
Abstract
Background:
Owing to its high sensitivity, as concluded in the Breast UltraSound Trial (BUST), targeted ultrasound (US) now seems a promising accurate stand-alone modality for diagnostic evaluation of breast complaints. This approach implies omission of bilateral digital breast tomosynthesis (DBT) in women with clearly benign US findings. Within BUST, radiologists started with US followed by DBT. This side-study investigates women's experiences with DBT, their main motivation to undergo diagnostic imaging, and their view on US as a stand-alone modality.
Methods:
A subset of BUST participants completed a questionnaire on their DBT experiences, reason for undergoing diagnostic assessment, and view on US-only diagnostics. Responses were analyzed with descriptive statistics and logistic regression analyses.
Results:
In total, 778 of 838 women (response rate 92.8%) were included (M = 47, SD = 11.16). Of them, 16.8% reported no burden of DBT, 33.5% slight burden, 31.0% moderate, and 12.7% severe burden. Furthermore, 13% reported no pain, 35.3% slight pain, 33.2% moderate, and 11.3% severe pain. Moreover, 88.3% indicated that the most important reason for breast assessment was explanation of their complaint and to rule out breast cancer, whereas 3.2% wanted to “check” both breasts. And 82.4% reported satisfaction with US only in case of a nonmalignancy.
Conclusions:
Our study shows that most women in the diagnostic setting experience at least slight-to-moderate DBT-related burden and pain, and that explanation for their symptoms is their main interest. Also, the majority report satisfaction with US only in case of nonmalignant findings. However, exploration of women's perspectives outside this study is needed as our participants all underwent both examinations.
Introduction
Worldwide, many women are referred to the hospital with breast complaints, mostly palpable lumps. In ∼7%–15% of the cases, these lumps are breast cancer. 1 –4 Diagnostic evaluation currently involves bilateral digital breast tomosynthesis (DBT) (or previously mammography [MG]), followed by targeted ultrasound (US) of the complaint. In Europe, only young women (under 30 or 40 years depending on national guidelines), and pregnant or lactating women are primarily evaluated with US. 5,6 However, recent studies show that US has a much higher sensitivity than (at the time) MG, especially in younger women. 7 –9 According to these studies, US is a suitable stand-alone modality for women <40 or 45 years old, with a low added value of adjunct MG. 10
The value of targeted US for diagnostic assessment in older women, however, has not yet been evaluated, whereas also in these women the symptomatic area is always evaluated with US. Therefore, the Breast UltraSound Trial (BUST) investigated the diagnostic accuracy of US as stand-alone modality. Results show that US has a very high sensitivity and specificity (98.5% and 90.7%, respectively) and that the added value of DBT is very low (0.2%) in the evaluation of focal breast complaints (although there are some cases [0.4%] with malignant additional findings). 11 Therefore, it is evident that there is merit in the consideration of US as a first line modality in the clinical setting. More detailed information is provided in the original article on the trial. 11
Given the limited clinical impact, questions rise on women's attitude toward omitting DBT where appropriate. First, it is important to analyze women's experiences with diagnostic DBT, as the examination can be considered painful and uncomfortable due to the applied breast compression. Previous studies, however, mostly focused on asymptomatic women undergoing screening MG. 12 –15 One study that did include symptomatic women shows that 23% and 49% of participants report pain at a cutoff level of 60 and 40, respectively, on the visual analog scale.
In addition, 34% reported discomfort or pain on the Pain/Discomfort Rating Scale (DRS), a measure with six answers options ranging from very comfortable to painful/very painful. 16 Another study including a symptomatic population reported that 66.5% of women experienced pain, varying from mild to severe on a 4-point scale (1 = no pain, 4 = strong/intense pain). 17 However, no studies focused on DBT. This is important, as DBT compression time is longer, and could potentially impact pain experiences. 18 Since negative experiences with DBT might cause a delay in the timely detection of relevant findings due to women postponing future examinations, DBT-related pain experiences in the diagnostic setting should be explored.
Second, the BUST approach involves initial targeted US, which implies a localized complaint-specific evaluation without, in case of benign US outcomes, bilateral breast evaluation with DBT. There is currently a lack of knowledge about the value that women place upon additional imaging of the whole breast and both breasts when they present with only a local symptom. The question rises how important this bilateral “breast check” is in women presenting with symptoms undergoing diagnostic investigations.
