
Abstract
Objective:
Our objective was to evaluate the feasibility of a new protocol for telemedicine follow-up after medication management of early pregnancy loss.
Study Design:
The study was designed to assess the feasibility of planned telemedicine follow-up after medication management of early pregnancy loss. We compared these follow-up rates with those after planned in-person follow-up of medication management of early pregnancy loss and planned telemedicine follow-up after medication abortion. We conducted a retrospective cohort study, including patients initiating medication management of early pregnancy loss <13w0d gestation and medication abortion ≤10w0d with a combination of mifepristone and misoprostol between April 1, 2020, and March 28, 2021. As part of a new clinical protocol, patients could opt for telemedicine follow-up one week after treatment and a home urine pregnancy test 4 weeks after treatment. Our primary outcome was completed follow-up as per clinical protocol. We also examined outcomes related to complications across telemedicine and in-person follow-up groups.
Results:
Of patients reviewed, 181 were eligible for inclusion; 75 had medication management of early pregnancy loss, and 106 had medication abortion. Thirty-six out of 75 patients elected for telemedicine follow-up after early pregnancy loss. Of patients scheduled for telemedicine follow-up, 29/36 (81%, 95% CI: 64–92) with early pregnancy loss and 64/69 (93%, 95% CI: 84–98) undergoing medication abortion completed follow-up as per protocol (p = 0.06). Completed follow-up was also similar among patients undergoing medication management of early pregnancy loss who planned for in-person follow-up (p = 0.135). Complications were rare and did not differ across early pregnancy loss and medication abortion groups.
Conclusions:
Telemedicine follow-up is a feasible alternative to in-person assessment after medication management of early pregnancy loss.
Implications
During the COVID-19 pandemic, telemedicine services expanded for medication management of early pregnancy loss and medication abortion. These changes have the potential to improve care by removing barriers to follow-up ultrasounds and in-person visits. This study indicates that telemedicine follow-up is a safe and feasible alternative after medication management of early pregnancy loss.
Introduction
Early pregnancy loss is the most common complication of pregnancy affecting 15–20% of all clinically recognized pregnancies. 1 –4 In managing early pregnancy loss, most patients prefer an active approach with either uterine aspiration or medication with mifepristone and misoprostol to expedite completion of their loss. 5 –8 In contrast to uterine aspiration, approximately 10% of patients undergoing medication management may require additional intervention with uterine aspiration or repeat misoprostol dosing to achieve successful pregnancy expulsion. 5,9 Because of this possibility, medication management is traditionally followed by an in-person visit with a pelvic ultrasound 1–2 weeks after treatment to ensure the successful completion of the pregnancy and evaluate for the need for additional intervention. 5,10
Medication abortion, which utilizes the same medication regimen of mifepristone and misoprostol, has well-established remote treatment and follow-up options. 11 These options include entirely remote consultation, medication provision, and follow-up methods. 12 With regard to follow-up, telemedicine assessment in combination with a home urine pregnancy test has been proven to be a safe and practical alternative to in-person follow-up. 13 –16 Telemedicine assessment has also been shown to be preferable to in-person follow-up for medication abortion without compromising safety or success rates. 17,18 Similarly, serial serum human chorionic gonadotropin trends can be utilized in lieu of in-person follow-up after medication abortion as another method of remote follow-up. 18 Despite the treatment parallels in the medication management of early pregnancy loss and medication abortion, remote follow-up has not been established within the context of early pregnancy loss. 19
During the COVID-19 pandemic, telemedicine proved to be an instrumental part of health care delivery. More specifically, telemedicine represents an important innovation within obstetrics and gynecology that has been shown to improve outcomes and reduce disparities in care, especially across socioeconomic, geographic, and racial divides. 20 –22 These outcomes have been demonstrated in multiple settings, including prenatal, postpartum, contraception, and abortion care. 22 –27 After early pregnancy loss, patients may appreciate remote follow-up options to avoid potential logistical and emotional challenges of in-person assessment while still ensuring successful passage of the pregnancy. 27,28 Furthermore, with the Food and Drug Administration’s recent removal of the in-person dispensation requirement for mifepristone, remote management of early pregnancy loss may become more prevalent. 29,30 We sought to investigate the feasibility of a new telemedicine follow-up protocol for medication management of early pregnancy loss that was initiated during the COVID-19 pandemic.
