
Abstract
Objective:
Failure to “make weight” carries significant consequences for military personnel including additional training burdens, stigma, possible demotion, or even separation from service. The aim of this study was to examine potential gender differences in, and investigate relationships between, military making weight behavior and obesity, eating pathology, and mental health later in life.
Method:
Iraq and Afghanistan war era Veterans (N = 1,126, 51.8% women) completed the Making Weight Inventory (MWI), a measure of making weight behaviors engaged in during military service, and validated measures of eating behavior and mental health. Analyses compared participants who engaged in at least one making weight behavior (MWI+) versus those who did not (MWI−).
Results:
Overall, 41% (n = 462) of the sample was categorized as MWI+. The most frequently endorsed making weight behavior was excessive exercise (35.7%). Among those who were MWI+, there was a significantly greater proportion of women (58.2% versus 47.3%, p < 0.001). The MWI+ group had higher rates of obesity (52.4% versus 26.2%) and had significantly higher levels of dietary restraint, emotional eating, food addiction, depression, anxiety, and posttraumatic stress disorder than the MWI− group (p’s < 0.001).
Conclusions:
Military making weight behavior was associated with female gender, higher weight, eating pathology, and mental health later in life. Collectively, these findings suggest these factors may place female service members at a disadvantage for career advancement and salary. Efforts to better understand and address extreme making weight efforts in military populations, particularly in female service members and Veterans, are warranted.
Introduction
Eating disorders, disordered eating, and overweight are all observed at high rates in both active-duty military service members (ADSMs) and Veterans, and these rates are similar or higher than rates observed in civilians. 1 –6 This is surprising given that military personnel are required to pass biannual physical fitness tests, including mandatory weigh-ins with strict body composition requirements. 7
Pressure to meet preestablished weight cutoffs and body composition requirements may lead to service members engaging in making weight behaviors. Making weight is defined as meeting a preestablished weight cutoff for qualification purposes. Failure to “make weight” at weigh-ins carries significant consequences for military personnel including additional training burdens, stigmatizing measurements, and potential demotion or even separation from service. 8,9 For example, ADSMs who do not make weight may be subject to a “tape test.” This involves measurement of the neck and waist for men and the neck, waist, and hips for women. 10 In a descriptive study of 377 military members attending a weight management group, 71.5% reported that they felt the tape test was not an accurate measurement of their body mass index (BMI). 11 This study points out that, to meet requirements, ADSMs often turn to unhealthy weight loss measures, which may have detrimental long-term impacts on health (e.g., tachycardia, dehydration, and risk of heart attack or stroke). 11 This includes weight loss efforts made by those who may not be classified as traditionally overweight, but whose body composition may not be captured well by current standards. 11 Failure to meet Physical Fitness Assessment standards three times in the most recent 4-year period can result in the risk of administrative separation from the Navy or lack of promotion. 9,12,13 Given the severe repercussions of these failures, it makes sense that ADSMs may engage in unhealthy and extreme weight control strategies in an effort to meet weight requirements (henceforth referred to as making weight behaviors). Making weight behaviors can include things such as engaging in vomiting, laxative use, diuretic use, skipping meals, excessive exercise, and/or sauna or rubber suit use. Excessive exercise is defined as behavior that impedes other life domains, behavior that may cause physical injury, or behavior that is engaged in despite injury or illness. New research is demonstrating unintended consequences of making weight behaviors. 8,14
Gender may be an important factor with regard to making weight behaviors. In one study, 64% of women, in comparison with 39% of men, engaged in at least one making weight behavior during active duty. 15 A study of 1,015 civilian adolescent and young adult females found that participants using diet pills and laxatives, which are common making weight behaviors in the military population, had a higher risk of being diagnosed with an eating disorder in the following five years. 16 Furthermore, a systematic qualitative study identified the need to meet military weight requirements as a stressor and potential risk factor for long-term unhealthy eating habits in female Veterans. 17 Another study with 307 women and 453 men found that, particularly in female Veterans, mental health comorbidities are positively associated with eating disorder status. 18 This is critical to know given that female Veterans are more likely to report symptoms of, and have a probable, eating disorder diagnosis than male Veterans. 19 More quantitative data are warranted on making weight behaviors in female Veterans.
