
Abstract
Background:
The U.S. Public Health Service and the Institute of Medicine recommend that all women capable of becoming pregnant consume 400 μg of folic acid daily to help prevent neural tube defects (NTDs). Hispanic women are at higher risk of having babies with NTDs than non-Hispanic White women. This study assessed multivitamin (MV) use, a main source of folic acid, among Hispanic women of reproductive age using a survey of solely U.S. Hispanic adults.
Materials and Methods:
MV use was assessed as part of Porter Novelli's Estilos survey, fielded annually through the largest online U.S. Hispanic panel, Offerwise's QueOpinas. During the study period of 2013–2022, 9,999 surveys were completed; selection was weighted to match the U.S. Census American Community Survey proportions. Log-binomial regression models were applied to estimate MV use trends by age groups, acculturation levels, and pregnancy intention.
Results:
Among 3,700 Hispanic women of reproductive age, overall no MV use increased from 39.3% in 2013 to 54.7% in 2022 (p for trend <0.0001), especially among Hispanic women aged 18–34 years and those classified as acculturated. Among women planning to get pregnant, daily MV use was 31.1% in 2013 compared with 18.7% in 2020–2022 (p = 0.04).
Conclusions:
Given the increase in no MV use among Hispanic women of reproductive age, targeted interventions may help reach at-risk groups for NTDs prevention.
Introduction
Periconceptional use of folic acid has been shown to reduce the risk of neural tube defects (NTDs) in offspring. 1 –3 The U.S. Public Health Service and the Institute of Medicine recommend all women capable of becoming pregnant consume 400 μg of folic acid daily to prevent NTDs. 4,5 In 1998, mandatory fortification of enriched cereal grain products was fully implemented in the United States, which required 140 μg of folic acid for every 100 g of product. 6,7 In the years immediately following the mandatory fortification, the prevalence of NTDs declined and has subsequently remained at a lower prevalence. 8
Despite the overall decline in NTDs, Hispanic women consistently have higher rates of NTD-affected pregnancies compared with non-Hispanic White women and non-Hispanic Black women. 8 Hispanic women have lower concentrations of folate in their blood compared with non-Hispanic White women, 9 are more likely than non-Hispanic White and non-Hispanic Black women to have the MTHFR C677T gene variant, 8,10 and are less likely to know about the benefits of folic acid. 11 They have lower folic acid intake than women of other ethnic groups, and are less likely to consume fortified products, 12 –15 which may in part be owing to mandatory folic acid fortification not including corn masa flour, a staple food among many Hispanic Americans. In 2016, voluntary folic acid fortification of corn masa flour was authorized. 16,17 However, a recent study showed that pre- and postfortification red blood cell folate concentrations among Hispanic women of reproductive age did not differ, signifying remaining risk among Hispanic women for folate-sensitive NTDs. 18
In addition to fortified foods, folic acid can be found in dietary supplements. Most multivitamins (MVs) sold in the United States contain the recommended daily dose of folic acid for NTD prevention. In recent years, there has been a decrease in daily MV use among all women of reproductive age, and among Hispanic women specifically (from 30.6% in 2006 to 22.1% in 2016). 19,20 Hispanic women were also less likely to take supplements containing folic acid compared with non-Hispanic White women. 12,13,21 –26 When examining ethnic differences, acculturation, which is defined as the psychological, behavioral, and attitudinal change that takes place in the context of individuals of different cultures interacting continuously, can be an important factor. 27 Prior research has suggested that acculturation, indicated by language preference and time living in the United States, can influence folic acid intake, thereby affecting a person's folate status and NTD risk. 15,22 Previous studies found Mexican American women with fewer acculturation factors were less likely to report using a supplement containing folic acid than their more acculturated counterparts. 15,22,28
Given that the Hispanic population is one of the fastest growing populations in the United States 29 and that Hispanic women have the highest NTD prevalence, it is important to monitor MV use and identify specific characteristics of Hispanic women who are not taking MVs. This will help inform future efforts to increase MV use for NTD prevention within this population. Using a survey of solely Hispanic adults in the United States with an acculturation variable, we assessed MV use among Hispanic women of reproductive age.