Materials and Methods
We performed a retrospective chart review using data from the Complex Family Planning clinics associated with the University of Pennsylvania. These are two academic family planning clinics in which patients are seen for early pregnancy loss, induced abortion, and contraception. We offer medication management for early pregnancy loss at <13w0d gestation and medication abortion at ≤10w0d gestation consistent with widely accepted and researched guidelines. 10,11,31 We defined early pregnancy loss as a nonviable, intrauterine pregnancy with either an empty gestational sac or a gestational sac containing an embryo or fetus without embryonic cardiac activity <13w0d gestation. 10 Patient visits between April 1, 2020, and March 28, 2021, were included in the study. We excluded patients with pregnancy of unknown location. According to our clinical practice at the time of this study, individuals with pregnancy of unknown location were not offered medication abortion, and therefore this clinical scenario was excluded from this analysis. This study received exemption status from the University of Pennsylvania Institutional Review Board.
Medication administration
Medication management of early pregnancy loss and medication abortion was initiated at an in-person clinic encounter, at which time patients took 200 mg mifepristone orally and received a prescription for 800 mcg of misoprostol to be self-administered vaginally or buccally within 72 hours of mifepristone treatment. The clinical team counseled patients on emergency precautions for bleeding, pain, and infection, and advised them to call the office for issues arising ahead of their scheduled follow-up visit.
Follow-up protocol
In the context of the COVID-19 pandemic, our clinics initiated a telemedicine follow-up protocol for both medication management of early pregnancy loss and medication abortion. The new protocol began on April 1, 2020, and data were collected after the first year of implementation. Patients scheduled follow-up visits at the time of the in-person mifepristone administration and decided on mode of follow-up in conjunction with their providers. Both telemedicine and in-person follow-up appointments were scheduled to occur 1–2 weeks after the initial medication administration encounter.
Telemedicine follow-up was conducted through a synchronous video visit built into the electronic medical record system. During the scheduled telemedicine follow-up, providers utilized a standardized checklist (Fig. 1) for assessment of treatment success. Successful pregnancy passage was signaled by “yes” responses to questions one through four in the checklist. If responses indicated successful passage of the pregnancy, the patient was instructed to obtain and use a high-sensitivity urine pregnancy test four weeks from mifepristone administration. If the urine pregnancy test was positive, the patient was to contact the clinic for further evaluation in-person. If the urine pregnancy test was negative and the patient had no concerning symptoms, no further follow-up was required. If any responses during the telemedicine evaluation suggested incomplete abortion or other complications, the provider recommended additional in-person evaluation to occur in a timely fashion.