Beyond gender differences, there is evidence that making weight behaviors may increase risk for eating disorders later in life. Disordered eating behaviors can impact those of any age, including older adults. In a sample of 120 mostly male Veterans seeking weight management services, one-third of the participants who had overweight/obesity endorsed making weight behaviors during active-duty service. 8 These Veterans were shown to be more likely to currently engage in maladaptive eating behaviors such as binge eating, vomiting, emotional eating, food addiction, and night eating when compared with Veterans who did not screen positive for military making weight behaviors. The most frequently cited method of making weight was excessive exercise (reported by one-quarter of the sample), followed by skipping meals, sauna/rubber suit, laxatives, diuretics, and vomiting. Veterans in this sample who engaged in making weight behaviors were more likely to be younger, to be an ethnic/racial minority, and to engage in current maladaptive eating behaviors. 8
The objective of the current study was to examine gender differences in military making weight behaviors with a large Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) Veteran sample balanced by gender. To date, no studies have examined gender differences in efforts to make military weight and fitness standards nor has past research examined if those who engage in making weight behaviors differ on measures of psychiatric functioning. The current study aims to examine potential gender differences, and potential weight, eating behavior, and mental health differences between Veterans who engaged in unhealthy weight loss practices to make military weight (MWI+) and those who did not (MWI−). It is hypothesized that women will have engaged in significantly more making weight behaviors than men. Moreover, it is hypothesized that the MWI+ group will report significantly worse mental health and eating pathology outcomes than the MWI− group and have higher weight and rates of obesity than the MWI− group.
Materials and Methods
Participants and procedures
Participants were male and female OEF/OIF/OND Veterans who participated in the Women’s Veterans Cohort Study 2 (WVCS-2), a mixed methods study focused on examining gender differences in health care utilization and health outcomes. Detailed procedures describing WVCS-2 have been previously published. 19 –21 The current study is an analysis of 1,146 baseline survey data using a subset of WVCS-2 measures. Participants were eligible for inclusion in the current study analyses if they completed the measures of eating behavior needed to determine their “making weight” status, resulting in a final analytic sample of 1,126 Veterans (98%).
Measures
Sociodemographic, military service, and weight-related characteristics
Sociodemographic information included self-reported age, gender, race, ethnicity, marital status, income, and education level. Military service information included service branch and component. Military service information included service branch (e.g., Army, Navy, and Air Force) and component (Active-duty, Reserve, and National Guard). The Veteran’s current BMI (kg/m2) was calculated using self-reported height and weight.
The making weight inventory
The Making Weight Inventory (MWI) is a 6-item measure of use of weight control strategies to meet military service weight requirements. The questionnaire asks, “When you were in the service, how frequently did you use the following to make weight?” The questionnaire includes the following six behaviors: vomiting, laxative use, diuretic use, fasting or skipping meals, excessive exercise, and use of saunas or rubber suits. Participants chose from a seven-point Likert scale ranging from 0 (never) to 6 (always). Responses to each item were dichotomized with 0 coded as “no” and 1–6 coded as “yes.” A positive response (“yes”) to any of the six items indicates engagement in making weight behavior (MWI+). The MWI has been shown to have good internal consistency in a Veteran population seeking weight management treatment (8) and in this study population of OEF/OIF/OND Veterans as well (α = 0.81).
