
Abstract
Since the Dobbs decision to overturn Roe v Wade last summer in the United States, reproductive rights have grown increasingly salient in medical ethics. Here, we argue that political or governmental restriction of access to evidence-based health care, including abortion, is unethical for three reasons; namely, it violates the autonomy of pregnant persons, exposes women to harm (particularly with respect to cardiovascular disease [CVD] and cancer), and exacerbates systemic inequity and injustice.
Before expanding upon the ethical violations that such restriction would entail, it is important to address the question of the moral status of the fetus. While it is intellectually easiest to demarcate the bestowal of personhood at the moment of conception or alternatively at the moment of birth, this oversimplifies what for many people is a more complex reality. If we interrogate our moral intuition using the thought experiment of a rapidly sinking ship with a 1-month-old baby at the bow and a frozen test tube containing five fertilized embryos at the stern, and we only have time to rescue one before escaping to a lifeboat, it is hard to imagine that anyone would argue for any course of action other than saving the baby.
It is intuitive for most that the baby has a moral claim to personhood that goes well beyond that of an embryo. Similarly, we recognize that the loss of an intended pregnancy carries a degree of gravitas commensurate with its stage of development. While the loss of an embryo at 7 weeks gestation may be sad, the demise of a fetus at 5 months gestation is a tragedy, and the death of a 1-year-old child is a devasting event that completely changes the lives of parents.
We find it helpful to consider the concept of liminality, as described by the anthropologist Victor Turner, to capture this critical nuance. This term is often applied to rites of passage during adolescence, a period during which an individual is neither a child nor an adult. While legal adulthood in the United States is conferred at age 18, the more complex reality is that social and cultural adulthood are recognized gradually through the period of late teenage years to mid-twenties. Similarly, we argue that embryonic and fetal life exist in the liminal space between the complete lack of personhood that exists before the moment of conception and the full conferral of personhood that occurs at the moment of birth.
It is worth noting that society places a high symbolic value on an individual's date of birth rather than date of fertilization or implantation as the defining moment of when one's personhood is recognized and celebrated yearly thereafter. Regardless, the moral status of the fetus is ultimately a metaphysical question that science alone cannot decide, and some people will always believe that personhood begins at conception. Since it is unlikely that our pluralistic society will ever achieve a consensus on this question that is influenced so heavily by personal values, it seems only rational to leave it to the pregnant person herself to decide when her fetus can also claim the right to personhood before birth.
Indeed, the imposition of civil or criminal penalties to force women to continue a pregnancy against their will is a violation of their autonomy, a moral agent's right to self-determination or self-governance. Even if one does grant the fetus a full claim to personhood, there is a clear ethical precedent that prohibits individuals from being forced to use their bodies in a way that violates their autonomy, even to save a life.
If a person is gravely ill and in desperate need of a bone marrow transplant, one cannot compel her brother to donate his bone marrow even if he is the only identifiable match and the patient will almost certainly die without it. While most would agree that it would be supererogatory or laudable for the brother to donate if it would not cause him demonstrable harm, few would argue that he should be obligated to do so under threat of civil or criminal penalties should he refuse.
Furthermore, abortion is a medical intervention that is a critical component of comprehensive reproductive health care. The term “pro-life” as it is currently deployed is disingenuous, as it actually describes a “pro-forced-birth” or “anti-choice” stance that may in fact be “anti-life” with respect to the pregnant person and her family. Pregnancy itself carries non-negligible risks of morbidity and mortality, even in healthy women. According to the CDC, the maternal mortality rate in the United States was 24 deaths per 100 thousand live births in 2020, compared with 0.4 deaths per 100 thousand abortions, which represents a staggering 60-fold difference. 1 This risk is compounded with age, with maternal mortality as high as 108 deaths per 100 thousand live births for women 40 years of age and older. 1
Certain pre-existing conditions increase this risk substantially, most notably CVD. CVD accounts for one in four maternal deaths and is a leading cause of death during pregnancy and within the first postpartum year. 2 However, there is a subset of patients for whom pregnancy-related mortality risk can exceed 50%, including previous peripartum cardiomyopathy with residual left ventricular (LV) dysfunction, severe LV dysfunction, severe LV obstruction, pulmonary arterial hypertension, and inherited aortopathy with dilated aorta. 3 If patients with these conditions become pregnant, termination should be offered as a treatment option to preserve maternal life and health. 4 There are many other cardiovascular conditions for which pregnancy is not contraindicated, but still carries significantly elevated risk of pregnancy-related death, including mechanical valves, repaired complex congenital heart disease (CHD), and hypertrophic cardiomyopathy.