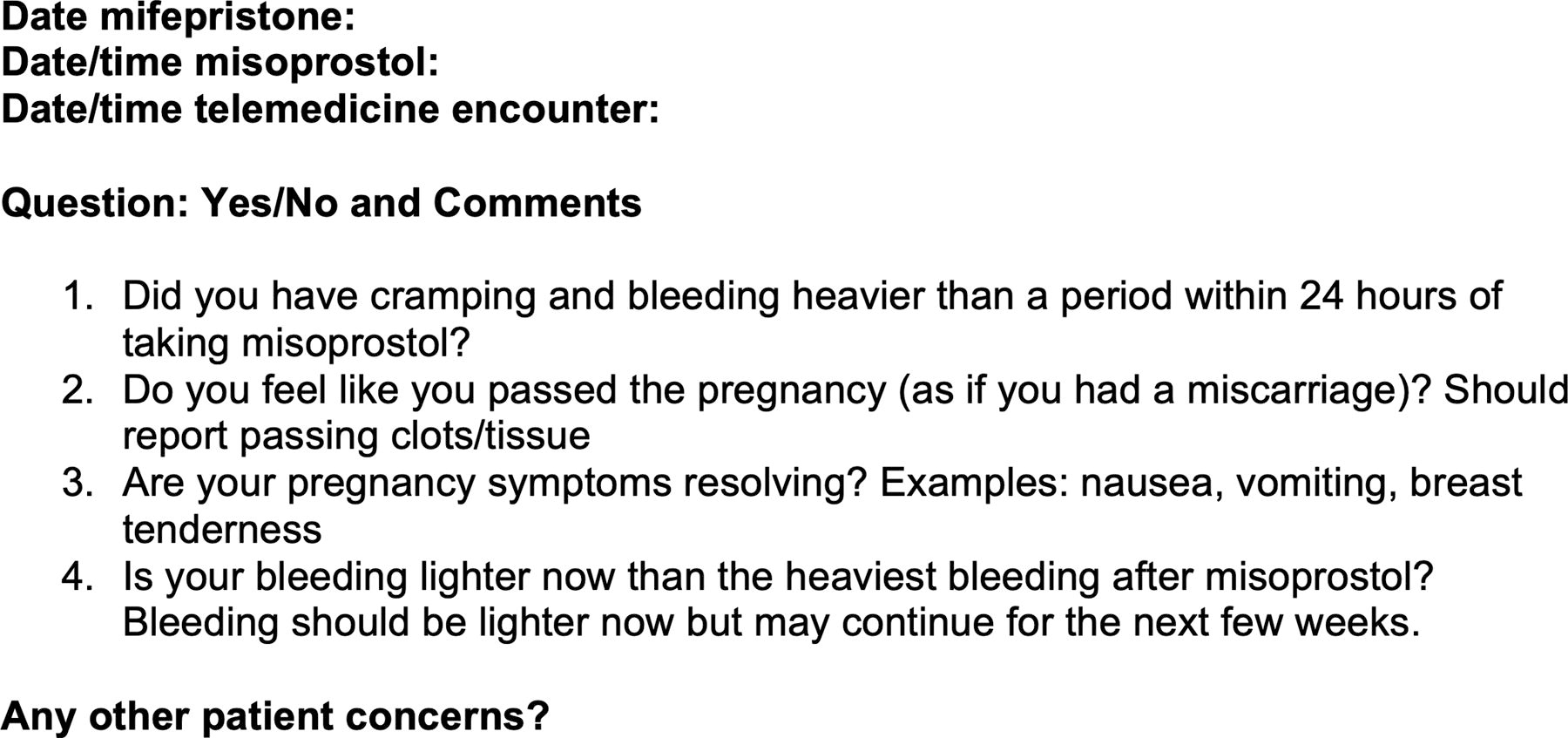
Clinical checklist utilized from 2020 through present day during telemedicine follow-up after medication management of early pregnancy loss and medication abortion from the Complex Family Planning clinics at the University of Pennsylvania.
During the scheduled in-person follow-up, the clinical team conducted a history, exam, and ultrasound. We defined treatment failure as the need for uterine aspiration after medication administration, based on a retained gestational sac on ultrasound or persistent symptoms of abnormal bleeding and/or pain. 32
Data and statistical analysis
Our primary outcome to determine the feasibility of this telemedicine protocol was the proportion of patients undergoing medication management of early pregnancy loss who planned for telemedicine follow-up and completed follow-up as per protocol. This included completion of the initial telemedicine follow-up visit as well as all other subsequent, recommended visits. Additionally, we compared this primary outcome with the proportion of patients undergoing medication management of early pregnancy loss who planned for in-person follow-up and completed follow-up as per protocol. We also compared the primary outcome with the proportion of patients undergoing medication abortion who planned for telemedicine follow-up and completed follow-up as per protocol. 13 –16
We considered feasibility as the extent to which our new protocol could be successfully used or carried out. With this in mind, we defined feasibility as a rate of completed follow-up as per protocol of over 80%. 33 –35
Statistical analysis included Chi-square and Fisher’s exact tests to compare outcomes for categorical variables. For continuous variables between two groups we employed T-tests and Wilcoxon rank-sum tests. When analyzing outcomes across our four treatment groups, we employed Kruskal–Wallis tests and one-way ANOVA for the continuous variables.
We collected secondary outcome data from the electronic medical record to describe complications by mode of follow-up. We individually reviewed emergency room encounters, hospital admissions, and any other available clinic visits from all hospital systems that were available in the electronic medical record for all study participants to capture complication data. Complications included emergency room presentations, infection, or blood transfusions received within 30 days of medication administration.