Eating pathology
Eating pathology outcomes included current self-reported dietary restraint, binge eating, emotional eating, and food addiction. Dietary restraint was assessed using the subscale items from the short-form version of the Eating Disorder Examination Questionnaire (EDE-Q7) with possible scores ranging from 0 to 6. 22 The average number of binge eating episodes per month over the past three months was assessed using the Eating Disorder Diagnostic Scale-5 (EDDS-5). Emotional eating was assessed using the Yale Emotional Overeating Questionnaire (YEOQ) 23 with scores ranging from 0 to 36. Food addiction was assessed using the Modified Yale Food Addiction Scale (mYFAS) 24 with possible scores ranging from 0 to 7. All measures were scored according to the provided scoring instructions. The EDE-Q7, EDDS-5, YEOQ, and mYFAS all have good psychometric properties, 23 –27 and Cronbach’s alphas for the current study demonstrated high internal consistency (α’s = 0.80–0.96).
Mental health characteristics
Mental health outcomes included symptoms of depression, anxiety, and PTSD and were assessed using the following measures, respectively: Patient Health Questionnaire-8 (PHQ-8), 28 Generalized Anxiety Disorder-7 (GAD-7), 29 and PTSD Checklist-Military (PCL-M). 30 PHQ-8 responses were summed to create a continuous measure ranging from 0 to 24. GAD-7 responses were summed to create a continuous measure ranging from 0 to 21. PCL-M responses were summed to create a continuous measure ranging from 17 to 85. All measures are well-validated and have been shown to have good psychometric properties. 31 –33 Cronbach’s α for the current study ranged from 0.80 to 0.92.
Statistical analysis
Data analyses were conducted using SAS version 9.4. Participants were categorized into two groups based on their responses to the MWI: those who reported engaging in at least one making weight behavior (MWI+) and those who did not (MWI−). Chi-square tests were used to examine gender differences in making weight behaviors. To compare the MWI+ and MWI− groups on sociodemographics, military service, weight-related characteristics, eating pathology, and mental health characteristics, unadjusted chi-square tests were used for categorical variables and unadjusted t tests for continuous variables. Linear regression models were also used to compare the groups on eating pathology and mental health outcomes. We fit a separate model for each one of the seven outcomes: dietary restraint, emotional eating, food addiction, binge eating, depression, anxiety, and PTSD (all continuous variables). The primary predictor in the models was engagement in making weight behaviors (MWI± versus MWI−), a categorical variable. Models were initially adjusted for age (continuous), gender (categorical), and BMI (continuous) because they are established predictors of eating pathology that were decided a priori. The models were then refitted to additionally include the following categorical variables that differed between groups in Table 1: race (White versus not), Hispanic (yes/no), active duty (yes/no), and education (≥4 years of college versus not). Race was categorized as White versus not due to small sample sizes in other categories. The substantive conclusions stayed the same with the added covariates, although the estimated differences between MWI± and MWI− groups were attenuated for the mental health outcomes. We are presenting the results from the fully adjusted models. A Bonferroni correction (α = 0.007) was used to correct for multiple comparisons. The Bonferroni correction was applied to the seven regression models used to estimate adjusted differences between groups (alpha = 0.05/7 = 0.007). Standardized mean differences are presented as effect sizes for both unadjusted and adjusted comparisons of the two groups. 34 A sensitivity analysis was performed that treated making weight as a continuous variable (number of behaviors endorsed).
Sociodemographic, Military Service, and Weight-Related Characteristics of the Overall Sample and by Engagement in Making Weight Behaviors (MWI+ [Yes] versus MWI− [No])
Data presented as N (%) for categorical variables and M (SD) for continuous variables.
MWI, Making Weight Inventory; MWI+, engaged in making weight behaviors; MWI−, did not engage in making weight behaviors; SMD, standardized mean differences between MWI+ and MWI− groups. Results are from chi-square tests for categorical variables and t tests for continuous variables.
Results
Sociodemographic, military service, and weight-related characteristics
The sample consisted of an approximately equal number of male and female participants. Participants who served in the Army were most represented over other military branches. Just under two-thirds were Veterans and the remainder were ADSMs. Mean age was 43.9 years, and average BMI was 28.9 kg/m2. Most participants identified as White, 83.79% followed by 9.84% Black or African American (Table 1).