Materials and Methods
Porter Novelli Public Service's Estilos survey is an annual web-based survey of U.S. Hispanic adults aged 18 years and older with questions on media preferences, health and nutrition choices, shopping habits, and political affiliation. It is administered through Offerwise's QueOpinas Panel, the largest online U.S. Hispanic panel with >220,000 active panelists who are recruited nationally through both English and Spanish network television. Quotas are used for age, language, acculturation level, region, gender, and heritage to prevent unbalanced results. Only participants with completed surveys are eligible to be included in the final dataset.
Acculturation levels were calculated by Offerwise based on four criteria: years living in the United States (0–4, 5–9, 10–14, 15–19, 20 years or more); language spoken at home (Spanish only, Spanish mostly, Spanish and English equally, English mostly, English only); cultural self-identification (Much closer to Hispanic/Latino culture, Somewhat closer to Hispanic/Latino culture, Equally close to both cultures, Somewhat closer to U.S. culture, Much closer to U.S. culture); and media habits (Spanish media only, Spanish media mostly, Equally Spanish and English media, English media mostly, English media only). Each criteria includes five response options, with five points being assigned to the unacculturated response options (0–4 years in the United States, only Spanish language spoken at home, etc.) and one point being assigned to acculturated response options (20 or more years in the United States, only English language spoken at home, etc.). All points from the four criteria were totaled to create an overall acculturation level (<9 points = acculturated; 9–15 = bicultural; 16–20 = unacculturated).
This analysis included data from the 2013 to 2022 surveys. The survey was fielded from September to November each year. Over the 10-year period, the surveys were sent to a sample of 30,094 panelists and 9,999 surveys were completed (∼1,000 annually). Response rates for each year varied between 27% and 40%, with an average of 34% over the 10-year period. The median time to completion varied between 18 and 42 minutes. Resulting data were weighted using gender, age, household income, household size, education, census region, country of origin, and acculturation. The weights were designed to match the prior year's U.S. Census American Community Survey (ACS) proportions for all variables except acculturation. Because acculturation is not measured in the ACS, acculturation weights were set to 25% unacculturated, 50% bicultural, and 25% acculturated to match the overall composition of the panel.
Every year from 2013 to 2022, the Estilos surveys asked about MV use, but the wording of the question and the response options changed in 2020. In the 2013–2019 surveys, the question assessing MV use asked respondents, “Please tell us approximately how often you usually take a multivitamin. Do you do it daily, weekly, monthly, less than once a month, or never?” In the 2020–2022 surveys, the question asked, “How many times a week do you take a multivitamin? If you do not take multivitamins, please type in ‘0’.” The response categories took into account the response options available across the 10-year study period. No MV use was defined as “never” from the 2013–2019 respondents and “0 times a week” from the 2020–2022 respondents. Daily MV use was defined as “daily” from the 2013–2019 respondents and six or more times a week from the 2020–2022 respondents.
Pregnancy intention was only asked in the 2013, 2020, 2021, and 2022 surveys, but differed in wording and response options between 2013 and 2020–2022. In the 2013 survey, the question assessing pregnancy intention asked, “From today, how soon do you plan to have a child?” with response options: I don't want to have any/any more, within the next year, 1–2, 3–5, more than 5 years, N/A: hysterectomy/menopause, and N/A: I am currently pregnant. In the 2020–2022 surveys, the question asked, “Which one of the following best describes your pregnancy planning status?” with response options: my partner and I are currently pregnant, my partner and I are planning to get pregnant in the next year or so, my partner and I do not plan to get pregnant at any time in the next year or so but plan at some time in the future, my partner and I do not plan to get pregnant at any time in the near future, we cannot get pregnant/have a child—that is, women (postmenopausal, tubal ligation, hysterectomy), men (vasectomy), and none of these/do not have a partner.
Analysis of pregnancy intention was coded as either planning to get pregnant or not planning to get pregnant. Those who could not get pregnant or were currently pregnant were excluded owing to small sample size.
