
Abstract
Background:
Polycystic ovary syndrome (PCOS) is a common endocrine condition, affecting up to 20% of reproductive aged women worldwide. Polycystic ovarian morphology (PCOM) may be present, but is not required for diagnosis. Our study seeks to evaluate the utility of ultrasound in diagnosing or excluding PCOS by 2023 International Guidelines Criteria.
Materials and Methods:
Subjects were patients seen in a tertiary care referral clinic in whom other causes of hyperandrogenism (HA) were ruled out. All underwent complete history, physical, modified Ferriman Gallwey scoring, and serum androgen testing; followed by transvaginal ultrasound (TVUS) to assess ovarian morphology if indicated. PCOM was identified as antral follicle count ≥20 and/or ovarian volume >10 mL in at least one ovary. After clinical classification, PCOS was diagnosed by at least two of three: biochemical/clinical HA, ovulatory dysfunction (OD), and PCOM. Statistics were calculated using Fisher’s exact test and chi-square.
Results:
In total, 454 subjects were included. 299 were classified as group A/B and did not require TVUS for diagnosis. Of 82 subjects with HA alone, 50 (61.0%) were classified as group C after demonstrating PCOM. Fifty-five subjects had OD alone, 37 (67.3%) of which were classified as group D based on PCOM. In total, 137/454, or 30.2% of subjects required TVUS for diagnosis or exclusion of PCOS.
Conclusions:
TVUS was necessary in less than one-third of subjects, primarily identifying PCOS groups C or D. Selective use of ovarian ultrasonography may reduce the costs and complexity of epidemiological and clinical studies for PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is prevalent among women of reproductive age, as it is thought to affect anywhere from 10–13% of women globally. 1 The diagnosis of PCOS has long been a topic of debate with guidelines that have shifted and evolved over the past 2 decades including the National Institutes of Health (NIH) 1990 criteria, Androgen Excess and Polycystic Ovary Syndrome Society (AE-PCOS) Society criteria, and Rotterdam criteria. 2 –5 Recently published guidelines from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome (2023 International Guidelines) established a stepwise diagnostic algorithm for diagnosis in the hopes of simplifying this process. 1 These guidelines uphold and provide nuance to the previously established Rotterdam Criteria, which indicate that upon exclusion of other androgenizing conditions, PCOS is characterized by two of three cardinal features: (i) clinical or biochemical hyperandrogenism (HA), (ii) ovulatory dysfunction (OD), and (iii) polycystic ovarian morphology (PCOM) or elevated anti-mullerian hormone level (AMH). 3
The Rotterdam and AE-PCOS Society criteria recognize variation in the phenotypes of PCOS, and much research has been conducted to ascertain clinical significance of phenotypic classifications. PCOS can therefore be sub-classified as (i) frank PCOS: HA + OD + PCOM, (ii) ovulatory PCOS: HA + PCOM, (iii) non-PCO PCOS: HA + OD, and (iv) normoandrogenic PCOS: OD + PCOM. 6 It has been well-established and is clear from these sub-classifications that PCOS can exist in the absence of PCOM. Conversely, it has been shown that PCOM may be present without other clinical and biochemical feature of PCOS. 7 Moreover, the updated guidelines propose with moderate quality evidence the use of serum AMH measurements as a potential proxy for PCOM, although it is noted with conditional evidence that follicle number per ovary and ovarian volume should be considered accurate ultrasound markers as well. 1 Nonetheless, transvaginal ultrasound (TVUS) for antral follicle count (AFC) and ovarian volume remains a mainstay of the diagnostic workup for this condition, perhaps in part due to a lack of consensus regarding an AMH cutoff for diagnosis. Transabdominal ultrasound can be used for diagnosis as well with a threshold of ≥10 mL ovarian volume or ≥10 follicles per section in either ovary. 1 TVUS, while the most accurate for diagnosis of PCOM, also represents the most costly and the most invasive portion of most PCOS workups. 8 As such, this study sought evaluate the frequency with which ultrasound evaluation was required for ruling in or ruling out the diagnosis of PCOS by 2023 International Guidelines in a population presenting for evaluation of hyperandrogenism to a tertiary care center, thus lending credence to the International Guideline’s newly outlined diagnostic algorithm (Fig. 1).