Preliminary analysis of the data
The distribution of some outcomes was skewed (e.g., the binge eating variable and the food addiction variable). T tests and linear regressions give valid results even if the distribution of the outcome is not normal as long as the sample size is large. 35 The large sample size in the present study allowed us to utilize these methods with untransformed data, making the results easier to interpret.
Making weight behaviors
Overall, 41% of the sample engaged in at least one of the six identified making weight behaviors during their military service. The most endorsed making weight behavior was excessive exercise (35.7%) followed by fasting/skipping meals (26.3%), use of sauna/rubber suit (17.8%), use of laxatives (12.9%), diuretics (10.1%), and then vomiting (4.7%; Fig. 1). Those who engaged in making weight behaviors during military service had higher rates of identifying as female, White, Hispanic, less educated, currently active duty, and obesity and had a higher BMI (Table 1). Results of unadjusted bivariate analyses showed MWI+ had higher scores of dietary restraint, emotional eating, symptoms of food addiction, and symptoms of binge eating. Lastly, the MWI+ group demonstrated higher scores of depressive, anxiety, and PTSD symptomology (Table 2).
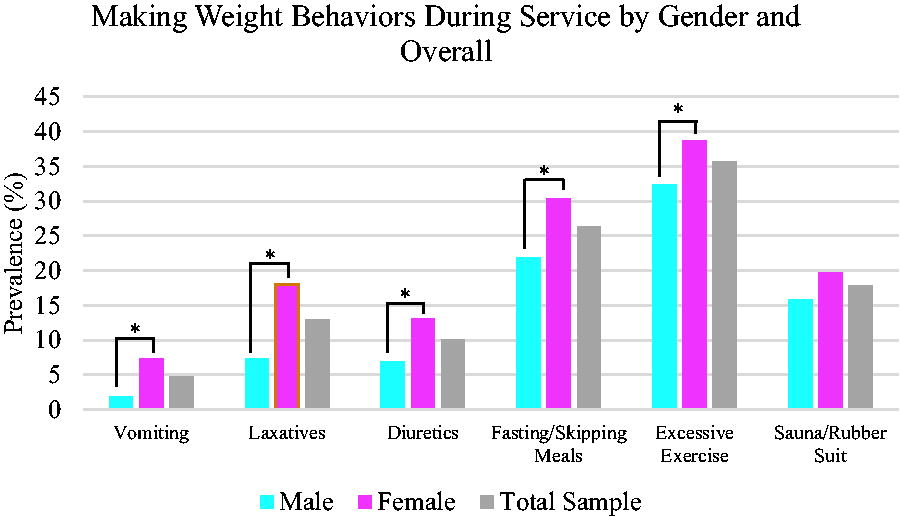
Percentage of making weight behaviors during active duty military service of the overall sample and by gender. Note. * = p < .05.
Eating Pathology and Mental Health Characteristics of the Overall Sample and by Engagement in Making Weight Behaviors (MWI+ [Yes] versus MWI− [No])
Results are from t-tests.
MWI, Making Weight Inventory; MWI+, engaged in making weight behaviors; MWI−, did not engage in making weight behaviors; difference = mean differences between MWI+ and MWI− groups; SMD, standardized mean differences between MWI+ and MWI− groups; EDE-Q7, Eating Disorder Examination Questionnaire Short Form Version; YEOQ, Yale Emotional Overeating Questionnaire; mYFAS, Modified Yale Food Addiction Scale; EDDS-5, Eating Disorder Diagnostic Scale; PHQ-8, Patient Health Questionnaire-8; GAD-7, Generalized Anxiety Disorder-7; PTSD, posttraumatic stress disorder; PCL-M, PTSD Checklist-Military.
