
Abstract
Background:
We aimed to estimate contraceptive claims prevalence among reproductive-aged women with selected autoimmune diseases compared with those without these conditions in 2019.
Materials and Methods:
Using IBM MarketScan Commercial Claims and Encounters and Multistate Medicaid databases, we analyzed permanent and prescription contraception claims prevalence among women aged 15–49 years with inflammatory bowel disease (IBD), multiple sclerosis (MS), rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and among women with these autoimmune diseases using selected fetotoxic medications. We calculated adjusted prevalence ratios (aPR) and 95% confidence intervals (CIs) using Poisson regression.
Results:
In 2019, most (60–75%) insured women with selected autoimmune diseases did not have contraception claims. Among commercially insured women, those with SLE were less likely to have claims for any method assessed (aPR = 0.90, 95% CI: 0.86–0.95), less likely to have combined hormonal contraceptives (CHC) claims (aPR = 0.65, 95% CI: 0.60–0.70), and more likely to have long-acting reversible contraceptives (LARC) claims (aPR = 1.14, 95% CI: 1.05–1.23) than women without selected autoimmune diseases. Among Medicaid-insured women, those with IBD, MS, RA, and SLE were more likely to have claims for any method assessed (aPR = 1.23–1.31) and LARC (aPR = 1.23–1.47) than women without selected autoimmune diseases. Women with SLE with lupus nephritis were less likely to have CHC claims (aPR = 0.56, 95% CI: 0.35–0.89) than females without selected autoimmune diseases. Among those using selected fetotoxic medications, 70.4% of commercially insured women and 72.2% of Medicaid-insured women did not have contraceptive claims in 2019.
Conclusions:
Less than half of the insured women with selected autoimmune diseases had permanent or prescription contraception claims in 2019.
Introduction
Autoimmune diseases have an estimated prevalence of 5% in the U.S. population, and many autoimmune diseases disproportionately affect women. 1 Autoimmune diseases such as inflammatory bowel disease (IBD), including Crohn’s disease and ulcerative colitis, multiple sclerosis (MS), rheumatoid arthritis (RA), and systematic lupus erythematosus (SLE), are commonly diagnosed during the reproductive years and are associated with adverse pregnancy and perinatal outcomes, including maternal and fetal morbidity and mortality.2–4 Additionally, some immunosuppressive medications (e.g., methotrexate, mycophenolate mofetil) are fetotoxic or might affect the effectiveness of certain contraceptives.2,5 As a result, reproductive health issues, including contraception, are important to women with autoimmune diseases. Health care providers who manage patients with these conditions can support their patients’ reproductive goals. However, some health care providers may be hesitant to provide contraception due to concerns or lack of knowledge about the safety of various contraceptive methods for women with autoimmune diseases. 6
Several national organizations have published guidelines or statements on the safe use of contraception for women with autoimmune diseases. The U.S. Medical Eligibility Criteria for Contraceptive Use (MEC) provides evidence-based recommendations for the safe use of contraception for patients with certain characteristics or medical conditions. 7 In general, women with autoimmune diseases may safely use both hormonal and nonhormonal contraceptive methods (Fig. 1). However, health and safety issues do arise in these populations, especially regarding risk of venous thromboembolism (VTE) with certain autoimmune diseases and combined hormonal contraception (CHC) (i.e., estrogen-containing pill, patch, and ring) or risk of bone loss with prolonged immobility or corticosteroid use and certain contraceptives. 7 The American College of Rheumatology has released evidence-based recommendations for the management of a broad range of reproductive health topics, including contraception, for patients with rheumatic and musculoskeletal diseases, 2 and the American Gastroenterological Association encourages family planning counseling, including contraception, for IBD patients in its Pregnancy Clinical Care Pathway. 8
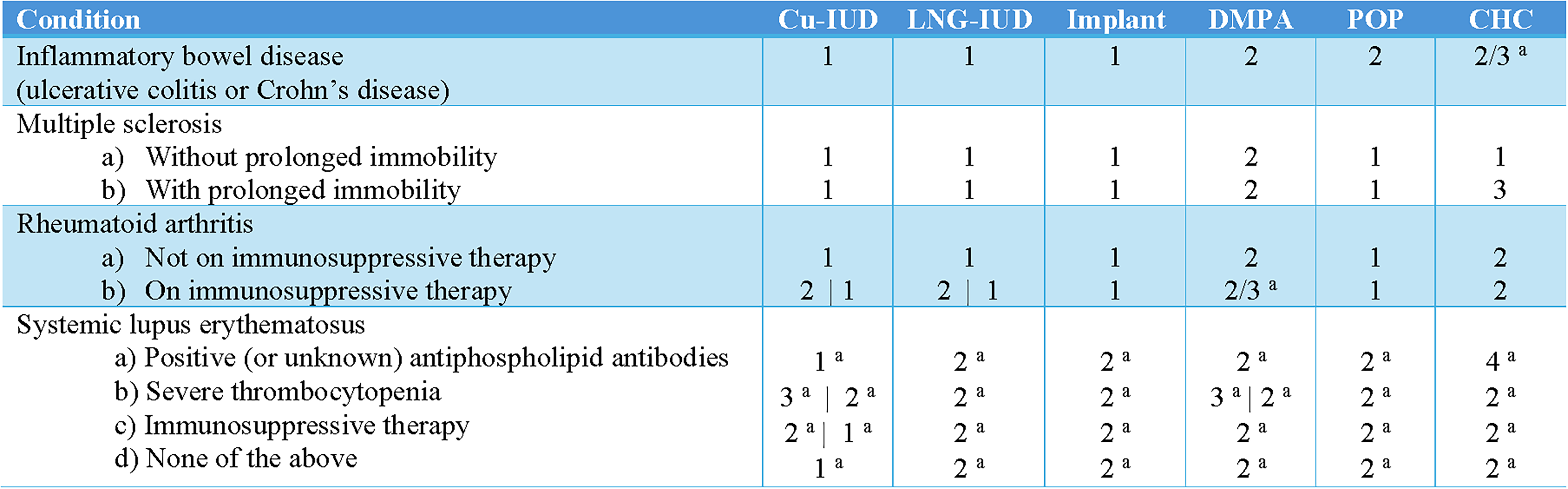
Summary of U.S. MEC 2024 recommendations for selected autoimmune diseases. CHC, combined hormonal contraception (combined oral contraception, contraceptive patch, vaginal ring); Cu-IUD, copper intrauterine device; DMPA, depot-medroxyprogesterone acetate; LNG-IUD, levonorgestrel intrauterine device; POP, progestin-only pill; U.S. MEC, United States Medical Eligibility Criteria for Contraceptive Use. 1—No restriction (method can be used); 2—advantages generally outweigh theoretical or proven risks; 3—theoretical or proven risks usually outweigh the advantages; and 4—unacceptable health risk (method not to be used). aPlease see the complete guidance for a clarification of this classification: https://www.cdc.gov/contraception/hcp/contraceptive-guidance/index.html. Adapted with permission from Nguyen et al. 7
