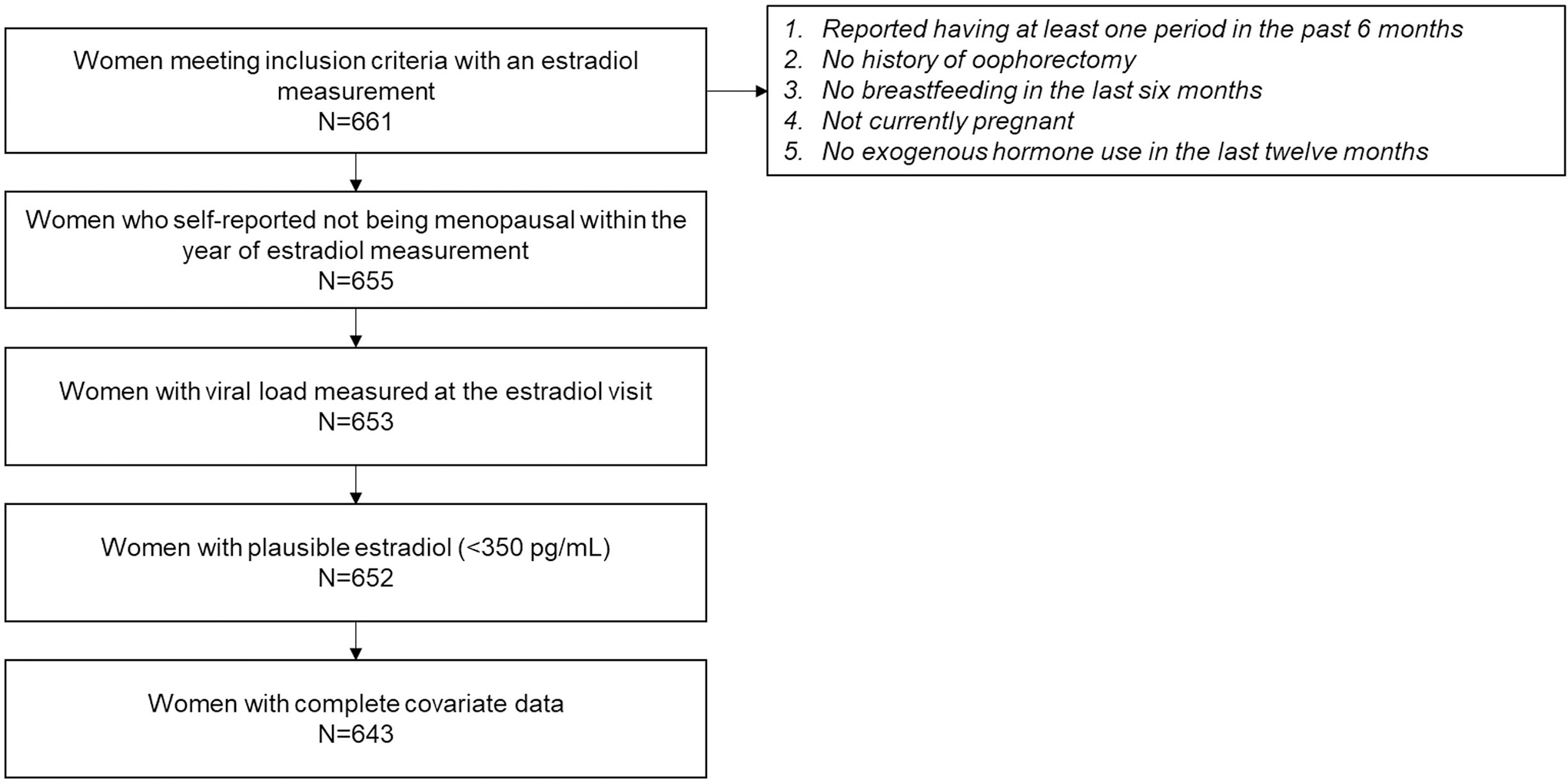
Flow diagram for inclusion into the analytic population.