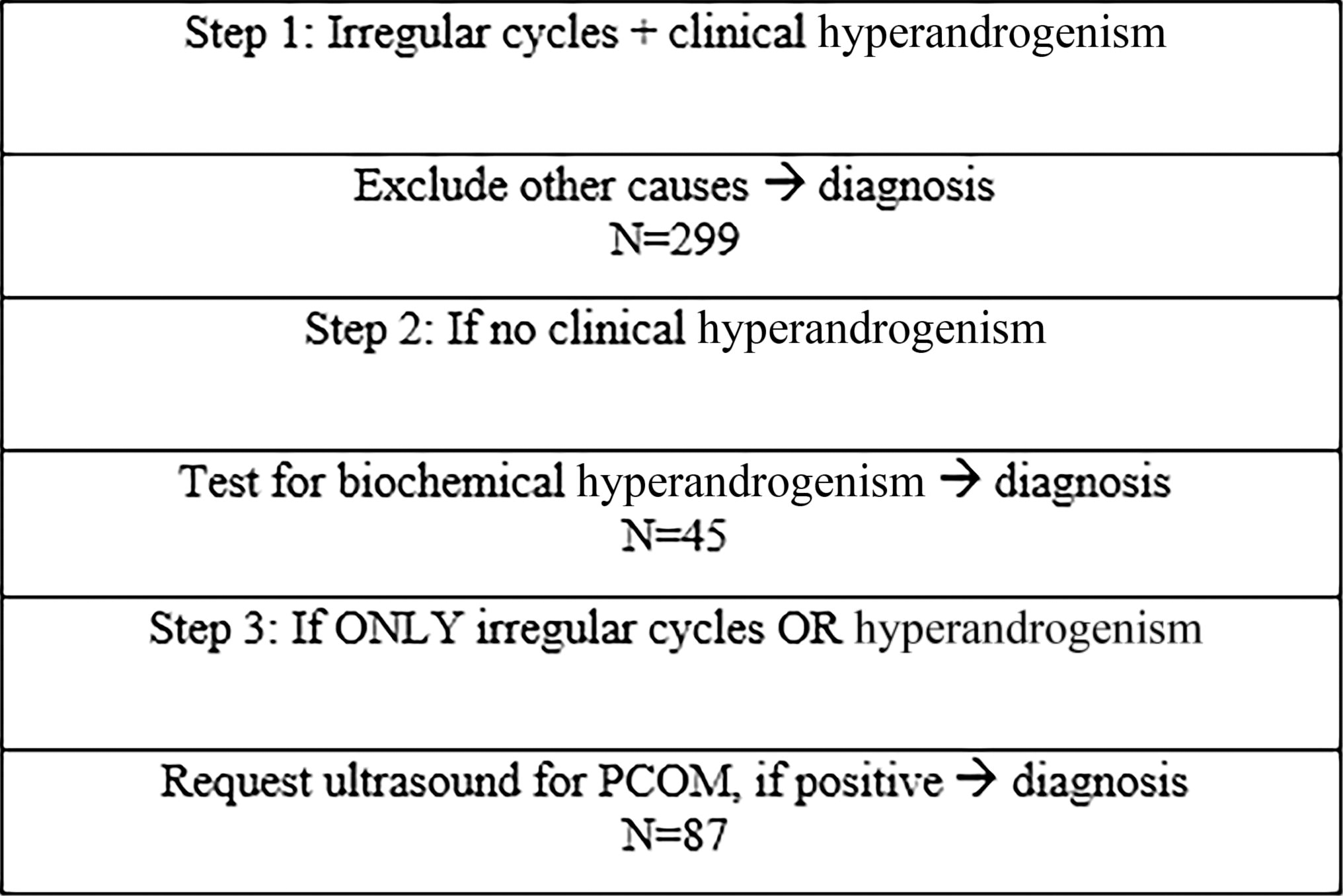
Algorithm for PCOS Diagnosis Adapted from 2023 Guidelines. 1
Materials and Methods
Data collection
This study involved a secondary analysis of a dataset previously obtained from a cohort of patients referred to an androgen excess clinic at a tertiary care center for evaluation. In total, 645 subjects were included in the analyzed database.