Results
During the study period, 181 subjects were eligible for inclusion. Of eligible subjects, 75 had medication management of early pregnancy loss and 36/75 (48%) chose telemedicine follow-up. A total of 106 had medication abortion and 69/106 (65%) chose telemedicine follow-up. These subjects were categorized into four groups: medication management of early pregnancy loss with planned telemedicine follow-up, medication management of early pregnancy loss with planned in-person follow-up, medication abortion with planned telemedicine follow-up, and medication abortion with planned in-person follow-up. These four groups were demographically similar, including in age, parity, and gestational age, across pregnancy type and mode of follow-up (Table 1). Patients with early pregnancy loss opted for in-person follow-up out of personal preference (18/39, 46%), desire to submit tissue for cytogenetic testing (3/39, 8%), insertion of an intrauterine device (1/39, 2%), and for unspecified reasons (17/39, 44%).
Demographics and Baseline Characteristics of Patients Undergoing Medication Management of Early Pregnancy Loss and Induced Abortion Between April 1, 2020, and March 28, 2021 from the Complex Family Planning Clinics at the University of Pennsylvania
Figure 2 illustrates participation in the telemedicine follow-up protocol for medication management of early pregnancy loss. Of patients undergoing medication management of early pregnancy loss who chose telemedicine follow-up, 29/36 (81%, 95% CI: 64–92) achieved successful follow-up as per protocol. Four patients (4/36, 11%) were not able to be reached for their initial telemedicine assessment and were lost to follow-up. Additionally, of the 6 patients who were recommended during their telemedicine visits to present to clinic in-person out of concern for incomplete abortion, 3 successfully completed this evaluation, while 3 were lost to follow-up at this subsequent visit. No patients in the entire cohort called to report a positive urine pregnancy test 4 weeks after misoprostol administration.
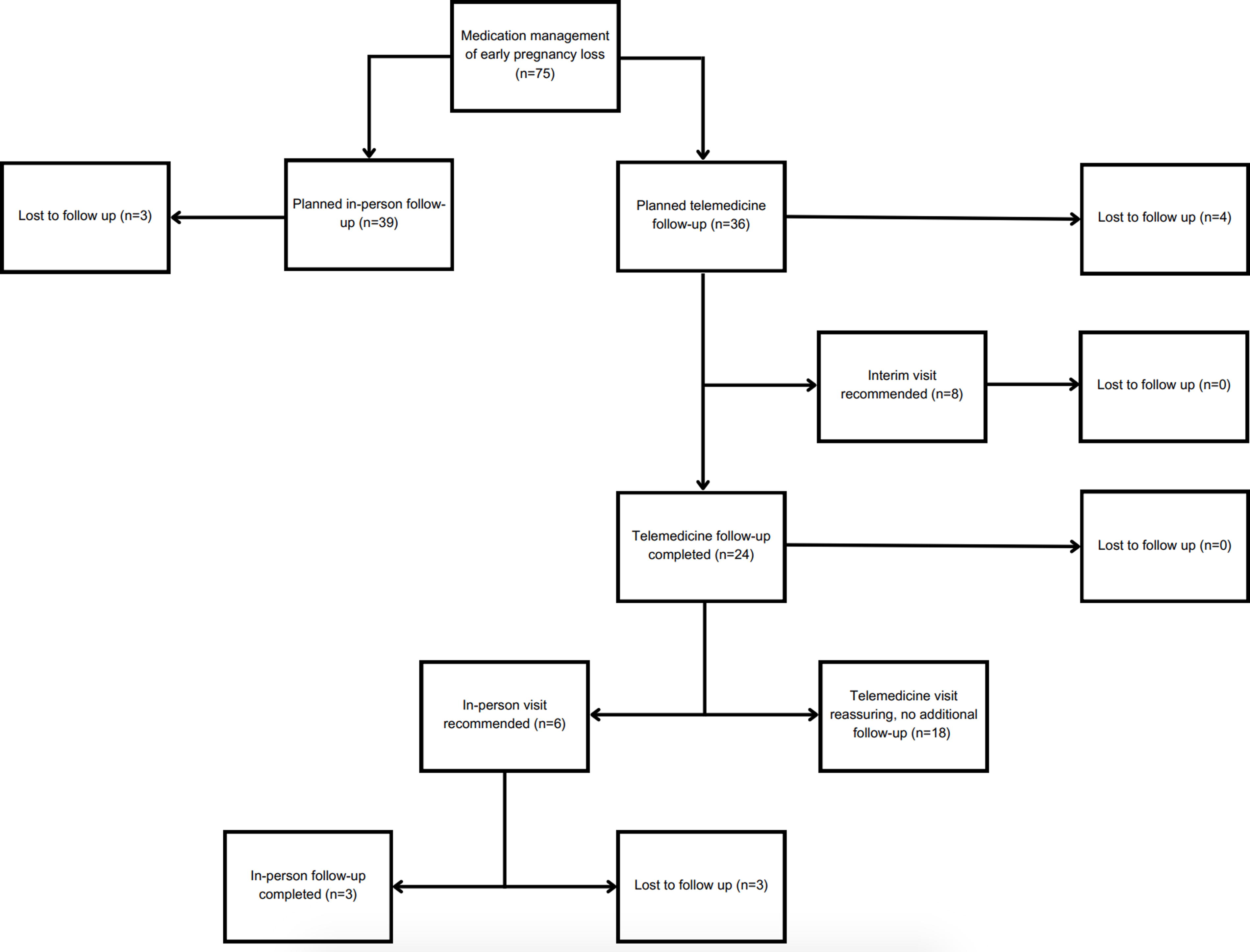
Flow chart of patient in-person and telemedicine follow-up after medication management of early pregnancy loss between April 1, 2020, and March 28, 2021, from the Complex Family Planning clinics at the University of Pennsylvania.
We compared follow-up as per protocol for patients with medication management of early pregnancy loss who elected for telemedicine follow-up with that of patients undergoing medication abortion who elected for telemedicine follow-up (Table 2). Completion of follow-up as per protocol was not significantly different between the medication management of early pregnancy loss and the medication abortion groups who planned for telemedicine follow-up (p = 0.06). Completed follow-up was also similar among patients undergoing medication management of early pregnancy loss who planned for in-person follow-up (p = 0.135). Table 2 describes completed follow-up rates across the comparison groups.