Biomarker measurements
Total estradiol was assessed continuously and measured in picograms per milliliter (pg/mL). Estradiol was measured using serum samples on the Coat-A-Count solid-phase radioimmunoassay (Siemens Medical Solutions, Malvern, PA) with six-dilution calibration standards and a zero control (lower limit of quantification = 20 pg/mL). 36,39 SHBG was tested using a chemiluminescent assay run on the Siemens DPC Immulite (Siemens DPC, Washington, DC) using their reagents, and was assessed continuously and measured in nanomoles per liter (nmol/L). Estradiol and SHBG measurements were both performed by Quest Diagnostic Laboratories (Baltimore, MD). Of the 643 women included, 431 also had SHBG measured at the same visit and laboratory. Free estradiol was calculated using total estradiol, SHBG, and a constant for albumin. 43
Covariates
Race/ethnicity was defined categorically: non-Hispanic white, non-Hispanic Black, Hispanic, and other. This was selected to ensure sufficient sample size to conduct regression analyses and maximize precision. Covariates assessed at the time of the biomarker measurements included: BMI (analyzed continuously as kg/m2), smoking status (current, former, and never), alcohol use (abstain, 1–7, 8–12, and 12+ drinks/week), age at menarche (years of age), parity (nulliparous, 1, 2, 3, and 4+ births), age (years), hepatitis C status (measured using HCV [hepatitis C virus] RNA among those seropositive at entry into the WIHS), and opioid use (self-reported prescribed [including methadone] and nonprescribed use).
Among women with HIV, ART status at the substudy visit was collected (no therapy vs. on therapy), as was cumulative duration of protease inhibitor (PI) use, and CD4 count (assessed continuously, cells/mm3). PI use was assessed because this class of medications has known metabolic complications which could inform hormone concentrations. Missing values for BMI and CD4 count were carried forward from the last visit attended (6–12 months) before the substudy visit as needed (n = 13 and n = 1, respectively).
Exposure assessment
HIV status was stratified into three categories: women without HIV, women with HIV and suppressed viral load defined as HIV RNA <200 copies/mL, or women with HIV and unsuppressed viral load. This cutoff for viral load was used because it is a clinically relevant marker regarding HIV transmission, has been associated with adverse health outcomes, and is the current threshold used to define virological failure used by the Department of Health and Human Services. 44,45
Comparisons were made between women without HIV with women with HIV with suppressed, or unsuppressed viral load. Among women with HIV, women were first compared by suppression status at the substudy visit. Then, to explore the temporality of the association between viral suppression and these biomarkers, we also assessed the viral suppression status at the last visit attended (6 months before, or if not attended, 12 months) before the biomarker measurement.
Statistical analyses
First, we evaluated differences in demographic, clinical, and reproductive factors by HIV status (women with vs. without HIV) using nonparametric two-sample tests for continuous covariates and chi-square tests for categorical variables. Second, we calculated geometric means for total estradiol, free estradiol, and SHBG by HIV status, and among women with HIV, by viral suppression status. T-tests on the log-transformed values of these biomarkers were utilized to assess statistically significant differences by HIV status and viral suppression status. 46 Geometric means were selected to reduce sensitivity to skewed values.
Third, we utilized weighted quantile regression to estimate differences in total estradiol, free estradiol, and SHBG by HIV status. Pairwise comparisons were made with women without HIV as the reference group with: (a) women with suppressed HIV viral load, and (b) women with unsuppressed HIV viral load.
Among women with HIV, women with suppressed versus unsuppressed viral load at the substudy visit and 6–12 months before the visit were also compared. We hypothesized that women without HIV would have higher total and free estradiol but lower SHBG compared with women with suppressed or unsuppressed viral load. Among women with HIV, we hypothesized that women with suppressed viral load would have higher total and free estradiol with lower SHBG compared with women with unsuppressed viral load, and this association would strengthen when viral suppression was assessed before the biomarker measurement.