Subjects
Subjects included for this analysis were patients consecutively seen in a tertiary care referral clinic at Cedars-Sinai Medical Center for evaluation of androgen excess, aged 19–45 years. Other possible causes of HA or OD including thyroid dysfunction, hyperprolactinemia, non-classical adrenal hyperplasia, were ruled out. Exclusion criteria for analysis were pregnancy and inability to provide informed consent. Those on oral contraceptives (OCs) or other hormone-blocking agents were not excluded. Subjects were also excluded from analysis if their age at analysis were <19 years or >45 years, visual scoring of hair growth for hirsutism was not performed or recorded, serum evaluation for androgens was indicated but not completed, they failed to provide a menstrual history, or TVUS was indicated and not completed. All subjects provided informed consent for study participation prior to inclusion. Initial study and data collection were approved by the Cedars-Sinai Institutional Review Board.
Protocol
Subjects were evaluated with a complete history and physical examination. History obtained included extensive menstrual and gynecological history as well as subjective experience of hirsutism and acne. Oligo-ovulation was defined as fewer than eight menstrual cycles per year, menstrual cycles that were <21 or >35 days in length, or a luteal phase progesterone of less than 3 ng/mL, indicating anovulation. 1,5 Physical exam included metrics such as weight, waist circumference, and evaluation of clinical HA using modified Ferriman Gallwey (mFG) scoring. 9 All participants were evaluated by a single trained physician and were not excluded for use of anti-androgenic or depilatory treatment. Hirsutism was defined by an mFG score ≥4. 1,10 The diagnosis of PCOS was made by the 2023 International Guidelines criteria. Subjects were therefore required to be positive for at least two of three: biochemical or clinical HA, OD, or PCOM to meet criteria for diagnosis.
All subjects underwent blood collection for hormonal assay. Serum androgens evaluated included free testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS). Serum free testosterone values were evaluated by equilibrium dialysis (Quest Diagnostics; San Juan Capistrano, CA, or LabCorp; Calabasas, CA). 11 DHEAS levels were determined using quantitative electrochemiluminescent immunoassay (ARUP Laboratories; Salt Lake City, UT, Quest Diagnostics, or LabCorp). Elevations were determined based on the laboratory reference range, or if unavailable, published upper normal limits for normally cycling premenopausal women. 12,13 Other pathological causes of elevated androgens, such as non-classical adrenal hyperplasia, were excluded appropriately.
Subjects also underwent TVUS to assess ovarian volume and morphology, if indicated. Indication for ultrasound was a history and physical exam that indicated the presence of either hyperandrogenism or ovulatory dysfunction but was not required for inclusion if the subject was found to have both. PCOM was identified as an AFC ≥20 in at least one ovary and/or ovarian volume >10 mL. AFC included a count of all cystic areas 2–9mm in diameter throughout the entirety of a single ovary. Ovarian volume calculations were performed using a standard ellipsoid approximation formula: 0.523 × length × width × thickness, measured in centimeters. Transvaginal ultrasound was conducted with a 6.26 MHz frequency transducer probe (λ = 47.9 m), and most ultrasounds were conducted by a trained physician.
We should note that some AFCs were recorded as being above a certain number, but an exact number was not given, i.e., >12 or >15. In these cases, it was presumed that the actual AFC was difficult to obtain but was not >20, and therefore unless the ovarian volume was >10 mL these subjects were deemed not to have PCOM. Given that using ovarian volume for diagnosis is an accepted practice per the 2023 Guidelines in the absence of an appropriate follicle assessment, these subjects were still included in analysis.
Statistical analysis
Subjects were classified into one of four clinical groups; Group A: HA + OD + PCOM, Group B: HA + OD, Group C: HA + PCOM, and Group D: OD + PCOM. Statistics were calculated using Fisher’s exact test and chi-square analysis, and a p-value of <0.05 was considered statistically significant.