Gender differences
Chi-square tests used to determine whether the proportion of making weight behaviors was different between genders indicated there were significant gender differences for all making weight behaviors (p’s < 0.05) other than wearing a sauna/rubber suit (p = 0.09). A greater proportion of female participants than males endorsed these behaviors. Also, more women engaged with at least one of the six making weight behaviors (p < 0.0001).
Eating pathology differences
Results of adjusted multiple linear regressions showed that those with MWI+ had higher scores of dietary restraint (by 0.89 [95% confidence interval [CI]: 0.50 to 1.28], p < 0.0001), emotional eating (by 0.44 [99.3% CI: 0.28 to 0.60], p < 0.0001), food addiction (by 0.47 [99.3% CI: 0.22 to 0.71], p < 0.0001), and binge eating (by 3.63 [99.3% CI: 1.25 to 6.01], p < 0.001) than those with MWI−.
Mental health differences
The multiple linear regressions used to test if making weight behavior significantly predicted mental health indicated that, after controlling for covariates, those with MWI+ had higher scores of depression (by = 1.38 [99.3% CI: 0.32 to 2.45], p < 0.0001), anxiety (by = 1.76 [99.3% CI: 0.73 to 2.79] p < 0.0001), and PTSD symptomatology scores (by = 5.07 [99.3% CI: 2.12 to 8.01], p < .0001) than those with MWI− (Table 3).
Adjusted Differences in Eating Pathology and Mental Health Mean Scores Between Making Weight Behavior Groups (MWI+ [Yes] versus MWI− [No])
Results are from regression models adjusted for age, gender, BMI, White race, Hispanic, active duty, and education. Bonferroni correction (α = 0.007) was used to correct for multiple comparisons.
CI, confidence interval; LL, lower limit; UL, upper limit; MWI, Making Weight Inventory; SMD, standardized mean differences between MWI+ and MWI− groups; MWI+, engaged in making weight behaviors; MWI−, did not engage in making weight behaviors; EDE-Q7, Eating Disorder Examination Questionnaire Short Form Version; YEOQ, Yale Emotional Overeating Questionnaire; mYFAS, Modified Yale Food Addiction Scale; EDDS-5, Eating Disorder Diagnostic Scale; PHQ-8, Patient Health Questionnaire-8; GAD-7, Generalized Anxiety Disorder-7; PTSD, posttraumatic stress disorder; PCL-M, PTSD Checklist-Military.
Sensitivity analysis
We examined making weight behavior a dichotomous variable rather than continuous to facilitate comparison with the only other study that has examined this. 8 To substantiate findings, analyses were conducted using MWI as a continuous variable as well, and substantive conclusions remained unchanged (not shown).
Discussion
The current study is the first to examine gender differences in making weight behaviors in an exclusively OEF/OIF/OND Veteran population. This was a critical population for the aims of this study given that the number of female Veterans and ADSMs and the prevalence of having overweight and obesity are greater in this service era than previous ones. 36 Using a dataset specifically designed to examine potential gender differences in health and health care, we were able to demonstrate gender differences in making weight behaviors in this military population. This study also aimed to investigate associations between making weight behaviors and obesity, eating pathology, and mental health characteristics later in life. Results confirmed hypotheses, more female Veterans reported a history of making weight behaviors overall and specifically with five of the six behaviors when compared with male Veterans. In addition, among all participants, regardless of gender, those who endorsed making weight behaviors had higher weight measurements and scores on measures of current eating pathology and mental health than those who did not endorse those behaviors.
Veterans endorsed a range of making weight behaviors in this study, with the most common being excessive exercise, reported by more than one-third of the sample, followed by fasting or skipping meals, which was endorsed by over one-quarter of the sample. Excessive exercise and fasting may actually be behaviors encouraged in military settings and, therefore, difficult to detect. It is important to note, however, that a high proportion of Veterans also endorsed engaging in disordered eating behaviors, such as vomiting and laxative and diuretic use, that are more commonly associated with eating disorders in adolescents. 8 We were not able to ascertain in this study whether some Veterans may have entered military life with a preexisting eating disorder and continued these disordered eating behaviors once in service.