Lastly, it is highly relevant to explore women's satisfaction with US as a stand-alone imaging modality when omitting DBT from the diagnostic pathway. This study thus focusses on women's clinical DBT-related pain experiences, their motivation for undergoing diagnostic assessment, and their opinion on performance of US only in case of no malignancies. Moreover, we aimed to identify potential external factors (e.g., the hospital or getting biopsy) or personal characteristics of women (e.g., complaint type or age) that are associated with these outcomes.
Materials and Methods
Design
This survey study was performed as a side study to the prospective BUST. The regional ethical committee (CMO Arnhem-Nijmegen) waived ethical approval for the BUST and this side study (2016-3034). This study conformed to the principles of the Helsinki Declaration. All participants provided written informed consent.
Subjects
The study base consisted of 838 Dutch women who visited the radiology department of three different Dutch hospitals: Radboudumc Nijmegen (RUMC), NWZ Alkmaar (NWZ), and St. Antonius Hospital Utrecht (ANT). All women presented with focal breast complaints and were >30 years, because DBT is recommended for women from this age onward according to the Dutch guidelines. This survey study started when BUST was already running for >8 months, so radiologists and radiographers were familiar with and used to the study procedures.
Participants were excluded when they were men, gene mutation carriers, referred from the breast screening program, and/or when having a relevant history of breast cancer or surgery. Women were further excluded when they only underwent US during their visit (for various reasons).
Procedure
Each woman participated in the BUST, in which the regular order of evaluation of breast imaging was reversed so that the targeted US was assessed before the DBT images. However, the exact procedure differed between the hospitals. During the course of this survey, at RUMC and ANT, the US was performed before DBT. However, at NWZ, only the order of the imaging evaluation by the radiologist was reversed while the order of the examinations for the participants remained unchanged (DBT was performed before US, but not released for radiological evaluation until after US was performed).
After imaging, mostly during their wait for the DBT results, participants filled out a short one-page questionnaire on paper. Upon participation, all women were assigned a study number so that all data could only be traced back to their unique number. The document linking the participants' data with their study number was archived.
Measures
The questionnaire had three sections (Supplementary File A). In the first section personal factors were addressed. Participants were asked about the nature of their complaint. They could choose from several options and select multiple answers (Table 1). Furthermore, participants were asked about their cup size (AA to G) and whether they are currently participating in the national breast cancer screening program (yes vs. no).
Participant Characteristics
ANT, St. Antonius Hospital Utrecht; NWZ, NWZ Alkmaar; RUMC, Radboudumc Nijmegen.
In the second section, DBT-related burden (causing worry or distress) and pain were evaluated. They could report the burden they experienced during DBT on a 4-point scale: (1) no burden, (2) slight burden, (3) moderate burden, and (4) severe burden. The same 4-point scale was used for pain.
In the third section, the acceptability of an US-only approach (in case of nonmalignant findings) was explored. Women were asked about their motivation for visiting the radiology department (explanation of the complaint to rule out breast cancer immediately vs. checking both breasts) and whether they would already feel enough comforted when US showed the complaint to be explained by normal breast tissue or a benign abnormality (yes vs. no).
Statistical analysis
Descriptive statistics were calculated for pain and burden and for the questions on women's reasons for undergoing breast assessment and acceptability of an US-only approach, taking into account the missing values. To evaluate potential effects of complaint type (lump/other complaint), cup size (AA to C/D to G), age category (<50/>50), getting biopsy (yes/no), reason for visiting (explanation complaint/checking breasts), screening program participation (yes/no), or the hospital (RUMC/ANT/NWZ) on the outcomes variables, ordinal logistic regression analyses were done for the effect on burden and pain and binary logistic regression analyses for the effect on reason for visiting and US satisfaction. All tests were performed in IBM SPSS Statistics version 25. Outcomes are reported as chi square values with the corresponding degrees of freedom. A p-value ≤0.05 was considered significant.
Results
Subjects
A total of 778 of 838 invited women completed the questionnaire (response rate 92.8%) (Supplementary File B). They ranged in age from 30 to 88 years old (M = 47, SD = 11.16). In the vast majority of women, the complaint consisted of a palpable lump (82.8%). A total of 145 women underwent biopsy of the complaint after US. Characteristics of the participants are given in Table 1.