Results
Of 645 eligible subjects in our referral population, 18 were excluded for a diagnosis other than PCOS, 56 were excluded for age outside the parameters used for this study, 26 were excluded for lack of available mFG score, 75 were excluded for lack of menstrual history provided. Of the 470 remaining subjects, one was excluded for lack of hirsutism without completing biochemical androgen testing, and 15 were excluded for history indicating HA or OD alone, but ultimately did not undergo TVUS to evaluate for PCOM.
In total, 454 subjects aged 19–45 years were included in the analysis (Table 1). Eighteen had neither OD or HA and therefore did not require ultrasound evaluation for PCOM, as regardless of the results they would not be diagnosed with PCOS. In clinical classification of subjects, 299 were found to have OD and HA, and therefore fell into group A or B (“classical PCOS”) and did not require TVUS for diagnosis. Of these, 34 did not undergo TVUS. Of those who did complete this portion of the study, 201/265 (75.8%) demonstrated PCOM (i.e., group A) (Fig. 2). Therefore, 201 subjects were classified as group A, and 98 subjects were classified as group B.
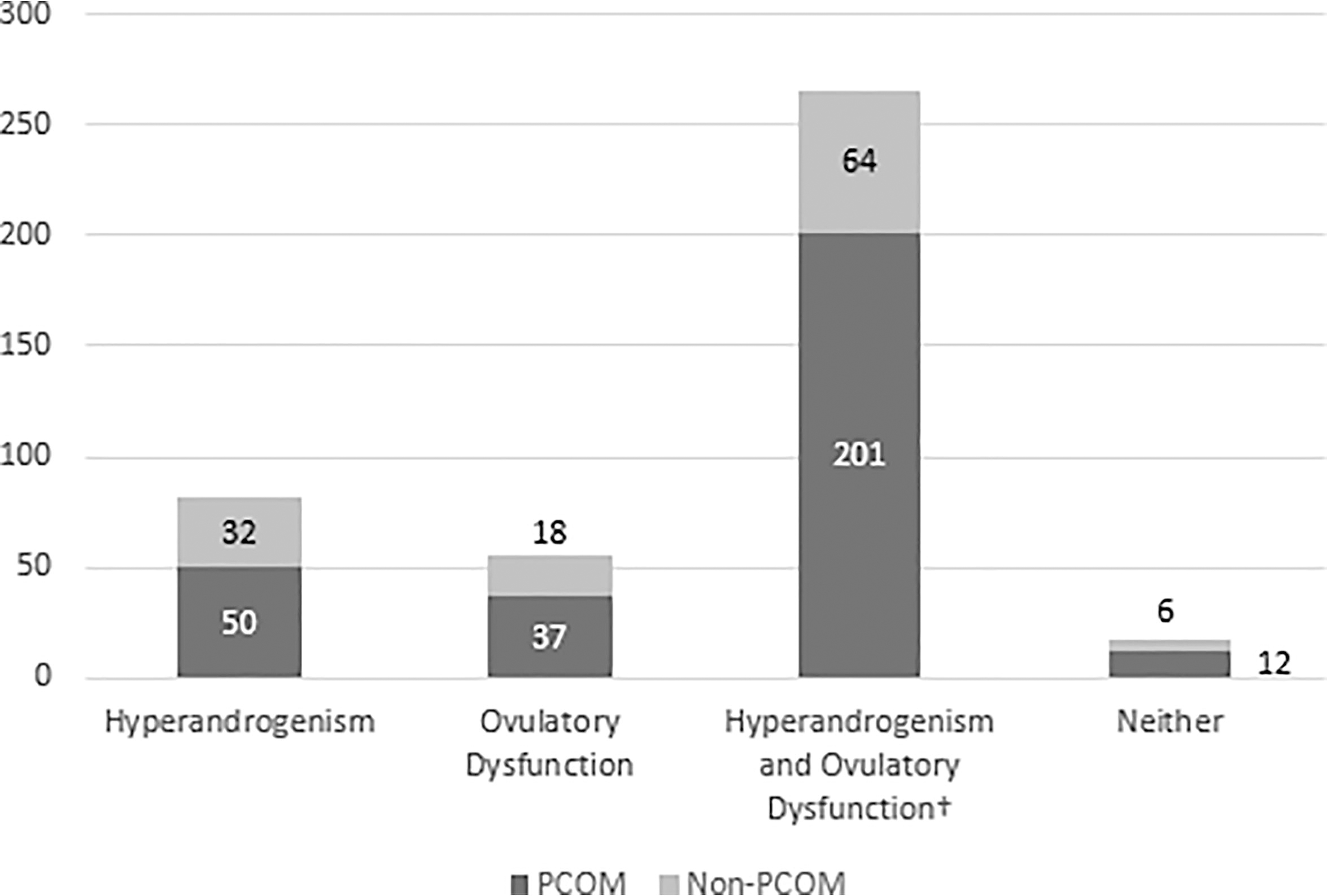
Rates of Polycystic Ovarian Morphology on Ultrasound by Phenotypic Classification. †Thirty-four patients with both hyperandrogenism and ovulatory dysfunction did not complete TVUS, but were still included given this was not necessary for diagnosis.