We restricted the analysis to female respondents aged 18–44 years, then calculated the unweighted counts and weighted percentages of the demographic variables by survey year. We calculated the prevalence of MV use by year for age groups, acculturation levels, and pregnancy intention. When examining acculturation, we also looked at Mexican women and non-Mexican women separately. We used a log-binomial model to estimate the crude trend in no and daily MV use between 2013 and 2022. All models were weighted to account for the survey design. We estimated the trend in no and daily MV use by age groups and acculturation levels. All analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
There were 3,700 Hispanic women of reproductive age (18–44 years) with completed surveys over the 10-year period. Overall, 73.4% of women were aged 25–44 years, 52.5% were married, 73.7% were Mexican, 56.9% had spent 15 or more years in the United States, and 40.9% resided in the West region (Table 1). Among the women who indicated pregnancy intention (n = 1,354, survey years 2013, 2020–2022), 35.0% were planning to get pregnant and 50.2% were not planning to get pregnant.
Respondent Demographics Among U.S. Hispanic Women of Reproductive Age, Porter Novelli Estilos Survey, 2013–2022
Employment status was missing for approximately 48% of respondents in 2016.
Pregnancy intention was only collected in 2013, 2020, 2021, and 2022.
Overall, no MV use increased from 39.3% in 2013 to 54.7% in 2022, with a significant trend over the 10-year period (p for trend <0.0001; Fig. 1). Daily MV use decreased from 26.7% in 2013 to 17.6% in 2022, with a significant trend (p for trend <0.0001). From 2013 to 2019, weekly MV use increased from 12.9% to 17.6%. Approximately 7% reported consumption of 4–5 MVs/week in 2020, 22% reported in 2021, and 11% reported in 2022 (Supplementary Fig. S1).