The results of the current study align with previous findings that significantly more Veterans who are classified as having overweight/obesity engaged in at least one making weight behavior during service. 8 These behaviors may be motivated by service members aiming to avoid repercussions of not meeting weight standards, being subject to the “tape test” and the impact of military culture on beliefs on eating and weight. 14 Ironically, Veterans queried about the “tape test” do not believe it is an accurate measure of body composition, further complicating the appraisal of health and wellness standards. 11 The current study extends previous qualitative findings that suggest meeting military weight standards serves as a risk factor for eating pathology in women Veterans, 17 and that making weight behaviors such as diet pill and laxative use increases risk of eating disorder diagnosis in female civilians. 16
Furthermore, this work extends previous findings of an association between military making weight behaviors and later life obesity. 8 Results show that Veterans who engaged in at least one making weight behavior during time of service had a greater proportion of having a BMI in the overweight or obese range. This study replicates earlier findings that demonstrated that Veterans who engaged in making weight behaviors during service had a greater proportion of engaging in current pathological eating behaviors, most notably binge eating. 8 Moreover, the current study found that those who engaged in at least one making weight behavior during service had a greater proportion of reporting significantly higher levels of current dietary restraint, emotional eating, food addiction, and binge eating. Previous qualitative work has supported that disordered eating behaviors have been cited as a method to manage stress while in service, 17 and our findings suggest that this coping strategy may extend beyond military service.
Lastly, findings confirm that those who engaged in making weight behaviors endorsed more psychological distress on measures of mental health. Research has supported that, particularly in female Veterans, mental health comorbidities are positively associated with eating disorder status. 18 This finding is extremely important given the rate of mental health pathology among Veteran populations is higher than the national average. 18 Moreover, those Veterans with obesity present with higher rates of mental health disorders and may have experienced the most pressure to lose weight to make military weight standards. 36 Given that making weight behaviors such as excessive exercise and restrictive eating often predict eating disorders generally in the civilian population, these findings highlight the strength of that association in a Veteran population given their increased risk. 16
The current study demonstrates a significant strength in utilizing a sample with an even proportion of male to female Veterans, and measuring making weight behaviors with an internally consistent, and previously established measure. This has allowed for the current study to add to the current literature base by demonstrating gender differences in making weight behaviors. A few limitations should be considered as findings may have been influenced by recall and self-report biases. There are also limitations on generalizability of findings given this sample consists of predominately White, non-Hispanic Veterans. The survey used in this study did not include information on length of service, MOS, or rank, which is a limitation and opportunity for future research. Furthermore, this study uses correlational data and is limited in that we can only comment on associations and not infer that making weight behavior in the military caused eating pathology or mental health pathology later in life. Higher weight during the military may have contributed to the likelihood of engaging in making weight behaviors and thus served as a confound. The weight during the military was not collected, but we adjusted the analyses looking at the relationship between engagement in making weight behaviors and eating pathology/mental health for current BMI. Our findings also do not take into account that participants may have engaged in making weight behaviors prior to service. Given the correlational study design, we cannot ascertain from these findings whether military making weight behaviors caused later life mental health conditions. Due to participant survey burden, there were other potential making weight behaviors, such as fluid restriction or extreme dieting behaviors, that we were unable to assess. Finally, there may be other making weight behaviors, currently unknown to the investigators, that were not examined in this work.