Furthermore, rates of pregnancy-related cardiovascular complications such as cardiac arrest, arrhythmia, acute myocardial infarction, and aneurysm/dissection have increased 100%–175% in the past decade, despite advances in pregnancy-related medical expertise. 5 Accordingly, access to comprehensive counseling about reproductive choices and safe abortion care is essential for the management of pregnancy in patients with concomitant maternal CVD.
In addition, the development of certain conditions can pit the survival of the fetus against the survival of the pregnant person. For women diagnosed with cancer, administration of curative treatment is often unsafe for the fetus, particularly in the first trimester. 6 For some diseases, such as acute promyelocytic leukemia (APL), a delay of instituting curative chemotherapy even for a few days could result in maternal death. In contrast, this fatal cancer is highly treatable and curable when therapy is given as soon as the disease is diagnosed. 7 However, the mainstay of therapy for APL is all-trans retinoic acid, for which the prescribing information warns of “a high risk that a severely deformed infant will result if tretinoin capsules are administered during pregnancy.” Similarly, early-stage breast cancer is highly curable when appropriate therapy is given.
For the most aggressive types of breast cancer, treatment with targeted therapies (such as trastuzumab for HER2-positive breast cancer and pembrolizumab for triple negative breast cancer) cannot be given safely at any point during pregnancy due to adverse fetal effects. Likewise, endocrine therapy that targets the estrogen receptor is not safe at any point during pregnancy. 8 Delaying otherwise indicated cancer treatment can increase the risk of cancer recurrence and death. Although not all patients in these circumstances would choose to terminate, the restriction of comprehensive options may reduce the survivability of women who present with cancer, while pregnant. While other types of chemotherapy can be given during the second and third trimesters without the risk of fetal malformations, they may nonetheless confer increased risk of obstetrical complications. 9
These are extremely complex situations, decisions regarding which patients should be able to make with their physicians, considering the desire of the patient to preserve the pregnancy, the oncologic risks incurred from a delay in therapy, the uncertainty regarding long-term fetal/neonatal outcomes related to treatment choices, and the timing of the diagnosis. For example, a woman with three small children at home may prioritize her own survival to maximize her chance of being alive to raise them, while a woman who has struggled to become pregnant after many failed attempts might embrace a different calculus. Regardless, these intensely personal decisions should be made based on the best available scientific evidence, the specific medical facts of each individual case, and the pregnant person's own goals and values.