Subjects Demonstrating Characteristics of Interest
420 subjects underwent ultrasound as this was not necessary if both hyperandrogenism and ovulatory dysfunction were present.
There were 82 subjects found to have HA without OD who underwent ultrasound, 72 of these demonstrating mFG score ≥4 and an additional 10 demonstrating elevated serum androgen levels alone. Fifty subjects (61.0%) were classified as PCOS group C after demonstrating PCOM, and 32 had HA alone. Fifty-five subjects had OD without HA and underwent ultrasound, 37 (67.3%) of which were classified as group D based on the presence of PCOM, 18 demonstrated OD alone. No significant difference was found in the rates of PCOM between subjects with HA without OD or OD without HA (p = 0.475), and a chi-square analysis of all clinical groups showed no significant difference in rates of polycystic ovarian morphology (χ2 = 7.59, p = 0.055). In total, 137/454, or 30.2% of subjects required TVUS for diagnosis or exclusion of PCOS (Fig. 3). Of these, 87/137 (63.5%) were diagnosed with PCOS. Of all subjects ultimately diagnosed with PCOS, 87/386 (23.6%) required TVUS to make the diagnosis.
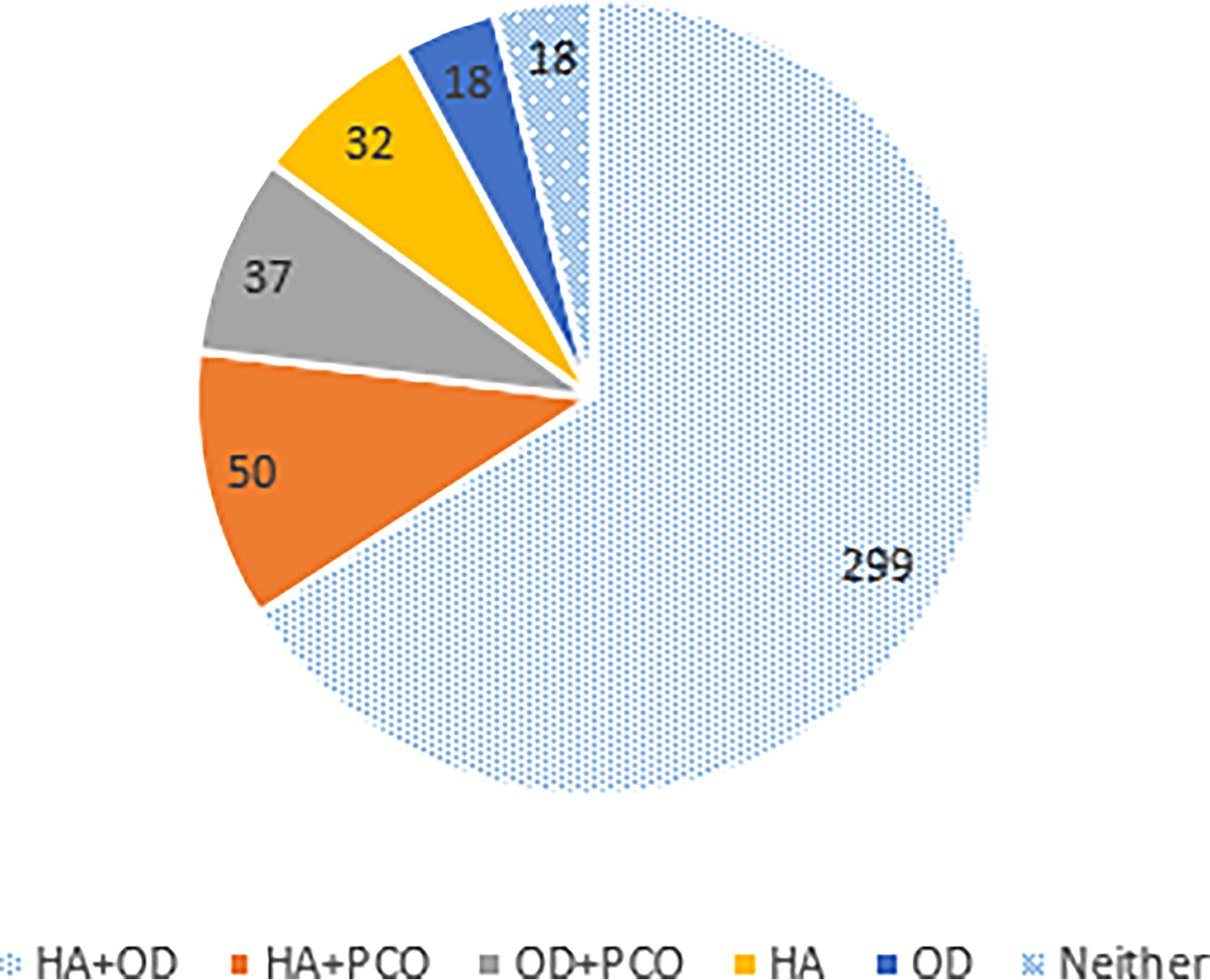
Phenotypic Classifications of Analyzed Subjects. Note that phenotypes represented by a solid color required ultrasound for diagnosis; those represented by a non-solid color did not.
Discussion
This study demonstrates the utility of clinical subgroup classification in stratifying the need for TVUS in the diagnosis of PCOS. In our referral-based population, about one-third of subjects required ultrasound for inclusion or exclusion of the diagnosis, supporting the idea that diagnosis of PCOS for patients with higher pretest probability can be streamlined and expedited. Nonetheless, the finding that the rate of PCOS diagnosis by TVUS is not significantly different between subjects with OD without HA as compared