
Abstract
Background:
There are limited data on sex difference in patients with hypertensive crisis. We investigated sex differences in characteristics and long-term mortality in patients with hypertensive crisis visiting the emergency department (ED).
Materials and Methods:
This cross-sectional study at a tertiary referral center included patients ≥18 years of age who were admitted to the ED between 2016 and 2019 with hypertensive crisis, defined as systolic blood pressure ≥180 mmHg and/or diastolic blood pressure ≥110 mmHg.
Results:
Among the 6,467 patients who visited the ED with hypertensive crisis, 3,131(48.4%) were women. Women were older and less likely to have acute hypertension-mediated organ damage than men. The 3-year all-cause mortality did not differ between women and men (16.9% in women and 17.2% in men, p = 0.738). After adjusting for age and comorbidities, the 3-year all-cause mortality was significantly higher in men than in women (hazard ratio [HR], 1.14; 95% confidence interval [CI], 1.01–1.29; p = 0.031). In particular, among patients ≥50 years of age, the 3-year all-cause mortality was significantly higher in men than in women (HR, 1.14; 95% CI, 1.01–1.29; p = 0.038); however, it was not different according to sex among patients 18–49 years of age. Moreover, the 3-year all-cause mortality was significantly higher in men than in women among patients with hypertensive urgency (HR, 1.59; 95% CI, 1.34–1.90; p < 0.001), which was reversed in patients with hypertensive emergency (HR, 0.71; 95% CI, 0.60–0.84; p < 0.001).
Conclusions:
Men ≥50 years of age with hypertensive crisis, men with hypertensive urgencies, and women with hypertensive emergencies have a high risk of all-cause mortality. Thus, it is necessary to consider sex differences when predicting subsequent prognosis and determining the appropriate treatment for patients with hypertensive crisis.
Introduction
Hypertension contributes significantly to cardio-cerebrovascular and renal morbidity and mortality, 1 and the prevalence of hypertension is increasing in both women and men in all age groups. 2
The prevalence, awareness, treatment, and control rates of hypertension differ greatly between women and men. It has been established that men have a higher prevalence of hypertension than women before the onset of menopause, after which women display a more rapid increase in the prevalence of hypertension than men, eventually exceeding that in men. 3 –6 Moreover, in a population-based prospective study, the risk of cardiovascular disease morbidity or mortality was significantly higher in men with hypertension than in women with hypertension, and this sex gap was reduced with advancing age. 7 Despite these differences between men and women with hypertension, current hypertension guidelines rarely consider sex differences in hypertension management.
Hypertensive crisis is defined as a severe and abrupt elevation of blood pressure (BP) and is classified into hypertensive emergency and hypertensive urgency based on the presence or absence of acute hypertension-mediated organ damage (HMOD). 8 This situation is a sign of poorly controlled hypertension, which can lead to numerous complications, including myocardial infarction, heart failure, stroke, and kidney disease, and requires rapid diagnostic evaluation and prompt treatment. Hypertension awareness, treatment, and control have slightly increased in recent years; however, the prevalence of hypertensive crisis is still high and associated with a high mortality.
According to a previous study, the risk factors possibly promoting a hypertensive crisis include female sex, higher degrees of obesity, hypertension or coronary heart disease, higher number of antihypertensive drugs, and nonadherence to medication. 9 Moreover, according to a previous systematic review, hypertensive emergencies are more common in men and older patients than other individuals. 10 However, there are limited data on sex differences in the characteristics and clinical outcomes of patients with hypertensive crisis. In this study, we aimed to investigate sex differences in clinical profiles and all-cause mortality in patients with hypertensive crisis in an emergency department (ED).
Materials and Methods
Study population
This observational, cross-sectional study was conducted at single regional emergency medical centers affiliated with the academic university hospital in Guri, Gyeonggi-do, Korea. We reviewed the medical records of 172,105 patients ≥18 years of age who visited the ED of this center between January 2016 and December 2019. We included patients diagnosed with hypertensive crisis, which was defined as systolic blood pressure (SBP) ≥180 mmHg and/or diastolic blood pressure (DBP) ≥110 mmHg (Fig. 1).