DBT-related burden and pain
In total, 732 of 778 participants answered the question regarding burden of DBT. A total of 16.8% of the respondents reported no burden at all, 33.5% experienced slight burden, 31.0% moderate, and 12.7% severe burden. As for pain, 722 participants responded. Thirteen percent reported no pain, whereas the rest of the participants did, varying from slight (35.3%) to moderate (33.2%) to severe pain (11.3%).
Ordinal logistic regression analyses were performed to explore the effects of complaint type, cup size, age, biopsy, reason for visiting, screening participation, and hospital on the likelihood that participants reported DBT-related pain or burden. Both analyses provided no significant improvement in fit of the final model over the null model [respectively χ 2 (8) = 6.825, p = 0.556 and χ 2 (8) = 5.147, p = 0.742].
Reason for visiting
A total of 712 women reported their reason for undergoing diagnostic breast assessment. The great majority of 687 women indicated that explaining their complaint was their main motive (88.3%), whereas 25 women preferred evaluation of both breasts (3.2%). Of these women, 21 were ≤50 years old. Binary logistic regression shows no higher likelihood of women choosing either one of the options based on the following predictors: complaint type, cup size, age, biopsy, screening participation, or hospital [χ 2 (7) = 5.888, p = 0.553].
US diagnostics only
Out of all participants, 641 (82.4%) reported that they would be comforted with US diagnostics alone in case of a nonmalignancy, whereas 79 would not (10.2%). Binary logistic regression was performed to ascertain the effects of complaint, cup size, age, biopsy, reason for visiting, screening participation, and hospital on the likelihood that participants would be comforted after US diagnostics only. The logistic regression model provided a significant fit over the null model [χ 2 (8) = 16.110, p = 0.041]. Going to NWZ was associated with a somewhat greater likelihood of being comforted after US diagnostics only compared with visiting the other two hospitals (B = 1.066, p = 0.002) (Fig. 1).
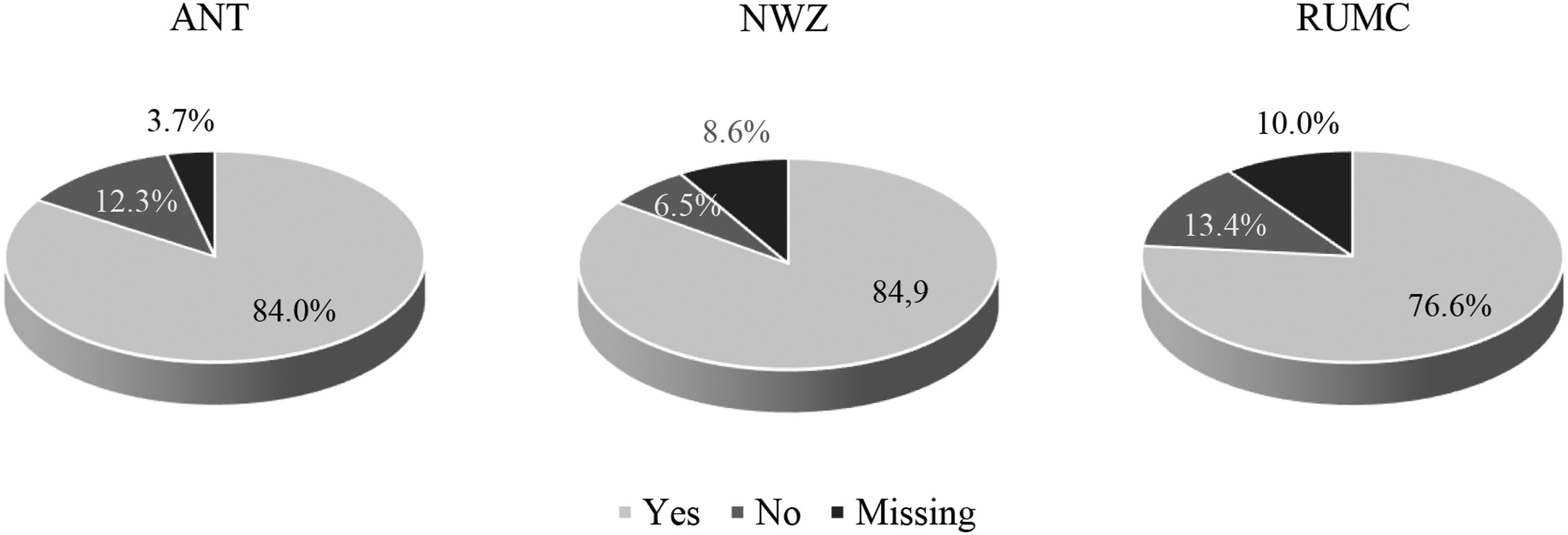
Percentage of participants being comforted after US diagnostics per hospital (ANT, n = 235, 9 missing; NWZ, n = 297, 28 missing; RUMC, n = 188, 21 missing). ANT, St. Antonius Hospital Utrecht; NWZ, NWZ Alkmaar; RUMC, Radboudumc Nijmegen; US, ultrasound.