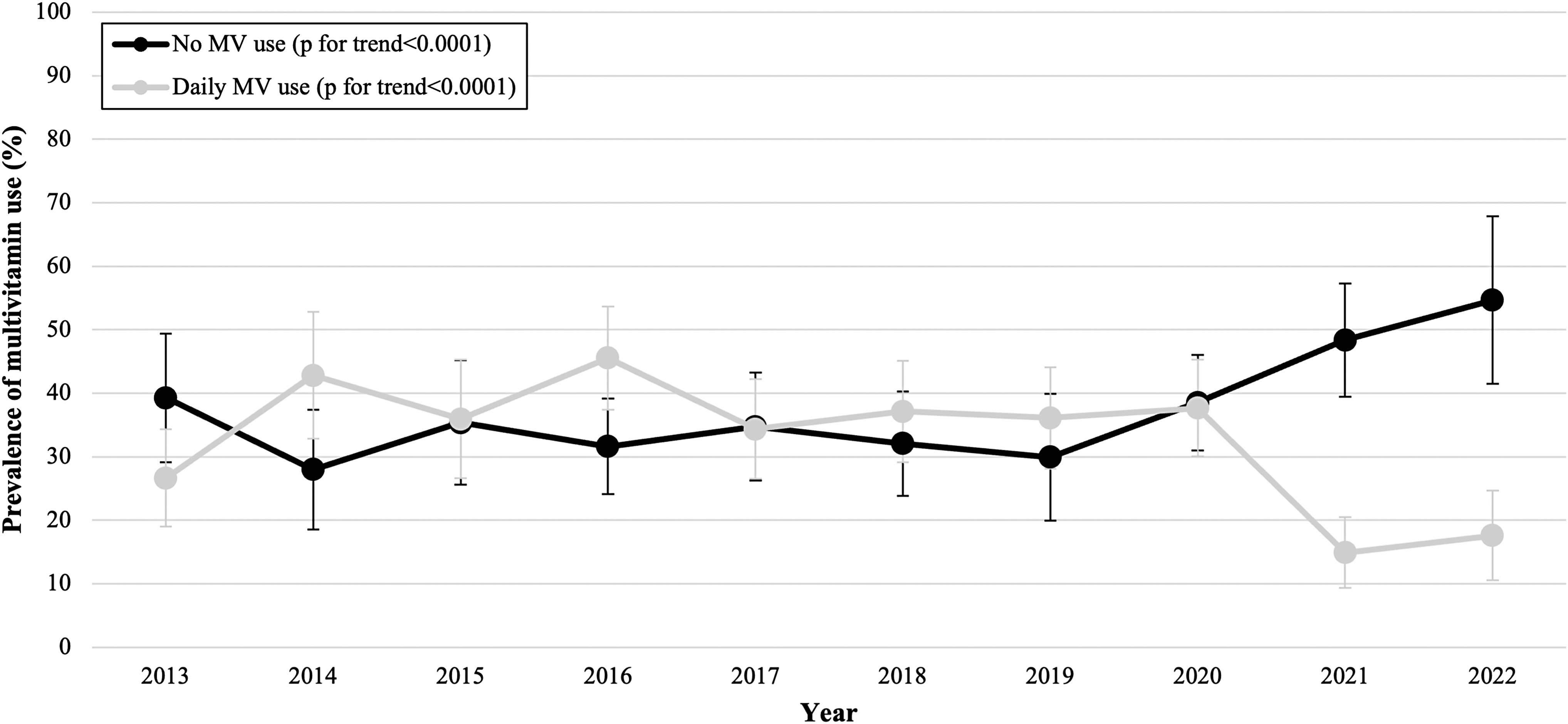
MV use among U.S. Hispanic women of reproductive age, Porter Novelli Estilos Survey, 2013–2022. MV, multivitamin.
MV use by age groups
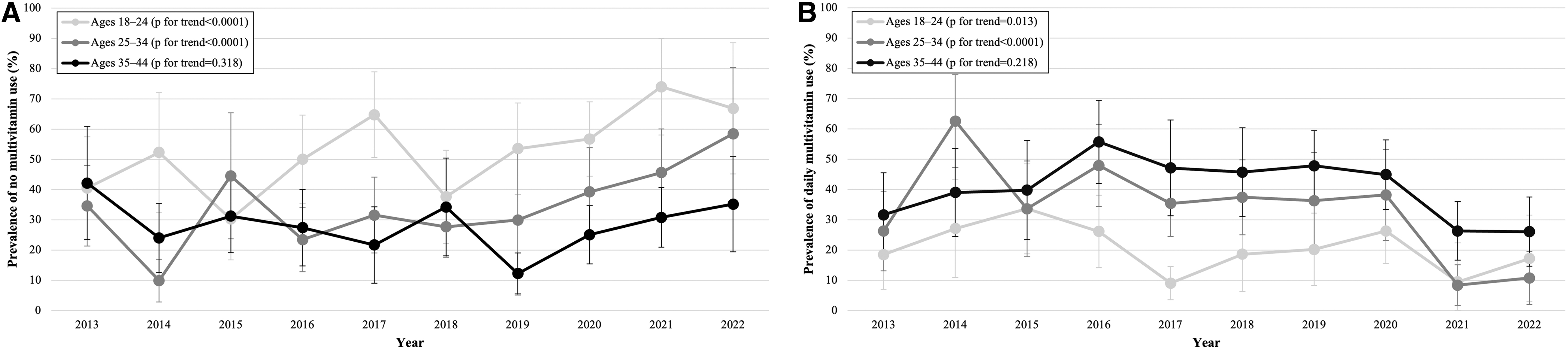
The overall prevalence of daily MV use was highest among women aged 35–44 years (40.9%; 95% confidence interval [CI], 36.5%–45.4%; data not shown), followed by women aged 25–34 years (33.8%; 95% CI, 29.1%–38.5%), and lowest among women aged 18–24 years (21.2%; 95% CI: 16.8%–25.6%). There were differences in MV use trends by age group. Among women aged 18–24 and 25–34 years, the prevalence of no MV use increased from 40.6% in 2013 to 66.9% in 2022, and from 34.7% in 2013 to 58.5% in 2022, respectively. The trends for both age groups were significant (p for trend <0.0001 for women aged 18–24 years and p < 0.0001 for women aged 25–34 years; Fig. 2A). Among women aged 35–44 years, the prevalence of no MV use decreased from 42.2% in 2013 to 35.2% in 2022, but the trend was not significant (p for trend = 0.318). The prevalence of daily MV use decreased among all women, although the trends were only significant for women aged 18–34 years (Fig. 2B). In women aged 18–24 years, the prevalence decreased from 18.5% in 2013 to 17.2% in 2022 (p for trend = 0.013). In women aged 25–34 years, the prevalence decreased from 26.3% in 2013 to 10.8% in 2022 (p for trend <0.0001). In women aged 35–44 years, the prevalence decreased from 31.6% in 2013 to 26.1% in 2022, although the trend was not significant (p for trend = 0.218).