There are critical clinical implications of our findings, most importantly for women Veterans. Failure to make weight at weigh-ins carries significant consequences for military personnel including additional training burdens, stigmatizing measurements, and potential demotion or even separation from service. Thus, the higher rate of making weight behaviors in women Veterans compared with men, coupled with its sequelae, particularly high weight, may be further compounding gender differences in career advancement and salary during and beyond military service. There is evidence that obesity during active duty is linked to lower career advancement opportunities and lower salaries. 12 This is considered in tandem with other documented reasons, such as pregnancy and military sexual assault, that result in women leaving the military sooner than men.37 This is largely due to promotions, as reenlistment and deployment are in part determined by ability to meet weight and body composition tests. 12,13
This study extends what we currently know about making weight behaviors during military service and the potential long-lasting impact on gender differences in career advancement and implications for long-term physical and mental health. In recognition of the limitations of utilizing measures such as BMI as a proxy for health and fitness, the Department of Defense (DoD) has recently added the use of physical fitness tests when limitations on body composition measurements are exceeded. 38 While, at the individual level, this practice remains problematic, at the population level the DoD is balancing the impact that high rates of obesity and overweight have on medical morbidity and thus potential readiness for mission. Data from this study are essential for providing the DOD with information related to military weight and fitness evaluations and to the Veterans Health Administration (VHA) for downstream health care utilization.
Prevention is essential, and more work is needed for how to address disordered eating and making weight behaviors that support the health and careers of service members without threat or fear of demotion and separation or being subjected to weight stigma and body shaming. An approach that encompasses enhanced screening of making weight behaviors, availability of interventions to address these behaviors, and assessing current DoD programs that focus on obesity and fitness testing to ensure they do not exacerbate problem behaviors seems warranted. A strong partnership between the DOD and VHA may be beneficial in translating current findings to improve methods for measuring military fitness standards during active-duty service.
Conclusion
In summary, this study examined the relationship between making weight behaviors during military service and gender, obesity, eating, and mental health outcomes later in life among U.S. Iraq and Afghanistan war Veterans. The results of the current study offer the first empirical investigation of gender differences in making weight behaviors. These findings are critical, as the impact of making weight behaviors is an often-overlooked area of health for women Veterans as well as for Veterans overall. Failure to make weight carries significant consequences for military personnel such as additional training burdens, stigma, and possible demotion or even separation from the service. Female service members engage in higher rates of making weight behaviors which may have implications for gender differences in military and postmilitary career advancement and salary. This area of research has potential policy implications in that it demonstrates the necessity for improved methods for measuring military fitness standards during active-duty service that are not stigmatizing and do not result in harmful career and health consequences. More efficient screening and treatment for disordered eating during service have potential to decrease later health care utilization and treatment cost for mental health and obesity-related disorders later in life for Veterans. This research is consistent with the VHA’s commitment to improving health care for women Veterans.
Footnotes
Authors’ Contributions
All authors contributed significant intellectual content to the overall article, participated in revisions, and have seen and approved of the final article. A.C.: Visualization, writing—original draft, and writing—review and editing. K.H.N.: Visualization, writing—original draft, and writing—review and editing. E.B.: Formal analysis, visualization, and writing—review and editing. L.F.: Visualization and writing—review and editing. C.R.: Formal analysis and writing—review and editing. J.S.: Visualization and writing—review and editing. S.H.: Funding acquisition and writing—review and editing. R.M.: Conceptualization, formal analysis, supervision, and writing—review and editing.
Ethics Approval Statement
Institutional Review Board approval was obtained from all sites of this study.
Author Disclosure Statement
The authors declare that there is no conflict of interest in the material presented. The authors also declare no financial disclosures.
Funding Information
The content of this research is solely the responsibility of the authors and does not necessarily represent the official views of the VA or the Veterans Health Administration. Study sponsors had no role in study design; collection, analysis, and interpretation of data; writing of the report; nor the decision to submit the report for publication. This project was supported in part by the Veterans Affairs Health Services Research and Development (CIN 13–407) (HSR&D), Center of Innovation (COIN) Pain Research, Informatics, Multi-morbidities, and Education (PRIME) Center, West Haven, CT. The Women Veterans Cohort Study (WVCS) was supported by the Department of Veterans Affairs, Veterans Health Administration, HSR&D project (IIR-12–118). This project was also supported in part by HSR&D project (IIR-15–349), Weight Loss Treatment, and CBT for Veterans with Binge Eating and HSR&D project.