The objective of this analysis is to describe contraceptive claims prevalence among women aged 15–49 years with selected autoimmune diseases (IBD, MS, RA, and SLE), compared with those without these conditions, in the year 2019. We also assessed contraceptive claims prevalence among specific subgroups: SLE with antiphospholipid antibody syndrome (APS), SLE with lupus nephritis, and women with any of the selected autoimmune diseases who were using one or more selected fetotoxic medications. We selected these conditions because they disproportionately affect reproductive-age women and are associated with increased risk for adverse events during pregnancy or with the use of fetotoxic medications.2–4
Materials and Methods
We used the IBM Watson Health MarketScan® Commercial Claims and Encounters Database and the Multistate Medicaid Database (MarketScan) to conduct this study. 9 The Commercial Database includes data from employees and their spouses or dependents covered by employer-sponsored private health insurance. The Multistate Medicaid Database includes data from Medicaid enrollees from 9 to 12 states. 9 Both databases include information on paid claims for pharmaceuticals, inpatient and outpatient medical services and procedures, and select demographic information. Claims included in the MarketScan databases are fully paid and adjudicated; using fully paid claims improves the reliability and accuracy of the data. 10 Because MarketScan data are deidentified, the institution did not consider this analysis to be human subjects research, and institutional review board review was not required.
We included women who were aged 15–49 years in 2019, had prescription drug coverage included in the database in 2019, and were enrolled for ≥11 months per year annually during 2016–2019. We excluded women with International Classification of Disease, 10th revision (ICD-10) diagnosis or procedure codes or other procedure/supply codes for hysterectomy (2016–2019) and pregnancy (at any point in 2019) (Supplementary Appendix A1).
We identified women with selected autoimmune diseases, including IBD, MS, RA, and SLE, using ICD-10 codes from inpatient and outpatient claims (2016–2019). We included women with at least one inpatient claim or two or more outpatient claims at least 30 days apart for each of the selected autoimmune diseases or subgroups (Supplementary Appendix A2). 11 We performed all analyses with women without any of the selected autoimmune diseases as a reference group. Among women with and without selected autoimmune diseases, we identified prescription claims for the following fetotoxic medications: cladribine, cyclophosphamide, fingolimod, leflunomide, methotrexate, mitoxantrone hydrochloride, mycophenolate mofetil, and teriflunomide. We initially identified target fetotoxic medications from two publications12,13 and refined this list to include commonly used medications with significant teratogenicity or abortifacient risk to the patient should they become pregnant (Supplementary Appendix A3). We categorized women with at least one prescription for any of the selected fetotoxic medications in 2019 as using fetotoxic medications.
We identified prescription contraception (i.e., injectable, oral contraception [combined oral contraception, COC, and progestin-only pill, POP], contraceptive patch, or vaginal ring) claims during the index year of 2019 or long-acting reversible contraceptive (LARC) and permanent contraception procedure claims from 2016 to 2019 using diagnostic, procedure, drug, and supply codes adapted from the Office of Population Affairs (Supplementary Appendix A4). 14 Contraceptive claims, including those for procedures and prescriptions filled, served as proxies for contraceptive use. Categorization of contraceptive method claims in the index year followed a previously established algorithm (Fig. 2). 15 Briefly, we first queried eligible women for permanent contraception codes from 2016 to 2019. Then, we queried for LARC codes from 2016 to 2019. We chose a 3-year period based on a previous sensitivity analysis performed by our team. 16 We then queried for remaining methods among women with LARC removal codes and all other women not yet classified. We classified women as using a short-acting reversible contraceptive (injectable, oral contraception, patch, ring) method in 2019 if there were any claims during that year, independent of duration of use. If we identified claims for multiple short-acting methods in the index year, that individual was classified as using the method associated with the most recent claim. We categorized COC, contraceptive patch, and vaginal ring as CHC in all analyses. We categorized oral contraceptives not specified as COC or POP as unknown oral contraceptives. We characterized women without any of the contraceptive claims as using neither permanent nor prescription contraception (these women may have been relying on other methods of contraception, such as condoms or partner’s vasectomy).