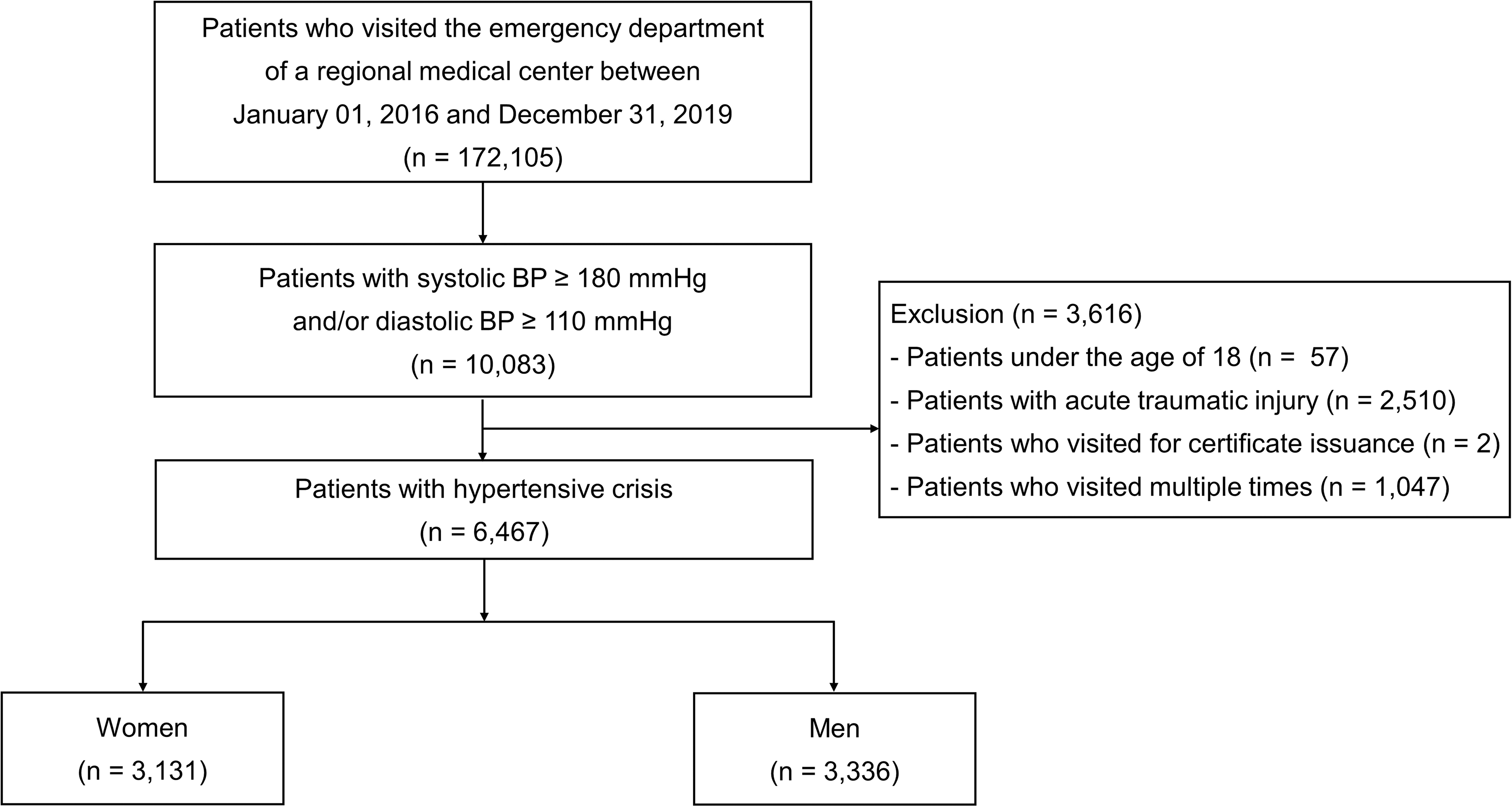
Study flowchart.
Data collection and outcomes
The design, eligibility criteria, collected data, and detailed descriptions of the definitions of acute HMOD and comorbidities in our study have been published previously. 11 Briefly, data were collected using electronic medical records by trained data collectors under the supervision of the principal investigator. The collected data included demographic and clinical characteristics, comorbidities, BP, distributions of acute HMOD, the findings of diagnostic tests performed in the ED, and events during the hospitalization and follow-up periods (e.g., admission and readmission, discharge, ED revisits, and death). Enrolled patients were followed up until death from any cause or the end of the study (March 2021). The incidence of death and its timing were extracted from the National Health Insurance Service in South Korea.