Quantile regression assesses whether there is a shift in the distribution of the outcome at a particular quantile. 47,48 For instance, at the 50th percentile (i.e., median), quantile regression assesses if there is a difference in the median estradiol levels between women with HIV and suppressed viral load compared with women without HIV. This can be performed for any percentile and allows for assessment of shift in entire distribution and not only at the central tendency (i.e., mean) that are typically modeled. Therefore, this approach can provide a comprehensive examination of the entire distribution of the outcome. This methodology is also advantageous when the outcome is not normally distributed, 48 which was evident in this analytic population. We assessed our biomarkers at three separate quantiles: 25th, 50th, and 75th percentile to capture associations with HIV status across the distribution.
Stabilized inverse probability weights were utilized to address confounding by several measured covariates. 49 Time-fixed weights were estimated using multinomial and logistic models where HIV status was the outcome, with following variables as predictors: race/ethnicity, log-transformed BMI, smoking status, current hepatitis C status, alcohol use, opioid use, age at menarche, parity, and current age. Models among women with HIV only were additionally weighted for ART status and CD4 count. Robust variance estimation was used to calculate standard errors. Estimates from the weighted quantile regression for each percentile (1st–99th) were graphically assessed to depict the distribution of each biomarker stratified by HIV status.
Subgroup analyses were conducted additionally excluding women with total estradiol levels >150 pg/mL (n = 13). These were considered to be likely inaccurate owing to measurement error given that measurements were supposed to be collected on days 2–4 of the menstrual cycle. We also conducted subgroup analyses among women with both FSH and inhibin-B data available who had FSH <20 pg/mL and detectable inhibin-B (n = 289) to mitigate inclusion of women who may be peri or postmenopausal.
Results
There were 643 women who participated in the sex steroid substudy meeting our inclusion criteria (Table 1). Women were predominantly non-Hispanic Black (63%), had a median age of 37 (interquartile range, 32–42), and were hepatitis C negative (86%). Fifty-one percent of women reported currently smoking, and 9% reported problematic drinking (>7 drinks/week). Women with HIV had statistically significantly lower BMI (p = 0.01) compared with women without HIV, and were less likely to report current smoking (p ≤ 0.01) as well as current drinking (p ≤ 0.01) compared with women without HIV. There were no differences in self-reported opioid use by HIV status. There were statistically significant differences in parity comparing women with versus without HIV (p = 0.03). Age at menarche was similar in women with and without HIV, with an overall median of 12 years.
Demographic and Clinical Factors by HIV Status Among Women in the Sex Steroid Substudy Measured at the Sex Steroid Substudy Visit (Women's Interagency HIV Study)
Values in bold demonstrate statistically significant difference by HIV status.
Nonparametric two-sample test for continuous variables and chi-square test for categorical variables comparing all women with HIV versus without HIV. For variables relevant to HIV, statistical tests were conducted comparing suppressed versus unsuppressed.
ART, antiretroviral therapy; IQR, interquartile range; PI, protease inhibitor.
Sixty-eight percent of participants were women with HIV. Sixty percent were not suppressed (n = 263), and 40% (n = 177) were suppressed at the substudy visit. Women with unsuppressed viral load were more commonly Black relative to those achieving suppression. Women with suppressed viral load were more likely to currently be on ART (88%) compared with women who were not virally suppressed (53%), p ≤ 0.01. Women with suppressed viral load had higher CD4 count compared with unsuppressed women (524 vs. 367 cells/μL, p = 0.03) and were more likely to also be suppressed at the last visit attended before the substudy visit (76% vs. 18%, p ≤ 0.01).
The duration of PI use was comparable by suppression status (p = 0.26). Among women with HIV, women with unsuppressed viral load were more likely to be smokers (55% vs. 33%). Current self-reported problematic drinking was lower in women with versus without suppressed viral load.
Geometric means of total estradiol were statistically significantly lower in women with HIV than in women without HIV (Table 2): (36.9 pg/mL vs. 41.6 pg/mL, p ≤ 0.01). Among women with HIV, total estradiol was lower in women who achieved suppression: 38.2 pg/mL among unsuppressed women versus 35.1 pg/mL among suppressed women, but was not statistically significant. Total estradiol was significantly lower in women with suppressed versus unsuppressed viral load when assessed at the last visit attended before the substudy visit (p = 0.03).
Geometric Means of Estradiol and SHBG by HIV Status and Viral Suppression Status
X indicates not applicable.