Trends in
MV use by acculturation levels
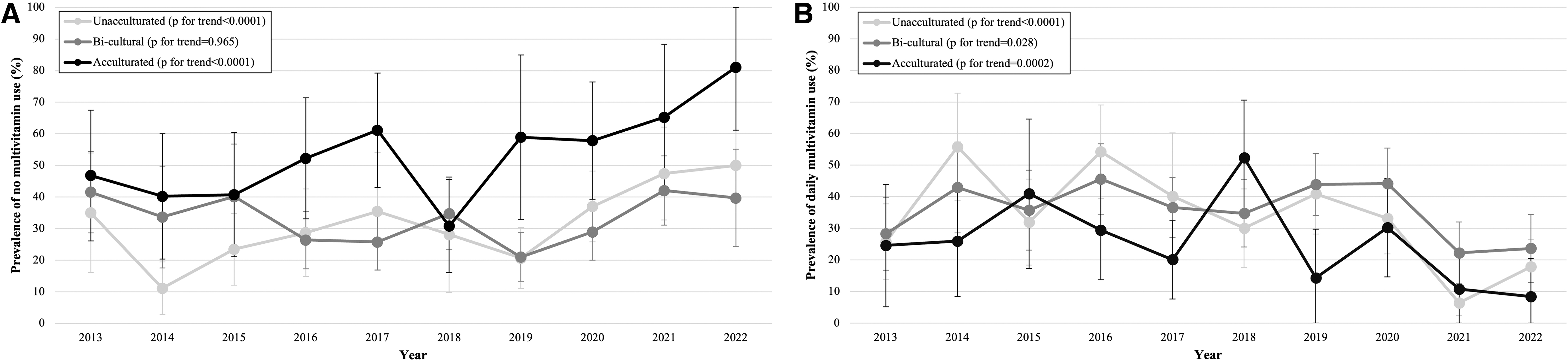
Differences were observed in MV use by acculturation status. The prevalence of no MV use increased from 35.0% in 2013 to 50.0% in 2022 among unacculturated women (Fig. 3A), and from 46.8% in 2013 to 81.1% in 2022 among acculturated women. Both unacculturated and acculturated women experienced significant trends in no MV use (p for trend <0.0001 and p for trend <0.0001, respectively). Among bicultural women, the prevalence of no MV use remained relatively unchanged from 41.5% in 2013 to 39.7% in 2022 (p for trend = 0.965). The trends of daily MV use decreased among all acculturation levels, with significant trends (unacculturated, p for trend <0.0001; bicultural, p for trend = 0.028; acculturated, p for trend = 0.0002; Fig. 3B). When assessing the women by country of origin (Mexican vs. non-Mexican women), we found that both acculturated Mexican and acculturated non-Mexican women had the lowest overall daily MV use compared with their unacculturated and bicultural counterparts (data not shown).