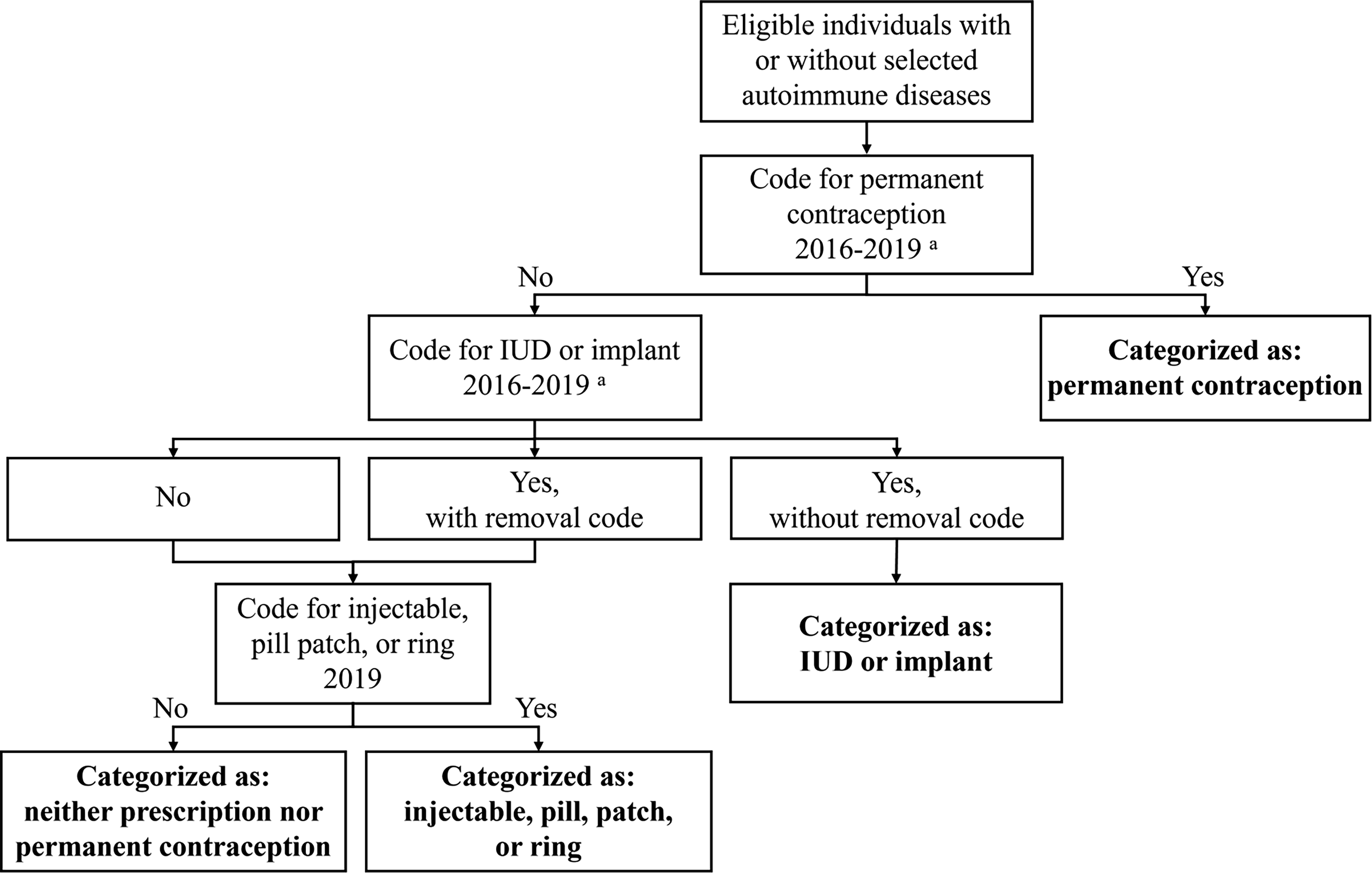
Algorithm for categorization of contraceptive method. IUD, intrauterine device. aThis duration was chosen based on a previous sensitivity analysis that only found an additional 1% permanent contraception users and an additional 1% IUD insertions with 7 years of claims data compared with 3 years. 16
We described the analytic population overall and by the presence or absence of selected autoimmune diseases separately for the commercial and Medicaid datasets. Because of the differences between the two datasets, we could not analyze the prevalence of contraception claims between datasets. We assessed the percent distributions of demographic characteristics and other covariates, including age (15–19, 20–34, and 35–49 years), geographic region (Northeast, North Central, South, West, unknown; only available in the commercial dataset), race/ethnicity (Black, Hispanic, Other, White, unknown; only available in the Medicaid dataset), and fetotoxic medications (yes or no). We estimated contraceptive claims prevalence for each contraceptive method by each selected autoimmune disease (IBD, MS, RA, or SLE [with subgroups SLE with APS or SLE with lupus nephritis]), by any of the selected autoimmune diseases (IBD, MS, RA, and SLE combined), and stratified by selected fetotoxic medication use among all women with selected autoimmune diseases. We estimated adjusted prevalence ratios (aPRs) and 95% confidence intervals (CIs) using Poisson regression to measure the association between autoimmune disease and contraceptive claims prevalence, adjusted for age (both commercial and Medicaid datasets) and race/ethnicity (Medicaid dataset). 17 For multivariable models, we considered contraceptive type as the response variable and autoimmune disease as a multilevel categorical explanatory variable. For all aPRs, the reference group was women without selected autoimmune diseases. A small proportion of women without selected autoimmune diseases had claims for selected fetotoxic medications (0.3% in both datasets); women without selected autoimmune diseases using selected fetotoxic medications were included in the reference group of women without selected autoimmune diseases for all analyses. We used four models to examine contraceptive claims prevalence by type: any permanent or prescription contraception, permanent contraception, LARC, and CHC. Sample sizes for injectables and POPs were too small for modeling. We could not classify a small proportion of oral contraceptive claims (0.2% and 0.3% of analytic samples for commercial and Medicaid insurance, respectively) as COC or POP; we included these in aPR calculations for any permanent or prescription contraception use, but not for the CHC model. We performed all analyses with applications of the GENMOD procedure in SAS (version 9.4).
Results
Commercial insurance
Among 1,836,492 eligible women with commercial insurance, we identified 34,033 (1.9%) women as having one or more of the selected autoimmune diseases (Fig. 3). Of these, 11,050 (32.5%) had IBD alone, 5,908 (17.4%) had MS alone, 9,977 (29.3%) had RA alone, 5,435 (16.0%) had SLE alone, and 1,663 (4.9%) had more than one selected autoimmune disease. Among women with SLE, 83 (1.5%) had both APS and lupus nephritis, 256 (4.7%) had APS alone, 628 (11.6%) had lupus nephritis alone, and 4,468 (82.2%) had neither APS nor lupus nephritis. Across all groups, most women were aged 35–49 years or resided in the southern United States (Table 1). Women with RA had the highest proportion of selected fetotoxic medication claims (51.1%) followed by females with multiple selected autoimmune diseases (48.2%).