CI, confidence interval; SHBG, sex hormone binding globulin.
Free estradiol did not differ comparing women with versus without HIV (p = 0.21). Among women with HIV, free estradiol was significantly higher in women who did not achieve suppression (1.4 vs. 1.2 pg/mL, p = 0.01), which was similar when suppression status was assessed at the visit prior (p = 0.02). SHBG was higher in women with versus without HIV: 58.8 nmol/L versus 47.0 nmol/L. Among women with HIV, SHBG was not significantly different by viral suppression status assessed at the biomarker measurement or at the visit before the substudy visit (p = 0.10, and p = 0.51, respectively).
Quantile regression estimated total estradiol levels revealed potential differences by HIV status (Table 3). In weighted analyses, women with suppressed viral load compared with women without HIV had lower total estradiol at the 25th, 50th, and 75th percentile. The median total estradiol level was 6 pg/mL lower among women with suppressed viral load than in women without HIV (β = −6, 95% confidence interval [CI], −10.75 to −1.25). Thus, while women without HIV had an expected median of 41 pg/mL, women with suppressed viral load had an expected median of 35 pg/mL.
Weighted Quantile Regression Estimates for the Association Between HIV Status and Viral Suppression Status with Estradiol and Sex Hormone Binding Globulin at the 25th, 50th, and 75th Percentile
Estimates in bold are statistically significant.
IPWe for: age, race/ethnicity, smoking status, hepatitis C status, age at menarche, parity, log BMI, alcohol use, and opioid use.
IPWe for: age, race/ethnicity, smoking status, age at menarche, hepatitis C status, parity, log BMI, alcohol use, opioid use, therapy status, and CD4 count.
The 25th percentile of total estradiol was also 4 pg/mL lower comparing women with unsuppressed viral load with women without HIV (β = −4, 95% CI, −7.47 to −0.53), and the median was 5 pg/mL lower comparing women with unsuppressed viral load with women without HIV (β = −5, 95% CI, −9.74 to −0.26).
Among women with HIV, there were no statistically significant differences in total estradiol when viral suppression was assessed at the same visit, although women with suppressed viral load consistently had lower total estradiol than women with unsuppressed viral load. When suppression was assessed at the visit prior, the 25th percentile was 6 pg/mL lower in women with suppressed viral load compared with women with unsuppressed viral load (β = −6, 95% CI, −9.54 to −2.46).
With respect to free estradiol, unweighted analyses indicated lower concentrations at the 75th percentile in women with suppressed viral load compared with women without HIV (β = −0.29, 95% CI, −0.57 to −0.02). Among women with HIV, the 75th percentile was −0.44 pg/mL lower in suppressed compared with unsuppressed women (95% CI, −0.74 to −0.13).
When viral suppression was assessed at the visit prior, this association remained, and the median of free estradiol was additionally lower in suppressed compared with unsuppressed women (β = −0.18, 95% CI, −0.32 to −0.04). Upon accounting for confounding, these associations were no longer statistically significant.
In weighted analyses of SHBG, the 25th and 50th percentile were both statistically significantly higher comparing women with unsuppressed viral load with women without HIV: the 25th percentile was 10 nmol/L higher (95% CI, 2.95 to 17.05), and the 50th percentile was 12 nmol/L higher (95% CI, 3.43 to 20.57). The 75th percentile was also estimated to be 10 nmol/L higher, although this was not statistically significant. The remaining comparisons between women without HIV to women with suppressed viral load were not significant, ranging from 2 to 3 nmol/L. There were no significant differences in SHBG by viral suppression status among women with HIV, although the greatest differences were observed at the 75th percentile of SHBG.
The graphical depiction of each percentile for total estradiol, free estradiol, and SHBG by HIV status, and among women with HIV, viral suppression status at the substudy visit are given in Figure 2. Although the shape of the distribution is similar across groups (right skewed), the distribution of total estradiol among women with HIV who are not virally suppressed is shifted toward lower values. The shape and position of the distribution of free estradiol is very similar comparing women with and without HIV. The shape of the distribution for SHBG is also similar across groups; however, the distribution among women without HIV is shifted toward lower values.