Many medical societies have issued statements expressing concern about the negative health consequences of the Dobbs decision or expressing explicit support of abortion rights underscoring the primacy of the health of pregnant persons, including the American Medical Association (AMA), American College of Physicians (ACP), American College of Obstetricians and Gynecologists (ACOG), Society for Maternal-Fetal Medicine (SMFM), American Academy of Family Physicians (AAFP), American Academy of Pediatrics (AAP), American Psychiatric Association (APA), American College of Cardiology (ACC), and American Society of Clinical Oncology (ASCO). Notably, the AMA statement highlights the additional issue of injustice: “Access to legal reproductive care will be limited to those with sufficient resources, circumstances, and financial means to do so—exacerbating health inequities by placing the heaviest burden on patients from Black, Latinx, Indigenous, low-income, rural, and other historically disadvantaged communities who already face numerous structural and systemic barriers to accessing health care.” 10
Indeed, women of color face higher risks of pregnancy-related morbidity and mortality, largely due to structural racism and social determinants of health. 11 The overall risk of pregnancy-related death is three to four times higher for Black women than White women in the United States 12 ; according to the CDC, the maternal mortality rate for Black women in 2020 was 55 deaths per 100 thousand live births. 1 Restrictions on abortion access do not eliminate abortion, but rather they eliminate safe abortions for already vulnerable populations. According to ACOG, “approximately 21 million women around the world obtain unsafe, illegal abortions each year, and complications from these unsafe procedures account for approximately 13% of all maternal deaths, nearly 50,000 annually.” 13
Conversely, many safe abortion options exist under the appropriate supervision of health care providers, including self-administered medication with telemedicine support. 14 Even in the pre-Dobbs era, restrictive abortion policies designed to limit access have been associated with higher maternal mortality rates. 15 However, in the post-Dobbs era, women without the resources to travel are even more vulnerable to the vagaries of their state laws to determine what therapeutic choices are available to them or even what options can be discussed. Figure 1 shows the rates of maternal mortality by state, which has over a tenfold variation between California with the lowest (4 per 100 thousand) and Louisiana with the highest (58 per 100 thousand). Notably, only states that have chosen not to expand Medicaid are likely to restrict abortion, and this “double hit” appears to correlate with higher maternal mortality regardless of state poverty rate.
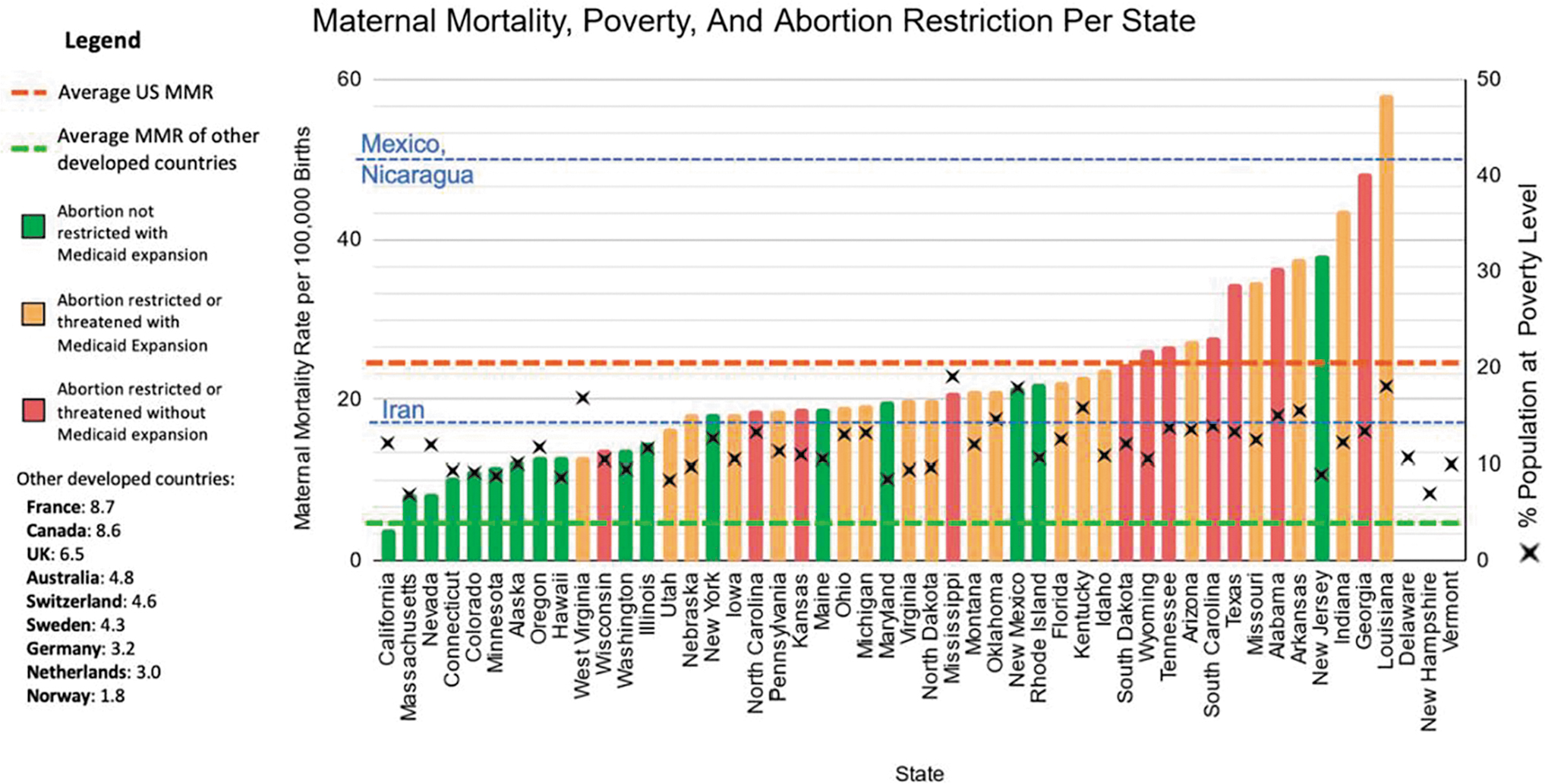
Maternal mortality rate by state (y axis on the left). 20 Colors indicate the presence of state abortion restrictions 21,22 and Medicaid expansion. 23 The red line represents average maternal mortality rate for the United States in 2020 from the CDC. 1 Blue lines represent other countries' maternal mortality rates for comparison. 24 The green line represents the average maternal mortality rate for other developed nations. 25 The percent of the population at the poverty level is marked with an X and refers to the y axis on the right.