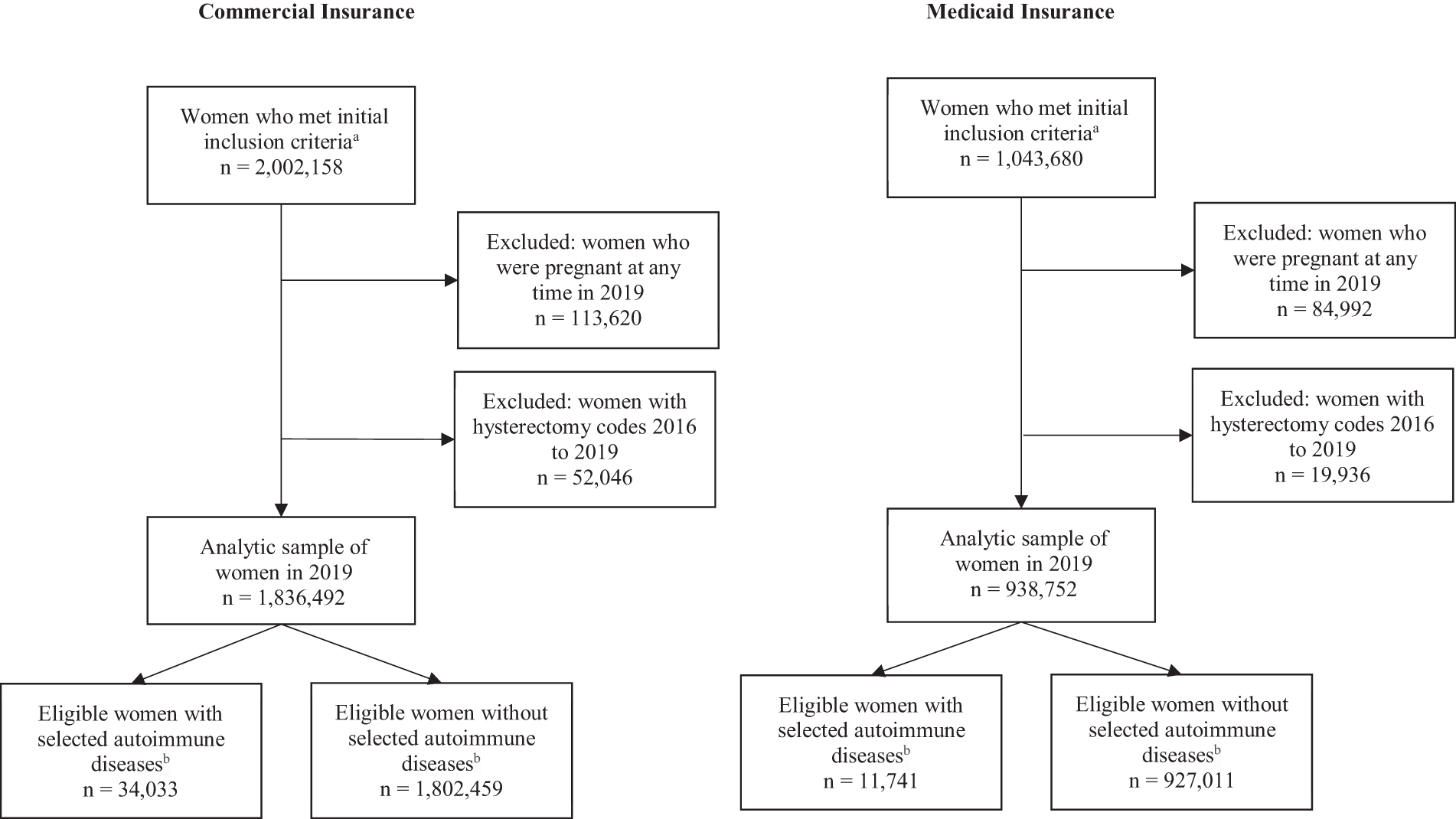
Sample selection for eligible U.S. women aged 15–49 years with commercial insurance or Medicaid, with and without selected autoimmune diseases. aWomen who were ages 15–49 years in 2019, had prescription drug coverage included in the database in 2019, and were enrolled for ≥11 months per year annually during 2016–2019. The commercial insurance dataset included 7,162,800 women ages 15–49 years, from which 5,085,530 (71.0%) were excluded for not being enrolled for ≥11 months per year annually during 2016–2019, and 75,112 (1.1%) were excluded for lack of prescription drug coverage in 2019, leaving 2,002,158 (28.0%) women who met the initial inclusion criteria. The Medicaid insurance dataset included 3,445,808 women ages 15–49 years, from which 2,283,097 (66.3%) were excluded for not being enrolled for ≥11 months per year annually during 2016–2019, and 119,031 (3.5%) were excluded for lack of prescription drug coverage in 2019, leaving 1,043,680 (30.3%) women who met the initial inclusion criteria. bIncluding inflammatory bowel disease (i.e., Crohn’s disease, ulcerative colitis), multiple sclerosis, rheumatoid arthritis, and systemic lupus erythematosus.