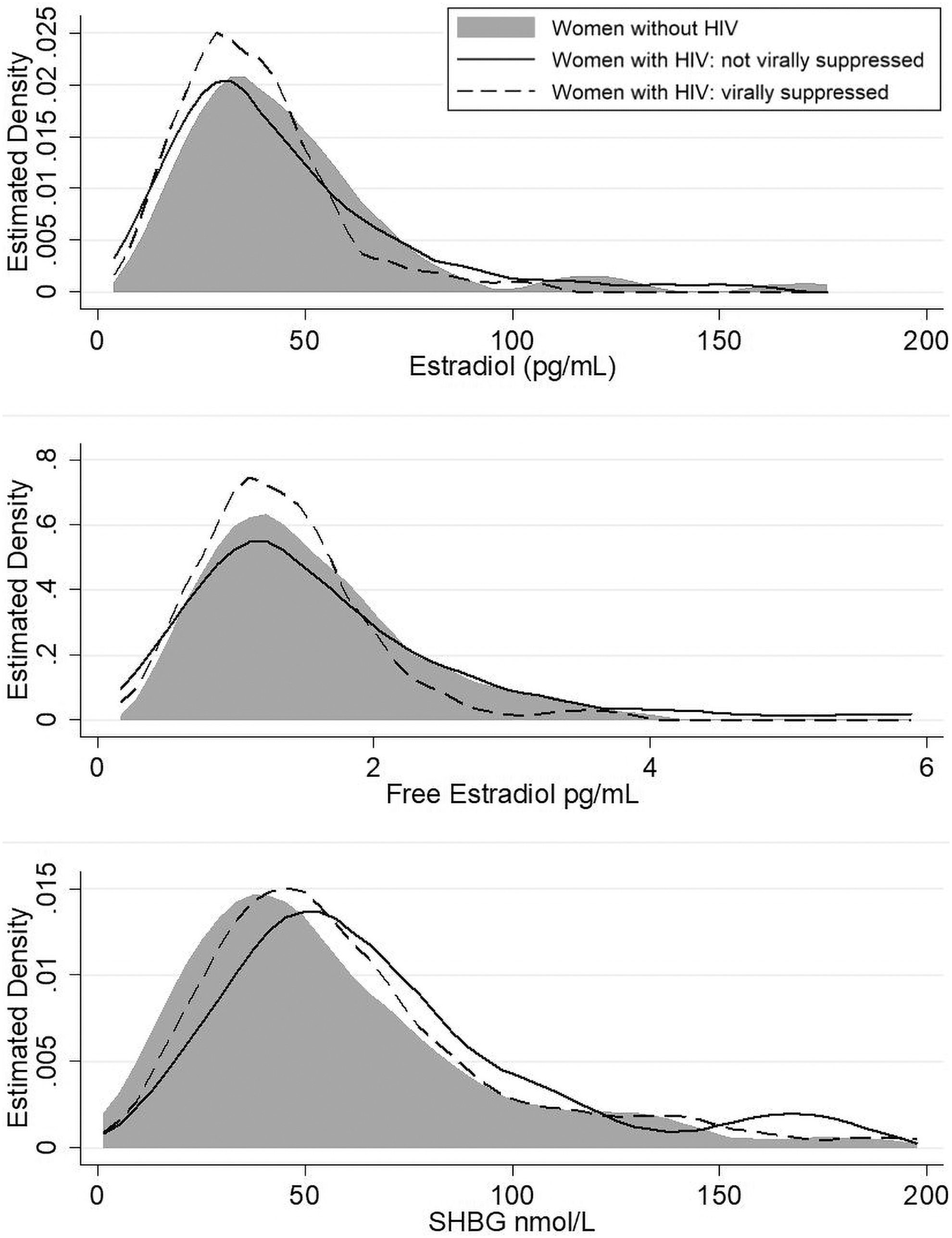
Estimated distribution of total and free estradiol (pg/mL) and SHBG (nmol/L) by HIV status using weighted quantile regression. SHBG, sex hormone binding globulin.