with those with HA without OD underscores an inability to predict PCOS diagnosis appropriately or accurately based on the presence of either factor alone. This finding, and our study as a whole, thus emphasizes the importance of appropriate phenotypic classification based on history, physical, and serum lab evaluation in accordance with the 2023 International Guidelines.
Prior investigations suggest that up to one-third of affected women visit three or more health care providers over 2 years before receiving a diagnosis of PCOS. 14,15 It is therefore unsurprising that PCOS patient dissatisfaction with clinical care is high, particularly as it relates to health care providers, the diagnostic process, and initial treatment. 16 PCOS is a lifelong disease with potentially harmful sequelae such as infertility, endometrial hyperplasia or cancer, cardiovascular disease, and metabolic dysfunction, all of which have been well-documented. 17 Diagnostic delays therefore have the potential to result in increased patient burden as well as a delay in the implementation of preventative care often necessitated by a diagnosis of PCOS. Moreover, delayed PCOS diagnosis is associated with higher rates of difficulty achieving pregnancy. 18
In general, women with PCOS have a higher mean age at first childbirth and are more likely to be over 35 years at first childbirth than non-PCOS women and data indicates that those diagnosed after 25 years of age have lower fecundity than those diagnosed before this age. 19 Nonetheless, after diagnosis fertility rates among those with PCOS have been demonstrated to be able to be restored to those of the background population, suggesting the efficacy of treatment once a diagnosis is made. 20 By expediting PCOS diagnosis, and therefore treatment, there is a significant potential to improve future reproductive outcomes and time to pregnancy in this patient population.