The study was reviewed and approved by the Institutional Review Board (IRB) of the researchers' affiliated university hospital (GURI 2020-01-028) and conducted in accordance with the Declaration of Helsinki. The IRB waived the requirement for written informed consent.
Statistical analyses
Quantitative data are presented as mean and standard deviation. Categorical variables are expressed as absolute (counts) and relative frequencies (percentages). For the univariate comparison of continuous variables, a t-test was used for two independent samples. For the univariate comparison of categorical data, chi square tests were used. We evaluated the differences in baseline characteristics, distribution of acute HMOD, and outcomes between women and men. For subgroup analysis, we stratified the study patients according to the presence of acute HMOD and different age groups (18–49 and ≥50 years).
Kaplan–Meier survival analysis and log-rank tests were used to compare 3-year all-cause mortality between women and men in all patients and each subgroup. Hazard ratios (HRs) and respective 95% confidence intervals (CIs) for 3-year all-cause mortality in men compared with women were calculated using multivariable Cox regression.
Multivariable Cox regression models assessed the association between sex and 3-year all-cause mortality, adjusting for age and comorbidities, including hypertension, diabetes mellitus, coronary artery disease, and chronic kidney disease. Likewise, subgroup analyses were performed by controlling for the same covariates. All tests were two tailed, and statistical significance was set at p < 0.05. All analyses were performed using the Statistical Analysis Software package (SAS version 9.4; SAS Institute, Cary, NC).
Results
Baseline characteristics and presenting symptoms
A total of 6,467 patients were analyzed in the study, and median follow-up period was 3.1 years (interquartile range, 2.0–4.1). Among the study patients, 3,131 (48.4%) were women and 3,336 (51.6%) were men. Women were significantly older than men (mean age: 64.7 vs. 58.3 years; p < 0.001).
Table 1 displays the sex differences in baseline characteristics and presenting symptoms. Compared with men, women had significantly more comorbidities such as hypertension, dyslipidemia, and heart failure. Furthermore, men were significantly more likely to be current smokers and alcohol drinkers than women. Men had a higher rate of not taking antihypertensive drugs than women (33.8% vs. 27.4%; p < 0.001) among patients with previously diagnosed hypertension. The mean DBP was higher in men than in women (109 vs. 106 mmHg; p < 0.001), but the mean SBP did not differ between the groups (190 vs. 190 mmHg; p > 0.05).
Baseline Characteristics
Data are presented as n (%) or mean (SD), as appropriate.
Proteinuria was defined as dipstick urinalysis result ≥1+.
BNP, B-type natriuretic peptide; CT, computed tomography; DBP, diastolic blood pressure; ECG, electrocardiography; eGFR, estimated glomerular filtration rate; Hb, hemoglobin; HMOD, hypertension-mediated organ damage; LVH, left ventricular hypertrophy; SBP, systolic blood pressure; SD, standard deviation.
Compared with men, women had a significantly lower estimated glomerular filtration rate (78.2 vs. 79.9 mL/min/1.73 m2; p = 0.047) and hemoglobin level (12.7 vs. 14.3 g/dL; p < 0.001). Troponin-I, B-type natriuretic peptide (BNP), and D-dimer levels were not significantly different between the groups. A higher frequency of proteinuria on dipstick urinalysis, left ventricular hypertrophy (LVH), myocardial ischemia on electrocardiography (ECG), and abnormal findings on brain imaging was noted in men than in women. In contrast, a higher frequency of cardiomegaly on chest radiography was noted in women than in men. Women frequently presented with dizziness (15.0%), focal neurologic deficit (12.8%), dyspnea (12.1%), and headache (10.1%), whereas men frequently presented with focal neurologic deficits (15.5%), dyspnea (12.5%), chest pain (11.7%), and dizziness (8.7%).
Acute HMOD, such as hypertensive encephalopathy, cerebral infarction, intracerebral hemorrhage, retinopathy, acute heart failure, acute coronary syndrome, acute renal failure, and aortic dissection, was more frequently observed in men than in women (34.1% vs. 26.9%; p < 0.001). Regarding the distribution of acute HMOD, a higher proportion of acute heart failure (26.9% vs. 18.0%) and subarachnoid hemorrhage (SAH) (7.7% vs. 4.0%) was observed in women than in men; otherwise, a higher proportion of acute coronary syndrome was observed in men than in women (26.3% vs. 8%; Table 2).