In subgroup analyses among women with total estradiol levels <150 pg/mL, findings were similar (Supplementary Table S1). In subgroup analyses among women who had FSH and inhibin-B data, with FSH <20 pg/mL and detectable inhibin-B, quantile regression estimates were also comparable (Supplementary Table S2). Of note, the median and 75th percentile of free estradiol were significantly lower comparing women with suppressed viral load with women without HIV in these weighted analyses. Among women with HIV, the 50th and 75th percentile of free estradiol were also lower comparing women with suppressed with unsuppressed viral load.
Discussion
In a sample of comparable premenopausal women with and without HIV in the United States, we found no significant differences in free estradiol by HIV status, but some statistically significant differences in total estradiol and SHBG. Specifically, we found lower total estradiol in weighted analyses comparing women with suppressed and unsuppressed viral load with women without HIV. Among women with HIV, there were no differences in total estradiol by suppression status. We also observed higher levels of SHBG comparing women with unsuppressed viral load with women without HIV. There were no significant differences in SHBG by suppression status in women with HIV.
The clinical implications of our findings with respect to adverse health outcomes such as breast cancer or cardiovascular disease in women with HIV remain unclear. High SHBG could lead to lower free estradiol concentrations, which in turn could possibly confer reduced breast cancer risk or increased cardiovascular disease risk over time; however, lower free estradiol was not consistently observed here. Our observations merit further investigation to elucidate the potential clinical impact of these differences in estradiol and SHBG among women with HIV.
Our assessment of total estradiol was comparable to prior works (including prior analyses within the WIHS), where total estradiol ranged from 32 to 48 pg/mL for women without HIV, and 33–43 pg/mL for women with HIV. 36,38 –40 There are few studies in large groups of women that are sociodemographically similar to the WIHS that assess free estradiol and SHBG. Comparability of estradiol and SHBG in women without HIV in our sample with other studies in the United States using early follicular measurements varied.
In two case–control studies assessing breast cancer in the Nurses' Health Study, geometric means for total estradiol were 45 and 51 pg/mL, free estradiol was 0.6 pg/mL in both analyses, and SHBG was 59 and 62 nmol/L. 9,50,51 An analysis from the Harvard Moods and Cycles study found mean early follicular estradiol was 30 pg/mL at baseline. 52
One study from the Study of Women's Health Across the Nation study found mean total estradiol of 76 pg/mL, free estradiol was 0.8 pg/mL, and SHBG of 45 nmol/L among pre/perimenopausal women. 53 Discrepancies may be due to differences in the source populations, the assays used, which may have different reference ranges, or whether protocols allowed random fasting measurements when early follicular was not available. Our observation of significantly lower smoking in women with versus without HIV was driven by the low (33%) proportion observed among women with suppressed viral load. This could be explained by the association demonstrated in prior works between ART adherence, or poor viremic control, and cigarette smoking. 54 –59
We did not find comparable studies using regression to characterize the association between these biomarkers and HIV. Earlier works have generally demonstrated that total estradiol in women with HIV was lower or comparable with women without HIV, 36,38,39 although one study found maximum follicular estradiol was higher in women with HIV (148 pg/mL) compared with women without HIV (111 pg/mL), all of whom reported regular menses. 41 The discrepancy between these findings may be attributed to the timing/assessment of maximum total estradiol over the entire follicular phase or differences in source populations. We have not found comparable studies examining free estradiol.
Higher SHBG levels comparing women with versus without HIV has been reported previously in the WIHS sex steroid substudy (58.5 nmol/L in women with HIV vs. 47.0 nmol/L in women without HIV); however, this has not been replicated elsewhere. 39 The lack of an association between HIV status and free estradiol could also be attributed to selecting women reporting a period in the past 6 months. This selection made our comparison groups more homogenous, and thus, differences in free estradiol could have been obscured.
Our observation that, among women with HIV, total and free estradiol were generally comparable in women with suppressed versus unsuppressed viral load contradicts one study that found that luteal estradiol was higher among women with a lower viral load in women with no ART exposure. 60 This limited difference in estradiol by suppression status we observed may be related to the fact that these women are participating in an interval cohort study and could be generally healthier than the broader population of women with HIV, where there may be larger or qualitative differences in viral suppression as it relates to estradiol.