Discussion
In this study, we surveyed a large group of women presenting with focal breast complaints on their experience with DBT, their reason for undergoing assessment at the hospital, and their views on US as a primary imaging modality. The results show that virtually all women particularly undergo diagnostic imaging to clarify the nature of their complaint and >80% of the women indicate to be comforted after US-based diagnostics in case of nonmalignant findings.
This is important as we also found that almost all women perceive DBT as at least slightly burdensome and the vast majority also report some degree of pain. For both outcomes, >10% of women rate the impact as severe. This implies that DBT performance should be carefully considered, provided that focal complaints can be well explained by US alone and hardly any carcinomas are missed.
The observation that most women perceive DBT as at least slightly burdensome and painful confirms results from previous studies with MG. 12 –15 However, we found relatively higher reported levels of discomfort and pain than other studies. Nonetheless, the results are very homogeneous over the different hospitals, whereas different professionals and DBT machines from different vendors were involved. One explanation for the discrepancy with other studies is that compression with DBT is somewhat longer than with regular MG, which may have increased pain scores. 19 A study by Hafslund 17 indeed shows that, compared with our study in which DBT was the standard, MG-related pain in symptomatic women tends to be absent more often (33.5% vs. 13%) and less frequently moderate to severe (31.8% vs. 44.5%).
Another explanation could be the wide variance in pain scales. Several studies show that less pain and burden is reported when there are less answer options. For instance, the Pain/Discomfort Rating Scale (PDRS) combines pain and discomfort in one scale, meaning fewer options to express pain experiences. This results in less pain report compared with other measures, with, for example, pain report in ∼2%–8.5% of women when using the PDRS versus pain report in 78%–92% of women with scales including more options. 14,18,20
Comparable scales were used by Aro et al., 13 who measured women's pain and burden due to MG separately. Despite this similar scale use, incidence of moderate and severe pain was higher in our study. This is likely explained by the fact that our study included a clinical population, whereas Aro et al. included only asymptomatic women coming for a screening examination. Although our population was investigated with DBT, research has shown that regular MG tends to be more painful for women undergoing a diagnostic examination than women attending screening MG. 21
Moreover, existing complaints such as breast lumps and breast pain, inflammatory conditions, and fibrocystic disease can be risk factors for pain experiences and strong discomfort. 16,22 Symptomatic women may also experience more fear that could result in higher reported pain levels, as anxiety is proven to be a risk factor for increased pain experiences. 23,24
We evaluated various factors that we presumed may affect participants' survey outcomes. However, no major effects of any of these factors on women's burden/pain or motives for undergoing breast assessment were found. For example, there was no effect of cup size on DBT-related pain. This finding is supported by several other studies that show no link between breast size and pain experience during DBT, with only one study showing that women with very large breasts (cup DD) and very small breasts (cup AA) are more at risk of experiencing severe pain during DBT. 12,15,25,26 The same studies show, similar to our study, no effect of age on DBT pain or discomfort.
We also expected that undergoing biopsy during US would result in greater pain during DBT, since a high fear of breast cancer is often associated with greater pain experiences. 23,24 Biopsy was only done in women with suspect lesions, presumably leaving them more anxious than women with clearly benign findings. Moreover, breast biopsy itself can sometimes cause pain in women, 27 which might increase when performing DBT right thereafter. Potentially, it could also be hypothesized that women who got biopsy experience less pain during DBT due to the administration of a local anesthetic. However, logistic regression analysis did not show any effect.