Trends in
MV use by pregnancy intention
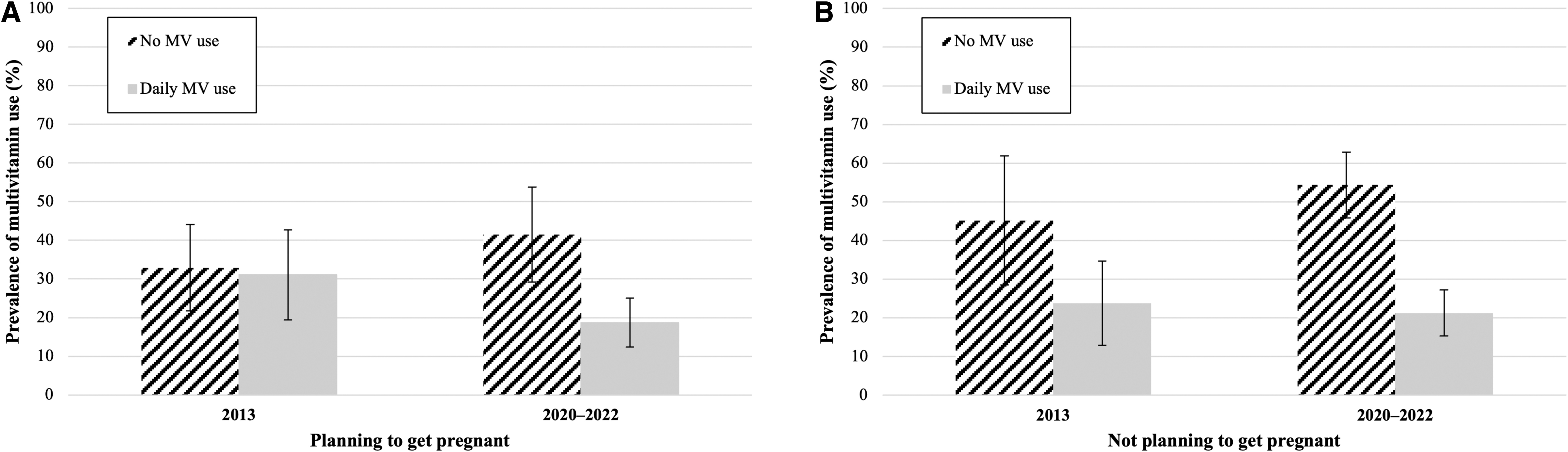
We also examined MV use by pregnancy intention. Among Hispanic women planning to get pregnant, 31.1% (95% CI, 19.4%–42.7%) reported daily MV use in 2013, whereas 18.7% (95% CI, 12.4%–25.0%) reported daily MV use in 2020–2022 (p = 0.04; Fig. 4A). Among Hispanic women not planning to get pregnant, 23.8% (95% CI, 12.9%–34.7%) reported daily use in 2013, whereas 21.3% (95% CI, 15.4%–27.2%) reported daily use in 2020–2022 (p = 0.39; Fig. 4B).
MV use by survey year among U.S. Hispanic women of reproductive age
Discussion
In our study of exclusively Hispanic women of reproductive age in the United States, no MV use increased from 39% in 2013 to 55% in 2022 with a significant trend. Although our study presents more recent data, the finding is consistent with an earlier study examining MV use among women of reproductive age in the United States that reported an increase in no MV use among Hispanic women from 40% in 2006 to 59% in 2016. 19 In addition, we observed a decrease in daily MV use from 27% in 2013 to 18% in 2022. In a study that defined daily MV use as seven or more MVs consumed per week, the prevalence of daily MV use decreased from 31% in 2006 to 22% in 2016 among Hispanic women. 19
This study observed that young women aged 18–24 years had the lowest overall prevalence of daily MV use (21.2%). The low prevalence in women aged 18–24 years may be in part owing to younger women having the lowest awareness regarding folic acid consumption. 30,31 In addition to low daily MV use, the prevalence of no MV use among the young Hispanic women increased over the 10-year study period. Given that the mean age at first birth for Hispanic women is ∼25 years, 32 it may help to tailor messaging on folic acid recommendations to younger women to promote the use of supplements containing folic acid. In contrast, women aged 35–44 years had the highest daily MV use over the 10-year study period. Previous research has shown that older women are more likely to take an MV or supplement compared with younger women, 23,33 –35 and this may be a result of older individuals being more likely to talk to a health care provider about taking vitamins, for any purpose. 36
A significant increase in no MV use was observed for both unacculturated and acculturated women, whereas a significant decrease in daily MV use was observed across all acculturation levels. Furthermore, acculturated women (both Mexican and non-Mexican) had the lowest overall prevalence of daily MV use compared with both unacculturated and bicultural women, which differs from previous studies that found Mexican American women with fewer acculturation factors were less likely to report using a supplement containing folic acid than their more acculturated counterparts. 15,22,28
Pregnancy intention among Hispanic women in our study did not appear to affect daily MV intake. Although the prevalence of daily MV use was higher for women planning to get pregnant than those not planning to get pregnant in 2013 (31% vs. 24%), more recent years showed similar prevalence of daily use between both groups (19% vs. 21%). Although our study's finding on daily MV use among women planning to get pregnant is inconsistent with a previous study that examined daily MV use among all women of reproductive age including those intending pregnancy in the next 12 months, 37 our study only includes Hispanic women, who are known to have lower MV use. Also, it is unclear how the COVID-19 pandemic might have impacted daily MV habits.