Distribution of Acute Hypertension-Mediated Organ Damage
Data are presented as n (%).
We performed additional analyses to understand the sex differences in the characteristics of the patients who expired (Supplementary Table S1). In terms of those with smoking and drinking abuse, lower estimated glomerular filtration rate levels, and no antihypertensive drug intake, more men than women died within 3 years. Conversely, women were older, had more cardiovascular risk factors (e.g., hypertension, diabetes mellitus, and heart failure), and had a higher proportion of acute HMOD than did men.
The baseline characteristics of women and men stratified by age group (18–49 and ≥50 years) are shown in Supplementary Table S2. In the younger age group (18–49 years), there was no difference in the prevalence of comorbidities between men and women, but in the older age group (≥50 years), the prevalence of heart failure was higher in women and that of chronic kidney disease was higher in men.
In both age groups, the rates of current smokers and alcohol drinkers; levels of serum creatinine; and frequency of LVH, brain imaging abnormality, and acute HMOD were higher in men than in women. In particular, the proportion of patients diagnosed with hypertension and dyslipidemia was significantly lower in men than in women in older age groups than in younger age groups. In addition, the proportion of patients who did not take antihypertensive drugs among patients with previously diagnosed hypertension was higher in men than in women in all age groups, but the difference was lower in the older age group than in the younger age group.
The baseline characteristics of women and men stratified by the presence of acute HMOD are presented in Supplementary Table S3. The overall trend was similar to that observed in overall patients. Cardiovascular risk factors, such as hypertension, diabetes mellitus, and dyslipidemia, and comorbidities, such as stroke, coronary artery disease, heart failure, and chronic kidney disease, were higher in patients with hypertensive emergency than in those with hypertensive urgency, regardless of sex. The rate of being diagnosed with hypertension and not taking antihypertensive drugs was higher in men than in women in both groups.
In particular, in the hypertensive emergency group, the incidence of abnormal findings on chest radiograph, such as cardiomegaly or pulmonary congestion, as well as hypertension and heart failure was higher in women than in men. However, in the hypertensive urgency group, the incidence of proteinuria and LVH on ECG was higher in men than in women.
Sex differences in clinical course and all-cause mortality during the follow-up period
Overall, 2,975 (46.0% [43.9% women vs. 48.0% men; p < 0.001]) patients were admitted, 5,115 (50.1% [46.5% women vs. 40.8% men; p < 0.001]) patients were discharged, 959 (9.4% [9.5% women vs. 11.1% men; p = 0.038]) patients were discharged against medical advice, and 7 (0.1% [0.1% women vs. 0.2% men; p = 0.293]) patients died in the ED. The overall rates of ED revisits within 1 month, 3 months, and 1 year were 9.6%, 16.8%, and 29.3%, respectively. The overall readmission rates within 1 month, 3 months, and 1 year were 6.1%, 9.0%, and 13.7%, respectively. There were no differences in the rates of ED revisits and readmissions between women and men (Supplementary Table S4).
During the follow-up period, the unadjusted 3-year all-cause mortality was not significantly different according to sex (Fig. 2A). After stratification according to age, men ≥50 years of age had a higher 3-year all-cause mortality than women ≥50 years of age (23.5% vs. 20.4%; p = 0.009); however, there was no sex difference among younger patients (18–49 years of age, 3.2% vs. 2.1%; p = 0.218) (Fig. 2B). Kaplan–Meier curves for the cumulative mortality according to the presence of acute HMOD revealed that 3-year all-cause mortality was significantly higher in men than in women among patients with hypertensive urgency (13.8% vs. 10.4%; log-rank p < 0.001), which was reversed in patients with hypertensive emergency (23.8% vs. 34.3%; log-rank p < 0.001; Fig. 2C).