From a justice standpoint, some abortion opponents might express concern that overly permissive abortion policy could promote a form of ableist eugenics by selectively terminating pregnancies with fetal abnormalities. However, this criticism ignores the fact that people with disabilities may be at increased risk of pregnancy-related morbidity or mortality themselves, 16,17 and limiting abortion access may in fact harm them as adults. For example, children with trisomy 21 have an elevated risk of CHD, and those with CHD who survive to adulthood and become pregnant may face an increased risk of pregnancy-related adverse cardiovascular outcomes for which termination may be their safest option.
Therefore, while we recognize the validity of good faith concerns regarding ableism, we would argue that the answer is not to force women to carry undesired pregnancies, but rather to reshape social and economic policies such that families feel they can better care for children—especially those with special needs.
Indeed, rather than attempting to control women's reproductive choices, violating their autonomy and forcing them to bear increased risk of pregnancy-related harm, we should aim to reshape choice architecture through implementation of policies that are truly pro-life for everyone at all stages of the life cycle. It should be a common and undisputed goal to reduce unwanted pregnancies through ensuring better contraceptive education and access; this has been clearly demonstrated to reduce unintended pregnancies, 18 which account for nearly half of pregnancies in the United States. 19 Furthermore, recognizing the liminal degree of personhood many ascribe to fetal life, it would seem laudable to promote policy changes that may ease the burdens of parenting to make it a more feasible choice. These might include universal parental leave, universally available childcare commensurate with the needs of each child (particularly with respect to disabilities), and better investment in public schools and public safety.
In summary, the moral status of the fetus cannot be resolved by science, and it is not reasonable to expect consensus on the matter in a pluralistic society. Therefore, we should allow individuals to decide for themselves rather than allow some people to force their personal beliefs onto others, especially in a nation that was explicitly founded upon the separation between church and state.
Women are autonomous moral agents, and decisions about their health and their bodies should rest between them and their health care providers. Pregnancy may expose women to harm that can sometimes only be mitigated by termination. Restrictions on access to essential health care, including abortion, exacerbate already unjust disparities due to structural racism and social determinants of health. Ethical health policy should have the dual aims of ensuring patient autonomy and access to evidence-based standards of care, as well as improving health systems to reduce unintended pregnancies and reduce barriers to providing adequate care for children.
Footnotes
Acknowledgments
We want to thank Sarah Knopf and Kami Pulikandem for their help in creating the graphic.
Authors' Contributions
This work was conceptualized by SCH, who wrote the initial draft. All authors contributed to subsequent revisions to add important content and context.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.