Sample Characteristics of U.S. Women Aged 15–49 Years with Commercial or Medicaid Insurance, with and without Selected Autoimmune Diseases, 2019
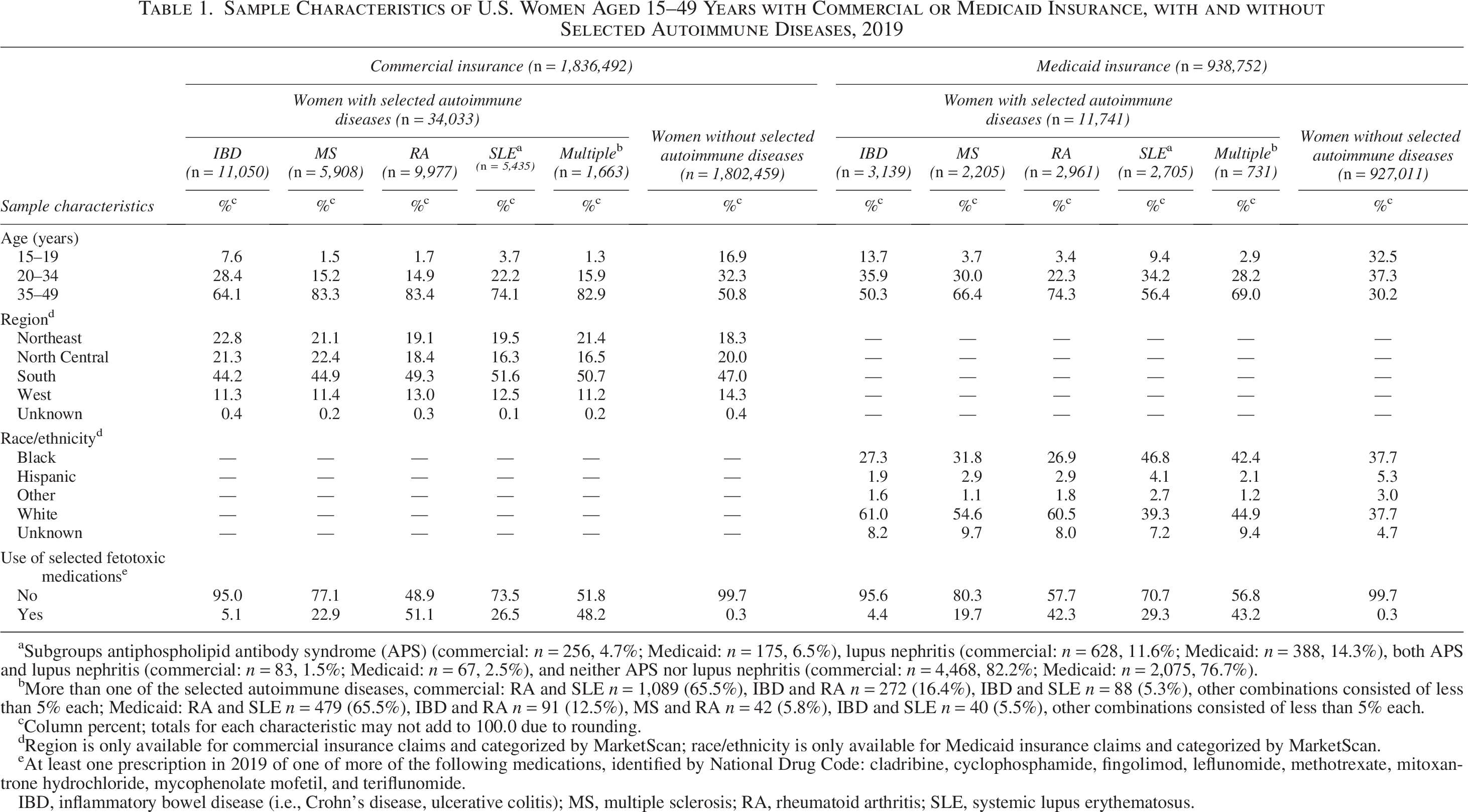
Subgroups antiphospholipid antibody syndrome (APS) (commercial: n = 256, 4.7%; Medicaid: n = 175, 6.5%), lupus nephritis (commercial: n = 628, 11.6%; Medicaid: n = 388, 14.3%), both APS and lupus nephritis (commercial: n = 83, 1.5%; Medicaid: n = 67, 2.5%), and neither APS nor lupus nephritis (commercial: n = 4,468, 82.2%; Medicaid: n = 2,075, 76.7%).
More than one of the selected autoimmune diseases, commercial: RA and SLE n = 1,089 (65.5%), IBD and RA n = 272 (16.4%), IBD and SLE n = 88 (5.3%), other combinations consisted of less than 5% each; Medicaid: RA and SLE n = 479 (65.5%), IBD and RA n = 91 (12.5%), MS and RA n = 42 (5.8%), IBD and SLE n = 40 (5.5%), other combinations consisted of less than 5% each.
Column percent; totals for each characteristic may not add to 100.0 due to rounding.
Region is only available for commercial insurance claims and categorized by MarketScan; race/ethnicity is only available for Medicaid insurance claims and categorized by MarketScan.
At least one prescription in 2019 of one of more of the following medications, identified by National Drug Code: cladribine, cyclophosphamide, fingolimod, leflunomide, methotrexate, mitoxantrone hydrochloride, mycophenolate mofetil, and teriflunomide.
IBD, inflammatory bowel disease (i.e., Crohn’s disease, ulcerative colitis); MS, multiple sclerosis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
In 2019, most women with and without selected autoimmune diseases did not have claims for permanent or prescription contraception (range: 61.7–74.1%) (Table 2). For women with IBD, MS, RA, and SLE and women without selected autoimmune diseases, the most common contraceptive claim was CHCs (range: 12.0–24.0%) followed by intrauterine devices (IUDs) (range: 7.5–9.1%). Other contraceptive methods accounted for ≤2.0% of the method claims mix among all selected autoimmune disease groups and those without selected autoimmune diseases. Among women with SLE with APS or SLE with lupus nephritis, IUDs were most common (range 11.0–14.5%). When stratified by selected fetotoxic medications, more women with any of the selected autoimmune diseases with selected fetotoxic medications did not have permanent or prescription contraceptive claims in 2019 compared to those with any selected autoimmune diseases and no fetotoxic medications (70.4% and 67.6%, respectively).