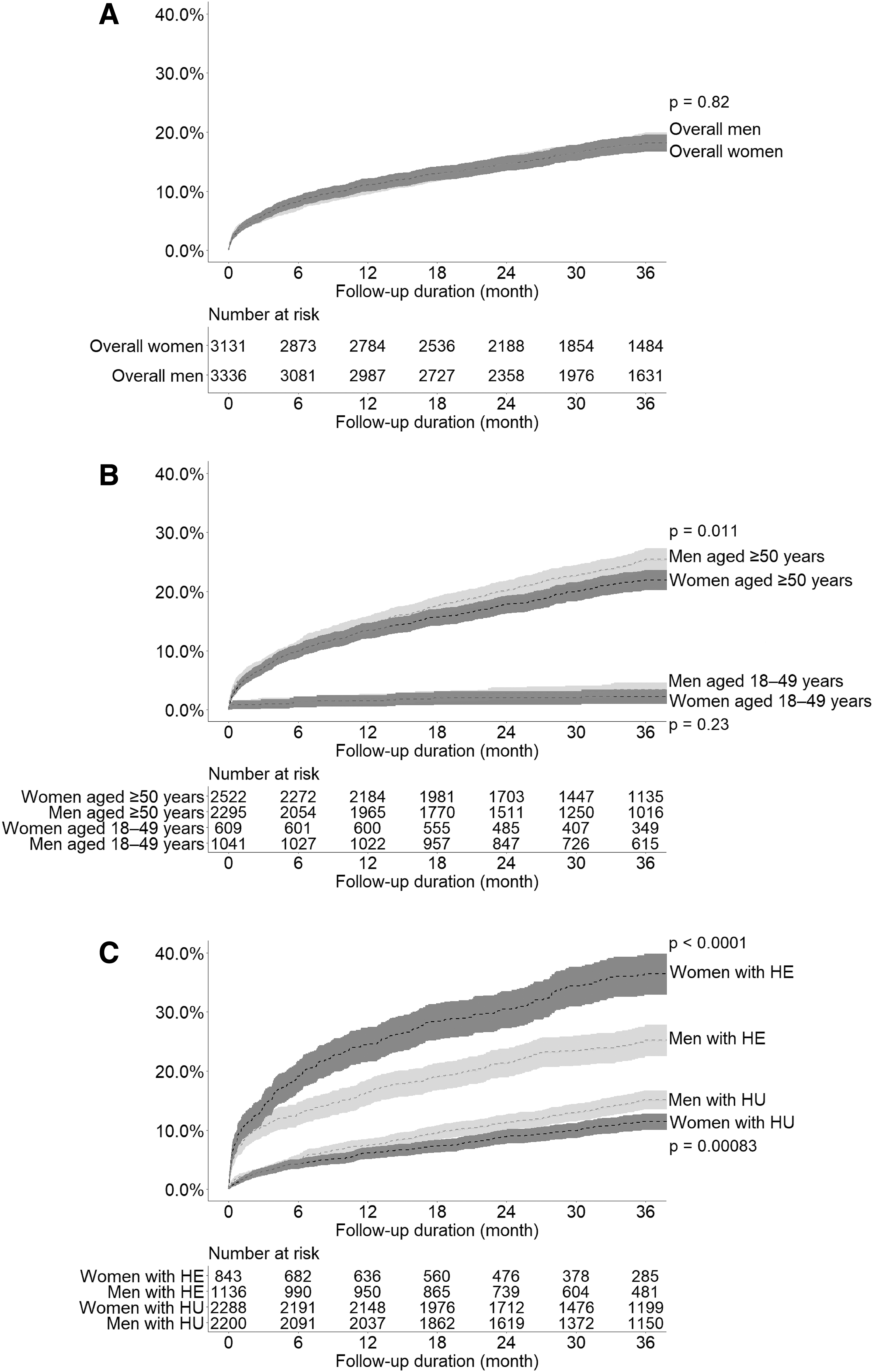
Sex difference in cumulative all-cause mortality in
In the multivariable Cox regression model, men had a higher 3-year all-cause mortality after adjusting for age and comorbidities in all patients (HR, 1.14; 95% CI, 1.01–1.29; p = 0.031). Among patients ≥50 years of age, men had a higher 3-year all-cause mortality than women (HR 1.14; 95% CI, 1.01–1.29; p = 0.038); however, there was no sex difference in 3-year all-cause mortality among patients 18–49 years of age (HR, 1.50; 95% CI, 0.77–2.93; p = 0.234). In the subgroup analysis stratified according to the presence of acute HMOD, women had a higher risk of all-cause mortality than men among patients with hypertensive emergency (HR, 0.71; 95% CI, 0.60–0.84; p < 0.001). In contrast, among patients with hypertensive urgency, men had a higher risk of all-cause mortality than women (HR, 1.59; 95% CI, 1.34–1.90; p < 0.001; Table 3).