Completed Follow-up Rates for Patients Undergoing Medication Management of Early Pregnancy Loss and Induced Abortion with Planned Telemedicine or In-Person Follow-up Between April 1, 2020, and March 28, 2021 from the Complex Family Planning Clinics at the University of Pennsylvania
Comparisons were made between each group with the telemedicine follow-up early pregnancy loss group as the reference group and performed using Chi-squared tests.
Table 3 depicts outcomes and complications of medication management across all groups. Of patients with early pregnancy loss who planned for telemedicine follow-up, 4/36 (11%) had failure of medication management and chose uterine aspiration for management. This failure rate was similar to that among patients undergoing medication management of early pregnancy loss who planned for in-person follow-up (7/39, 18%), as well as among patients undergoing medication abortion who planned for telemedicine follow-up (8/69, 12%) (p = 0.74). One patient who underwent medication abortion was diagnosed with an ongoing pregnancy by ultrasound and subsequently had a uterine aspiration.
Treatment Outcomes and Complication Rates Among Patients Undergoing Medication Management of Early Pregnancy Loss and Induced Abortion Who Planned Telemedicine or In-Person Follow-up Between April 1, 2020, and March 28, 2021 from the Complex Family Planning Clinics at the University of Pennsylvania
Treatment failure of medication management was defined as the need for additional intervention after medication administration, based on a retained gestational sac or persistent symptoms of abnormal bleeding and/or pain.
Complications, defined as emergency room visit, infection, or need for blood transfusion within 30 days of treatment across groups, were rare and did not differ across early pregnancy loss and medication abortion groups, or by follow-up modality (Table 3).
Discussion
In the literature, remote follow-up strategies for medication abortion have been studied, and adherence to these protocols varied from 69% to 97.8%. 14,16,36 –40 In our study, we determined that telemedicine follow-up after medication management of early pregnancy loss was feasible, with a follow-up as per protocol rate of 81%. This was comparable to the follow-up as per protocol for early pregnancy loss patients who planned in-person follow-up, as well as for medication abortion patients who planned telemedicine follow-up.