Contraceptive Method Use Among U.S. Women Aged 15–49 Years with Commercial or Medicaid Insurance, with and Without Selected Autoimmune Diseases and by Selected Fetotoxic Medication Use, 2019
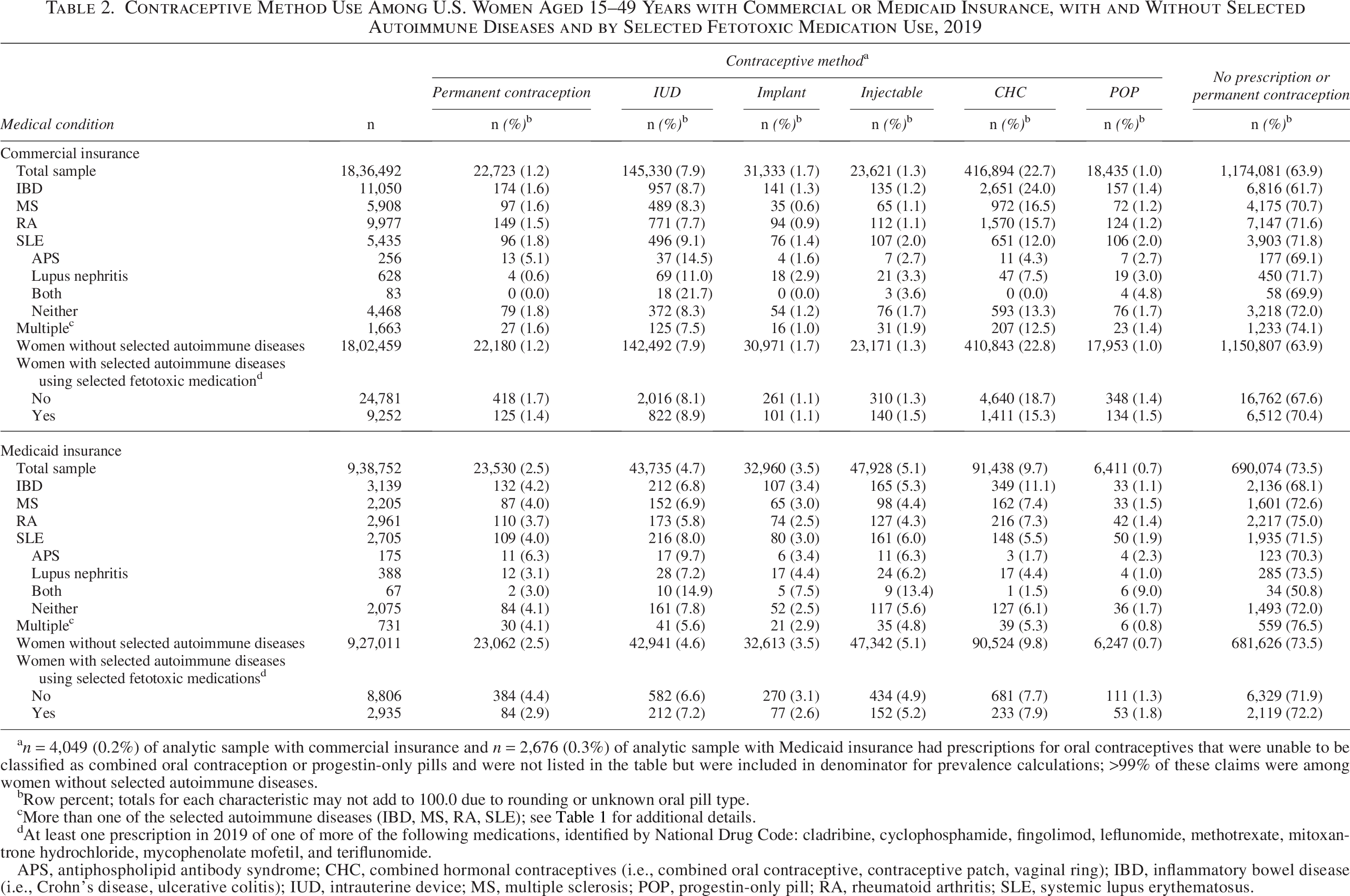
n = 4,049 (0.2%) of analytic sample with commercial insurance and n = 2,676 (0.3%) of analytic sample with Medicaid insurance had prescriptions for oral contraceptives that were unable to be classified as combined oral contraception or progestin-only pills and were not listed in the table but were included in denominator for prevalence calculations; >99% of these claims were among women without selected autoimmune diseases.
Row percent; totals for each characteristic may not add to 100.0 due to rounding or unknown oral pill type.
More than one of the selected autoimmune diseases (IBD, MS, RA, SLE); see Table 1 for additional details.
At least one prescription in 2019 of one of more of the following medications, identified by National Drug Code: cladribine, cyclophosphamide, fingolimod, leflunomide, methotrexate, mitoxantrone hydrochloride, mycophenolate mofetil, and teriflunomide.
APS, antiphospholipid antibody syndrome; CHC, combined hormonal contraceptives (i.e., combined oral contraceptive, contraceptive patch, vaginal ring); IBD, inflammatory bowel disease (i.e., Crohn’s disease, ulcerative colitis); IUD, intrauterine device; MS, multiple sclerosis; POP, progestin-only pill; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
When adjusted for age, women with IBD were more likely to have any permanent or prescription contraception claims (aPR = 1.14, 95% CI: 1.11–1.18) and more likely to have CHC claims (aPR = 1.18, 95% CI: 1.14–1.23) than those without selected autoimmune diseases (Table 3). Women with SLE were less likely to have any contraception claims (aPR = 0.90, 95% CI: 0.86–0.95) and less likely to have CHC claims (aPR = 0.65, 95% CI: 0.60–0.70); however, this group was more likely to have LARC claims (aPR = 1.14, 95% CI: 1.05–1.23). Women with SLE with APS were less likely to have any contraception claims (aPR = 0.90, 95% CI: 0.85–0.94), less likely to have CHC claims (aPR = 0.67, 95% CI: 0.62–0.72), and more likely to have LARC claims (aPR = 1.11, 95% CI: 1.02–1.21). Similarly, women with SLE with lupus nephritis were less likely to have any contraception claims (aPR = 0.80, 95% CI: 0.69–0.93), less likely to have CHC claims (aPR = 0.34, 95% CI: 0.26–0.46), and more likely to have LARC claims (aPR = 1.41, 95% CI: 1.14–1.74). We did not observe any statistically significant differences for permanent contraception claims across all groups analyzed; similarly, we did not observe any significant differences for any of the contraceptive method types among women with MS or RA. Women with any of the selected autoimmune diseases and selected fetotoxic medications were more likely to have LARC claims (aPR = 1.12, 95% CI: 1.05–1.20) and less likely to have CHC claims (aPR = 0.90, 95% CI: 0.86–0.95).