Sex Differences in All-Cause Mortality Rates and Hazard Ratios for Mortality Among Patients with Hypertensive Crisis
Data are presented as n (%).
Adjustment for age, medical history of hypertension, diabetes mellitus, coronary artery disease, and chronic kidney disease.
Adjustment for medical history of hypertension, diabetes mellitus, coronary artery disease, and chronic kidney disease.
CI, confidence interval; HR, hazard ratio.
Discussion
We investigated sex differences in the clinical characteristics and long-term mortality of patients with hypertensive crisis visiting the ED. The major findings of this study are as follows: (1) among patients with hypertensive crisis, men had a higher frequency of acute HMOD than women, although women were older and had significantly more comorbidities than men; (2) overall 3-year all-cause mortality was higher in men than in women with hypertensive crisis after adjusting for age and comorbidities, which were prominent in patients ≥50 years of age; (3) the 3-year all-cause mortality was significantly higher in men than in women among patients with hypertensive urgency; and (4) women had a higher risk of all-cause mortality than men among patients with hypertensive emergency.
Sex differences in BP were first reported in 1947 among university students; men had consistently higher BP than women. 12 It is well established that men have a higher prevalence of hypertension than women before the onset of menopause, after which women display a more rapid increase in the prevalence of hypertension relative to men, eventually exceeding that in men. 4,6,13 Moreover, in studies using large population data, men had a lower awareness, treatment, and control of hypertension than women in younger age, and these sex difference decreased in older age. 3,14 –16 A similar trend was observed in our study of patients with hypertensive crisis. Among patients 18–49 years of age, men had a higher frequency of hypertension and a higher rate of not taking antihypertensive drugs than women; these findings were reversed or diminished in patients ≥50 years of age.
Generally, women with hypertension have better cardiovascular outcomes than men with hypertension, and this trend tends to be larger in younger age groups as premenopausal women are relatively protected against cardiovascular disease compared with age-matched men. 17,18 Quan et al. reported that women with hypertension had lower mortality and cardiovascular outcomes than men, regardless of ethnicity. 19 Daugherty et al. also demonstrated that women were less likely to develop cardiovascular outcomes and had a lower risk of mortality than men. 20 Furthermore, according to data from the National Health and Nutrition Examination Survey (NHANES) I (1971–1975) and NHANES III (1988–1994), mortality rates were higher among men than among women with hypertension. 21 However, this mortality difference reduced with advancing age. 7
Epidemiologic and outcome data regarding sex differences are limited in hypertensive crisis. A previous study using nationwide inpatient sample data, focusing on the frequency of hospitalizations for a hypertensive emergency, showed that women were more likely to be hospitalized for hypertensive emergencies than men, but all-cause in-hospital mortality was higher in men than in women. 22
Our study demonstrated that men had a higher risk of long-term mortality than women among patients with hypertensive crisis, especially among those ≥50 years of age. There are a few possible explanations for this finding. First, men had a higher frequency of acute HMOD, specifically, acute coronary syndrome. Second, men had more cardiovascular risk factors, such as dyslipidemia, smoking, and alcohol consumption. Third, more men were hypertensive with de novo manifestations of hypertension and no antihypertensive medication intake. Fourth, men more frequently showed findings of subclinical HMOD such as proteinuria, LVH, or myocardial ischemia on ECG than women. Subclinical HMOD is associated with a risk of cardiovascular mortality and morbidity. 23,24
These results suggest that in men experiencing a hypertensive crisis, especially those ≥50 years of age, evaluation of subclinical HMOD should be actively performed even if there is no evidence of acute HMOD and intensive short-term follow-up is required. Finally, men exhibited higher DBPs than did women. However, since there were no sex differences in terms of SBP, we assume that other factors, including age, comorbidities, and presence of subclinical and acute HMOD, may contribute more to long-term prognoses than will absolute BP values. Further studies are needed on the sex differences in long-term prognosis according to SBP and DBP values.