We hypothesized that a whole-breast evaluation with DBT might sometimes be valued by women when undergoing diagnostic breast imaging for a focal complaint, especially when they are not yet eligible for the national screening program (i.e., younger than 50 years). After all, this means they are not subjected to a biennial breast control. Also in women who are eligible for screening, the time period since their last mammogram and the imaging results might influence their perceived burden and desire for DBT at the hospital, although we did not evaluate this in this study. Although indeed a number of women reported that evaluation of both breasts was their most important motivation, this percentage was small (3.2%).
The majority of those women (21 out of 25) were, however, indeed younger than 50 years. Still, bilateral breast control does not seem to be a common consideration in symptomatic women, although it is also plausible that a social desirability bias has minimized the reporting. In addition, the small number might be attributed to the type of complaints women presented with, such as lumps or other focal symptoms. Perhaps the desire for a “breast check” is less evident in women with targeted complaints relative to women with more vague complaints such as mastopathy. The latter is, however, not the BUST's target population and was, therefore, not investigated.
We asked women whether they would feel enough comforted after US when it showed nonmalignant results. Importantly, this is not about US actually being sufficient in terms of clinical performance, but more about whether women feel that US provides a satisfying explanation for their complaint. Also, although the differences were small, we did find that women at NWZ were somewhat more often comforted after US only compared with women at RUMC and ANT.
This is likely explained by the differences in exact study procedure, as at RUMC and ANT, US was actually performed before DBT. Possibly, women were aware of the order adjustment in these hospitals. This might have somewhat increased their anxiety, as reassuring remarks from radiographers that “nothing will change,” which could have been the case at NWZ, might have a different effect on women than remarks such as “we will do something different.” The latter could raise more concern, which could have happened at RUMC and ANT.
There are some important limitations to this study. First, participants completed the survey after US and DBT were performed, but mostly during their wait for the DBT outcomes, mimicking a setting in which participants only know their US outcomes. Although this could be considered the most realistic situation as an US-only approach would imply no performance of DBT and thus no knowledge of any DBT outcomes, it can be argued that reliability of the survey outcomes could be obscured by women's levels of anxiety when undertaking the survey directly after imaging.
In contrast, however, knowing there would be no consequences for them as they all underwent DBT anyway, regardless of the outcome of US, could have affected the extent to which women reported acceptability of US. In addition, it is likely that women's feeling of being reassured after US when no malignancy was detected is highly correlated with trust in their physician; when the performing radiologist believes and communicates to women that US is sufficient, this is likely reflected in their answers on the survey question.
It is, therefore, relevant to investigate women's satisfaction in a cohort that is indeed evaluated with US only, and outside of the direct imaging procedure. Lastly, this study was performed in women who underwent DBT. The results can, therefore, not be generalized to countries in which 2D MG is still the standard.
Conclusions
This study shows that DBT is perceived as burdensome and painful in many women. In symptomatic women, pre-existing fear and sore breasts might contribute to even greater burden and pain. Consequently, provided that US is an accurate diagnostic imaging tool, this population in particular could benefit from skipping DBT when initial US findings are nonmalignant. Our results suggest that the majority of women only want an explanation for their breast symptoms and that most women, at least in the BUST population, believe that US could provide a satisfying explanation for their complaint. However, given the limited options to elucidate on their attitude and the fact that our participants all underwent both examinations, exploration of women's perspectives outside this study is needed.
Footnotes
Acknowledgments
We thank all breast radiographers and radiologists who helped in the data collection and women who participated in the study.
Authors' Contributions
C.C.N.S. contributed to data curation, formal analysis, investigation, project administration, resources, and writing—original draft preparation. L.A. was involved in conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, supervision, and writing—review and editing. P.T.M.A. and S.G. carried out data curation, investigation, project administration, resources, and supervision. M.C.J.v.O. took charge of conceptualization and funding acquisition. M.J.M.B. carried out conceptualization, methodology, and writing—review and editing. R.M.M. was in charge of conceptualization, funding acquisition, investigation, methodology, supervision, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by ZonMw [Grant No. 843002823]. The funder had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Supplementary Material
Supplementary File A
Supplementary File B
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.