Adjusted Prevalence Ratios of Contraceptive Method Use Among U.S. Women with Commercial Insurance or Medicaid Aged 15–49 Years, by Selected Autoimmune Diseases and Subgroups, Compared with Women Without Any of the Selected Autoimmune Diseases, 2019
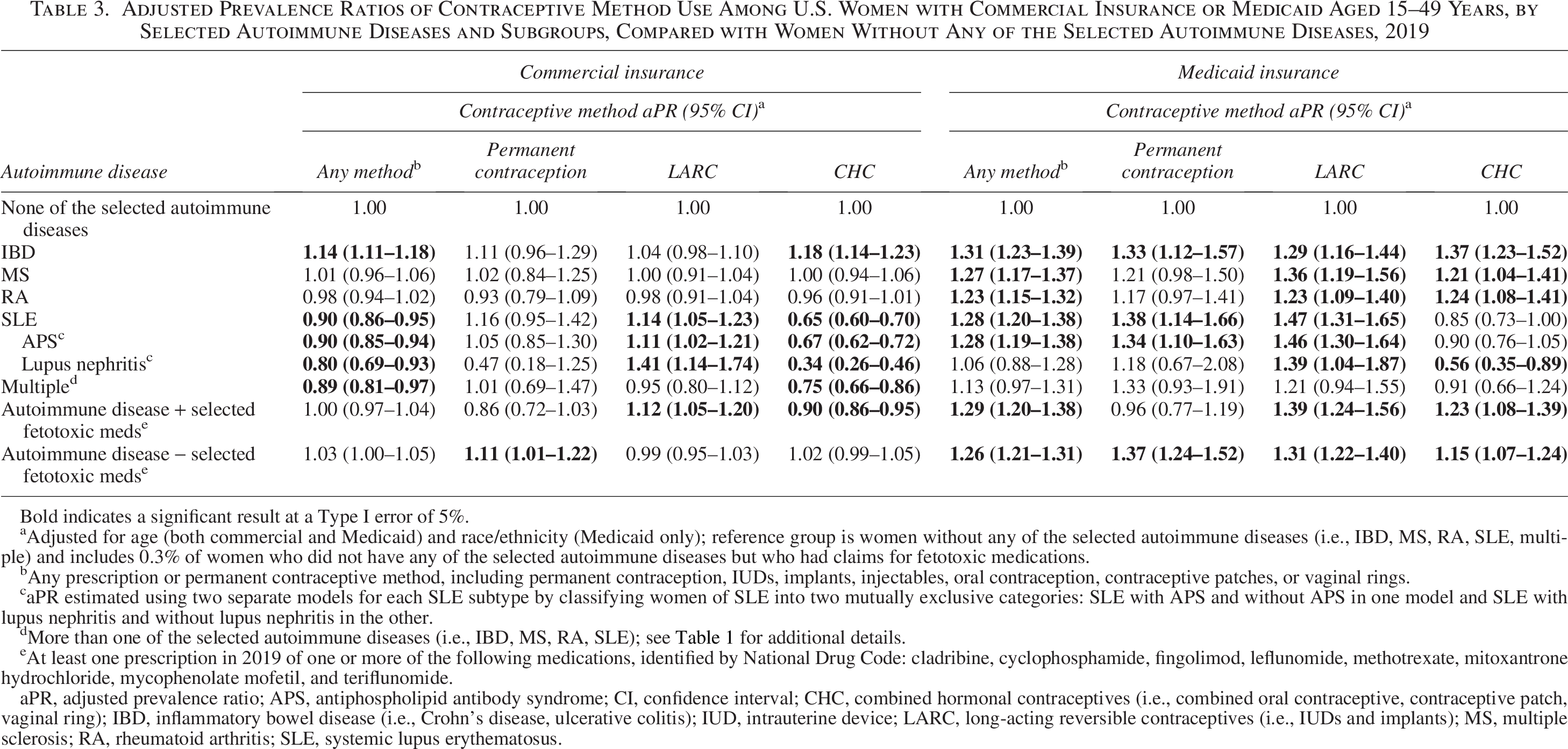
Bold indicates a significant result at a Type I error of 5%.
Adjusted for age (both commercial and Medicaid) and race/ethnicity (Medicaid only); reference group is women without any of the selected autoimmune diseases (i.e., IBD, MS, RA, SLE, multiple) and includes 0.3% of women who did not have any of the selected autoimmune diseases but who had claims for fetotoxic medications.
Any prescription or permanent contraceptive method, including permanent contraception, IUDs, implants, injectables, oral contraception, contraceptive patches, or vaginal rings.
aPR estimated using two separate models for each SLE subtype by classifying women of SLE into two mutually exclusive categories: SLE with APS and without APS in one model and SLE with lupus nephritis and without lupus nephritis in the other.
More than one of the selected autoimmune diseases (i.e., IBD, MS, RA, SLE); see Table 1 for additional details.
At least one prescription in 2019 of one or more of the following medications, identified by National Drug Code: cladribine, cyclophosphamide, fingolimod, leflunomide, methotrexate, mitoxantrone hydrochloride, mycophenolate mofetil, and teriflunomide.
aPR, adjusted prevalence ratio; APS, antiphospholipid antibody syndrome; CI, confidence interval; CHC, combined hormonal contraceptives (i.e., combined oral contraceptive, contraceptive patch, vaginal ring); IBD, inflammatory bowel disease (i.e., Crohn’s disease, ulcerative colitis); IUD, intrauterine device; LARC, long-acting reversible contraceptives (i.e., IUDs and implants); MS, multiple sclerosis; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
Medicaid insurance
Among 938,752 eligible Medicaid-insured women, we identified 11,741 (1.3%) women as having one or more of the selected autoimmune diseases (Table 1). Of these, 3,139 (26.7%) had IBD alone, 2,205 (18.8%) had MS alone, 2,961 (25.2%) had RA alone, 2,705 (23.0%) had SLE alone, and 731 (6.2%) had more than one selected autoimmune diseases. Among women with SLE, 67 (2.5%) had both APS and lupus nephritis, 175 (6.5%) had APS alone, 388 (14.3%) had lupus nephritis alone, and 2,075 (76.7%) had neither APS nor lupus nephritis. Most women with selected autoimmune diseases were aged 35–49 years. The highest proportion of women with SLE were Black, whereas the highest proportions of women with IBD, MS, and RA were White (Table 1). Women with multiple selected autoimmune diseases (43.2%) had the highest proportion of selected fetotoxic medication claims, followed by women with RA (42.3%).