The 2023 International Evidence-Based Guidelines for the Assessment and Management of Polycystic Ovary Syndrome aim to alleviate some of the diagnostic delay by providing a simplified and stepwise algorithm, similar to the one used in our study. 1 Importantly, diagnosis is simplified in patients presenting with clinical evidence of HA and irregular menstrual cycles, and serum AMH is now an approved alternative to transvaginal ultrasound. Though a diagnostic threshold has yet to be established for serum AMH, the use of either TVUS or AMH testing is now recommended only when either menstrual dysfunction or HA alone is present in a patient with suspected PCOS.
In addition, the updated guidelines specify the lack of utility of ultrasound in adolescent subjects, and therefore directly advise against its use in this patient population. The algorithmic changes may, in many cases, obviate the need for TVUS, which is estimated to be the highest-cost test in the standard evaluation for PCOS. 8 In addition, less frequent TVUS decreases the need for an intimate portion of the evaluation, which can sometimes be associated with pain or even trauma. 21,22 Our results therefore affirm and support the newly released guidelines, as a similar framework was effective for phenotypically classifying patients and determining their need for TVUS.
A notable strength of this study is the robust sample size of 454 women who underwent history, physical, serum labs, and when indicated, TVUS. Another strength of the study is the fact that we did not exclude subjects who were under treatment with OCs, anti-androgenic treatments, or using depilator treatment for unwanted hair, thus minimizing the risk of excluding affected individuals.
Study limitations include the referral-based nature of the subject population to an androgen excess clinic for evaluation, which understandably brings into question the generalizability to an unselected population. 23 A similar study in an unselected and medically unbiased population would likely be of great benefit in the future. Also, approximately 18% of subjects were excluded from analysis for having incomplete data. In addition, at the time of data collection, AFC was frequently recorded as “greater than 12” without indicating an exact number due to previously used guidelines for ultrasound diagnosis of PCOM. 24 For purposes of this analysis, these subjects were not considered as meeting current criteria for PCOM, and some of these subjects may have actually had PCOM but were not noted as such. Also, the lower resolution of the ultrasound machine used in this study may have led to under-reporting of PCOM, as AFC is less accurate with transducer probe frequencies <8 MHz. 25 Serum labs reported for this analysis did not include total testosterone and labs were drawn at various locations in the Los Angeles area, each of which used different reference ranges, with reference ranges in some cases not reported at all. The fact that this study did not exclude patients on OCs, anti-androgenic treatments, or using depilator treatment, while a strength of the study (see above) could also be a limitation, as subjects with hirsutism and HA may have been under-represented in our cohort.
In summary, in our study population 30.2% of subjects required ultrasound for the diagnosis or exclusion of PCOS, primarily in the detection of PCOS groups C and D. By using appropriate phenotypic classification parameters and the algorithmic criteria laid out in the 2023 International Guidelines, two-thirds of the population was able to receive a diagnosis without the need for ovarian ultrasonography. Our findings therefore uphold and ratify the recommendations of the guidelines, emphasizing the importance of swift and ubiquitous incorporation of these algorithms into practice. By employing these algorithmic diagnostic methods, practitioners stand to reduce the costs and complexity of epidemiological and clinical evaluation for this extremely common condition with a multitude of health repercussions. Finally, studies assessing this issue in population-based medically unbiased cohorts are needed. 26
Footnotes
Authors’ Contributions
All authors contributed to the study meaningfully with roles as follows: conceptualization, L.P. and R.A.; methodology, L.P., R.A., M.P, J.C.; statistics, L.P.; formal analysis, L.P.; investigation, M.P., J.C., L.P.; resources, L.P., J.W.; writing—original draft preparation, L.P., J.W.; writing—review and editing, J.W., R.A.; supervision, R.A. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
Lauren Pace, Joshua Waldeck, Jessica Chan, and Margareta Pisarska have no competing interests to declare. Ricardo Azziz serves as a consultant for Spruce Bioscience, Core Access Surgical Technology, PostEra, and May Health, as advisor for Arora Forge, and as investor in Martin Imaging.
Funding Information
This study received no external funding.