Studies have shown that shared decision-making using evidence-based counseling leads to improved patient satisfaction related to management of early pregnancy loss. 9 With the onset of the COVID-19 pandemic in 2020, our practice began to offer telemedicine follow-up for medication abortion, which has been previously studied and validated, as well as after medication management of early pregnancy loss, which has not been previously studied. 13 –16 Although patients seeking medication management of abortion and early pregnancy loss may differ in goals and motivations for treatment, their outcomes in terms of success and efficacy determined by the absence of pregnancy tissue after medication administration are comparable. 10,11 In our study, telemedicine proved to be popular, with approximately half of early pregnancy loss patients in this cohort opting to follow up in this way. Even now, after the height of the pandemic, there are numerous reasons that might lead a patient to prefer telemedicine to in-person follow-up after early pregnancy loss. 27,41 –43 In other areas of obstetrics and gynecology, telemedicine has been associated with improvements in outcomes, while reducing illness exposure and barriers to care related to transportation, childcare, and finances. 22,23,25 –27
Additionally, changing regulations on mifepristone have expanded future opportunities for remote follow-up options after medication management of early pregnancy loss. Recently, the Food and Drug Administration lifted the Risk Evaluation and Mitigation Strategy requirement that mifepristone be dispensed by healthcare providers in person. 29,30 While mifepristone regulation is currently being contested in the judicial system, remote dispensation of mifepristone remains an option as of this writing. This opens the prospect for telemedicine consultation and pharmacy prescription of mifepristone for medication management of early pregnancy loss. In this scenario, telemedicine follow-up could be the final step of a completely remote treatment protocol. Given the current rapidly changing and restrictive reproductive healthcare landscape, remote options for early pregnancy loss follow-up have the potential to expand overall access to care and improve patient autonomy.
A limitation of our study is sample size thereby undermining the internal and external validity of our study. We included all eligible participants in the designated time period during which the protocol was utilized. We used comparison groups for early pregnancy loss and medication abortion to provide additional support for our findings. We compared complications across modes of follow-up after early pregnancy loss and medication abortion to preliminarily assess complications related to this new protocol and found few in each group. However, complications after medication management of early pregnancy loss and abortion are uncommon, and a larger sample would be needed to detect differences in adverse outcomes. One rare but important complication of medication abortion is ongoing pregnancy, which is not a risk in the early pregnancy loss population. While treatment failure rates for medication abortion were higher in this study than those in the published literature, these failures were defined primarily by bleeding symptoms, rather than the presence of a gestational sac or ongoing pregnancy, and our clinical staff may have opted to treat with uterine aspiration when others may not have. These preliminary data suggest that telemedicine follow-up after early pregnancy loss does not elevate risk of bleeding, infection, or emergency care.
A limitation of this study was our inability to definitively assess treatment success. Due to the practical nature of this new clinical protocol, patients who sought telemedicine follow-up after early pregnancy loss did not also receive a pelvic ultrasound to confirm pregnancy completion. Thus, we did not have an opportunity to compare our virtual assessment of treatment success to the current gold standard. It is possible that interview questions used to assess treatment success after medication abortion do not identify treatment failure as accurately in the setting of early pregnancy loss. Although the lack of any reports of positive urine pregnancy test results during follow-up indicates high rates of successful pregnancy completion, we do not know the proportion of patients who actually completed the recommended urine pregnancy test since patients were asked to call the clinic only for positive test results. Additionally, we recognize patients may have sought clinical care outside of the research team and clinic. Although our chart review included access to records from multiple hospital systems, this may not have sufficiently captured every complication or emergency room visit at other hospitals.
Future studies should confirm the accuracy of treatment success as determined during telemedicine follow-up and measure patient satisfaction as a component of feasibility with this protocol. We recognize that the satisfaction and decision to follow up in-person or by telemedicine may differ between early pregnancy loss and abortion groups due to stigma and access. In addition, following serial human chorionic gonadotropin trends as an outpatient, which has not been well studied after early pregnancy loss, may enhance opportunities for remote follow-up. 19 While some patients and providers may prefer in-person assessment after medication management of early pregnancy loss, remote follow-up is a valuable alternative for many patients. The uptake and feasibility of telemedicine follow-up after medication management of early pregnancy loss in our patient population indicate that this new protocol warrants further study.
Footnotes
Authors’ Contributions
Study concept and design were by A.H.R., A.N.F., and J.C. Acquisition and analysis of data were by A.H.R., N.K., S.N., and J.C. Interpretation of data and critical revision of the article for important intellectual content were performed by A.H.R., A.N.F., S.S., C.A.S., and J.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.