Furthermore, sex differences in mortality in hypertensive crisis may have been related to adherence to regular outpatient follow-up and appropriate treatment. However, we did not include data on outpatient follow-up and adherence to antihypertensive medications. Further studies are needed to clarify the sex differences in optimal screening, risk stratification, treatment strategy, and follow-up interval, as they are related to the short-term and long-term clinical outcomes in patients with hypertensive crisis.
Sex differences in hypertensive emergencies showed different patterns in the groups described above. A hypertensive emergency is defined as a situation in which a patient with a hypertensive crisis has evidence of progressive acute HMOD caused by a rapid rise in BP. International guidelines focus more on hypertensive emergencies than on hypertensive urgencies because patients with the former are prone to high mortality and immediate BP reduction is required to limit extension or promote regression of acute HMOD. 25
In this study, acute HMOD was observed more frequently in men than in women, but the all-cause mortality was higher in women than in men among patients with acute HMOD. A possible explanation for this finding is that among patients with hypertensive emergencies, women had a higher frequency of medical history of heart failure and had worse findings related to heart failure, such as higher level of BNP, and higher frequency of cardiomegaly or pulmonary congestion on chest radiograph, than men.
Regarding the distribution of acute HMOD, a significantly higher prevalence of acute heart failure was observed in women than in men. Furthermore, women more frequently developed SAH than men in this study. Since both heart failure and SAH have high mortality rates, 26,27 the higher incidence of these diseases could have affected the higher mortality rate in women than in men with hypertensive emergencies.
Another possible explanation is the sex-related differences in the symptom perception and care-seeking behavior. Previously, Zrelak 28 reported significant sex-based differences in terms of time to presentation, symptom perception, disease knowledge, decision making, and bystander roles in acute stroke patients. We also revealed sex-related differences in presenting symptoms, including headache, dizziness, focal neurologic deficits, and chest pain. Further studies are needed to better understand the observed difference in prognosis in patients with hypertensive crisis between sexes and how both pathophysiology and treatments contribute to this.
Although substantial progress has been made regarding sex difference in cardiovascular disease, 29 most guidelines still recommend similar treatment for women and men with hypertension in all age groups without detailed descriptions on management in both sexes. In particular, studies on sex differences in hypertensive crisis are very limited. From this perspective, our study could provide some evidence on sex differences in hypertensive crisis and is expected to highlight the need for more attention and research on these issues.
The present study has several limitations. First, this was a retrospective study. Although the study was based on reliable registry data and electronic medical charts, compared with the accuracy and completeness of data used in prospective studies, those of the retrospective data on baseline characteristics and diagnostic test findings were insufficient.
Second, as the status of BP control in the ED and after discharge were not obtained, further analysis on the outcomes according to the BP control patterns was limited. Future research regarding the role of achieving target BP values and follow-up strategies after ED visits is needed. Third, we could not obtain data on socioeconomic status, such as marital status, education, and income status. Fourth, the study included data from a single center, which may not be representative of the entire population. Additionally, data on ED revisits and readmission rates may have been underestimated.
Finally, we did not obtain data on cardiovascular events, such as myocardial infarction, stroke, and heart failure, and cause of death, such as deaths from cardiovascular disease or cancer because the National Health Insurance Service data did not provide these information. However, data regarding all-cause mortality and date of death were highly accurate because they were obtained from the National Health Insurance Service, which covers the entire population of Korea.
Conclusions
There were significant sex differences in the 3-year all-cause mortality in patients with hypertensive crisis. Men with hypertensive crisis had an increased risk of all-cause mortality than women, especially among patients ≥50 years of age. Moreover, the all-cause mortality was significantly higher in men than in women among patients with hypertensive urgency; however, it was significantly higher in women than in men among patients with hypertensive emergency. Based on our results, sex-specific approaches regarding continuous monitoring, appropriate treatment, and regular follow-ups are required for patients with hypertensive crisis.
Footnotes
Authors' Contributions
Study conception and design: J.-H.S. Acquisition of data: B.S.K. and H.-J.K. Statistical analysis: J.H.L. Interpretation of data: W.K. and J.-K.P. Draft of article: B.S.K. and H.-J.K. Critical revisions: J.-H.S. and J.S. All authors have approved the final version of the article, including the authorship list.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.