Given that almost half of pregnancies are unintended, 38 it is important to ensure that women who are contemplating a pregnancy understand the importance of taking 400 μg of folic acid daily for NTD prevention. Examining MV use by pregnancy intention can give some insight into preconception care, as evidence has shown that women who had discussions with a health care provider about taking vitamins with folic acid before pregnancy were more likely to take vitamins in the month before pregnancy compared with women who did not have discussions. 39
MVs are one of the main sources of folic acid to ensure that at-risk populations, such as Hispanic women of reproductive age, reach the folate concentration needed for NTD prevention, especially because women who consume only fortified food might not reach 400 μg of folic acid daily. 40 Our findings show a significant increase in no MV use among Hispanic women over the 10-year study period, although continued monitoring would provide insight into the impact of the COVID-19 pandemic on MV use.
Targeted outreach may help to increase knowledge and utilization of MVs. In an intervention (either received advice to take MVs or provided MVs) targeted at mothers attending well-child visits of children aged 0–24 months, these mothers were more likely to report taking an MV at the subsequent well-child visit compared with mothers who received no intervention. 41 Another strategy that has successfully been used for outreach to Hispanic populations is the Promotora de Salud model. The Promotora de Salud model utilizes community outreach and provides the community member with a direct connection to a community health worker for questions and follow-up. 42 Significant changes in awareness and knowledge of folic acid as well as MV consumption have resulted from this model. 11,43 Understanding the drivers for successful outreach implementation is key to reaching Hispanic women of reproductive age, especially young Hispanic women, to better target MV use and NTD prevention messages.
This study had several strengths. The Estilos survey was solely administered to Hispanic adults, with the option to respond in either English or Spanish, which allowed for a closer look at a population that is at higher risk of NTD-affected pregnancies. It is also a national survey with multiple years of data, allowing for examination of changes over time. In addition, this study included two characteristics, acculturation levels and pregnancy intention, which have been shown to affect MV use for NTD prevention among Hispanic people.
There are several limitations to this study. First, the change in the response option for the MV question in 2020 could have affected the change in daily MV use over the 10-year period. However, we performed a sensitivity analysis on the 2020–2022 data that showed a clear cut-point for daily MV use. Second, MV use serves as a proxy for folic acid consumption. The survey question does not ask if the MV contains folic acid or if other types of supplements containing folic acid were consumed, and therefore may result in an inaccurate assumption of folic acid intake for NTD prevention. Third, the survey had the potential for selection bias and information bias because it was conducted online using a quota sampling panel with self-reported results on frequency of MV use. The selection bias owing to the nature of survey participation and only including surveys that are complete could limit the generalizability of these findings. Fourth, we were unable to stratify the non-Mexican group because of the small size of the different Latino subgroups and were, therefore, unable to examine any potential variability by country of origin. Finally, we restricted our analysis to respondents who reported “female” as their gender. Although this may not be inclusive and representative of all people capable of becoming pregnant, misclassification is expected to be low.
Conclusion
No MV use increased among U.S. Hispanic women of reproductive age, especially young Hispanic women, between 2013 and 2022. Targeted interventions to promote MV use, especially daily intake, might be beneficial to prevent NTDs among Hispanic women.
Footnotes
Acknowledgment
This project was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and CDC.
Authors' Contributions
K.L. led the analyses and wrote the initial draft of the article. C.T.M. and L.F.Y. initiated the project. X.Y. provided replications for all analyses. All authors provided substantive contributions to the development of the article and provided final approval of revisions.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy (e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.