There are limitations of this analysis that should be considered for future investigations of this association. Our sample size was limited for inferences at the extreme ends of the distribution and should be interpreted cautiously. This is a cross-sectional analysis so we cannot make inferences regarding the association between long-term exposure to HIV and these biomarkers. Exposure and outcome measurement were assessed at single timepoints, which makes them prone to measurement error. Measurement error of estradiol is compounded by using a radioimmunoassay, as opposed to a liquid chromatography with tandem mass spectrometry assay.
Free estradiol was calculated using standard equations assuming a constant for albumin and linear binding affinity of estradiol to SHBG, which may not represent the true relationship between SHBG and estradiol. Inclusion into the substudy could have allowed for perimenopausal women to participate and be included in analyses. Sensitivity analyses were conducted among only women with premenopausal concentrations of FSH and inhibin-B, and findings were robust. Finally, estradiol was measured in 2003–2006 and findings may not be generalizable to women today. This is especially important given integrase inhibitors, the most utilized ART today, have demonstrated increases in weight leading to obesity among women with HIV, 61 –64 which is known to increase estrogen concentrations in the general population, but has unknown impacts on estrogen in women with HIV.
This study represents a novel assessment of estradiol and SHBG by HIV status accounting for confounding by relevant covariates. This work demonstrates the importance of accounting for SHBG when assessing estradiol among women with versus without HIV and motivates further investigation in a larger, contemporary sample. Given the increased risk of hormonally related comorbidities with increasing age, and the shift in the age distribution of women with HIV toward older ages, it is important to understand the distribution of estradiol and SHBG not only among premenopausal women, but also among peri and postmenopausal women with HIV compared with the general population of women. Further research is needed to clarify the clinical implications of difference in estradiol and SHBG among women with HIV versus without across the life course.
Conclusion
Overall, we compared women with and without HIV, and among women with HIV by viral suppression status with respect to total estradiol, free estradiol, and SHBG. When we accounted for demographic, clinical, and lifestyle factors, there were no significant differences by HIV status or viral suppression status for free estradiol. We did observe significantly lower total estradiol and higher SHBG in women with versus without HIV. The clinical implications of these differences remain unclear but should compel further investigation in large contemporary samples of women with and without HIV, across the life course to understand potential differences in these biomarkers in not only premenopausal, but also, peri and postmenopausal women.
Footnotes
Authors' Contributions
S.B.C. was responsible for the conception, analysis and drafting of the article. T.T.B., K.N.A., and B.L. made substantial contributions to the design, analysis, and interpretation of this work in addition to critically revising this article. J.D.O., M.L.A., C.A.M., L.R., E.L., L.S.M., D.S., K.G.M., H.M., K.M., and K.V. made substantial efforts to critically revise this article and contributed greatly to the interpretation of the findings. All co-authors listed have reviewed and approved this article before submission. This article has been solely submitted to the Journal of Women's Health and is not published, in press, or submitted elsewhere.
Acknowledgment
The authors gratefully acknowledge the contributions of the study participants and dedication of the staff at the MWCCS sites.
Author Disclosure Statement
T.T.B. has served as a consultant to Gilead Sciences, Merck, Janssen, ViiV Healthcare, and Theratechnologies. All other co-authors have no conflicts of interest to report.
Funding Information
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D'Souza, Stephen Gange and Elizabeth Golub), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen and Audrey French), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, Jodie Dionne-Odom, and Deborah Konkle-Parker), U01-HL146192; UNC CRS (Adaora Adimora), U01-HL146194.
The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), National Institute On Aging (NIA), National Institute of Dental and Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR).
MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), UL1-TR003098 (JHU ICTR), UL1-TR001881 (UCLA CTSI), P30-AI-050409 (Atlanta CFAR), P30-AI-073961 (Miami CFAR), P30-AI-050410 (UNC CFAR), P30-AI-027767 (UAB CFAR), and P30-MH-116867 (Miami CHARM). Other funding sources include F31CA247610, K23HL152903, KL2TR001432, K24AI120834, and R01-CA250851.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.