In the Medicaid sample, most women with and without selected autoimmune diseases did not have permanent or prescription contraception claims in 2019 (range: 50.8–76.5%) (Table 2). CHCs were the most prevalent contraception claim among women with IBD, MS, and RA (range: 7.3–11.1%) followed by IUDs (range: 5.8–6.9%). Among women with SLE and SLE subgroups, IUDs were the most prevalent contraception claim (range: 7.2–9.7%), followed by injectables (range: 6.0–6.3%); CHC prevalence was lower (range: 1.7–5.5%). Among women with any of the selected autoimmune diseases and selected fetotoxic medications, 72.2% did not have permanent or prescription contraception claims, which was similar to those with selected autoimmune diseases without selected fetotoxic medications (71.9%).
When adjusted for age and race/ethnicity, women with IBD, MS, RA, SLE, and SLE with APS were more likely to have permanent or prescription contraception claims than those without selected autoimmune diseases (aPR = 1.23–1.31) (Table 3). Women with IBD, SLE, and SLE with APS were more likely to have permanent contraception claims (aPR = 1.33–1.38). Women with IBD, MS, RA, SLE, SLE with APS, and SLE with lupus nephritis were more likely to have LARC claims (aPR = 1.23–1.47). Women with IBD, MS, and RA were more likely to have CHC claims (aPR = 1.21–1.37); in contrast, women with SLE with lupus nephritis were less likely to have CHC claims (aPR = 0.56, 95% CI: 0.35–0.89). Women with selected autoimmune diseases and selected fetotoxic medications were more likely to have permanent or prescription contraception claims (aPR = 1.29, 95% CI: 1.20–1.38), LARC (aPR = 1.39, 95% CI: 1.24–1.56), and CHC claims (aPR = 1.23, 95% CI: 1.08–1.39).
Discussion
Understanding contraceptive use patterns of women with autoimmune diseases is important given the association of some autoimmune diseases with adverse pregnancy outcomes.2–4 In both commercial and Medicaid datasets, approximately 25–40% of women in each of the autoimmune disease groups assessed had claims for permanent or prescription contraception in 2019. These data are consistent with previous insurance claims analyses in which 20% of privately insured women with RA or SLE and approximately 30% of women with one of 22 autoimmune diseases used any prescription contraception.12,18 According to the 2017–2019 National Survey of Family Growth, approximately 65% of women aged 15–49 were using contraception; the most common contraceptive methods used were female sterilization (18.1%), oral contraception (14.0%), LARC (10.4%), and the male condom (8.4%). 19 Among our study population, there was a lower prevalence of any contraceptive method use and different method mix than in these national data; however, the current study does not explore reasons for contraceptive use or nonuse in this population. For women with autoimmune diseases who wish to prevent or time pregnancy, it is important to ensure access to contraceptive methods that are safe based on their medical conditions. Several professional organizations recommend or encourage discussion about contraception and pregnancy planning for reproductive-aged patients with autoimmune diseases or who take fetotoxic medications.2,8,20
According to U.S. MEC and American College of Rheumatology guidance, women with SLE and positive antiphospholipid antibodies should avoid CHC due to VTE risk, but can safely use other hormonal contraceptives such as the hormonal IUD.2,7 In our analysis, we found that women with SLE, including those with APS, were less likely to have CHC prescription claims than women without selected autoimmune diseases, which is consistent with these recommendations. The prevalence of CHC claims was also lower among women with SLE with lupus nephritis compared with those without selected autoimmune diseases. Lupus nephritis is an independent risk factor for VTE, 21 and the American College of Rheumatology recommends against CHC use in this population. 2 Specific subgroups of women with MS and IBD may also have other risk factors for thrombosis and should generally avoid CHC. 7 However, we were unable to identify these subpopulations in these data.
In addition to the risk of harm to fetal growth and development, at least one fetotoxic medication, mycophenolate mofetil, may reduce the efficacy of CHC; therefore, the U.S. Federal Drug Administration label and Risk Evaluation and Mitigation Strategy website recommends caution with CHC use.22,23 In our analysis of women with any of the selected autoimmune diseases and selected fetotoxic medications, approximately 70% did not have permanent or prescription contraception claims in 2019, similar to previously published results from a single-site rheumatology study. 12 Because these medications are associated with significant teratogenic or abortifacient risk, continued outreach to and education of health care providers and their patients can support discussions about contraception and pregnancy planning.
Improved care coordination for women with autoimmune diseases might facilitate improved contraceptive access for this population. In one study, only 32% of women with rheumatic conditions had seen a gynecologist in the last 2 years. 12 Furthermore, subspecialty clinicians might not feel equipped to discuss or prescribe contraception; similarly, reproductive health specialists might be unsure about the effects of contraception on disease status or disease-modifying antirheumatic drugs. 24 In a small cohort of women with SLE, one-third reported that they did not receive contraceptive counseling from their rheumatologist when starting a new teratogenic disease-modifying antirheumatic drug. 25 In a chart review of 100 women with IBD in an academic gastroenterology practice, about 28% of those using fetotoxic drugs (Category D or Category X) had documentation of contraceptive use. 26 Contraceptive counseling, visits with obstetrician–gynecologists, and other interventions have been associated with increased contraceptive use among women with rheumatologic conditions.12,27 Opportunities to educate medical subspecialists and reproductive health providers, build and expand referral networks, and disseminate contraception guidelines can improve patient-centered multidisciplinary care of women with autoimmune diseases. 2
Many factors contribute to contraceptive decision-making. In a national survey of reproductive-aged women, reasons for contraceptive nonuse included seeking pregnancy, not being sexually active, pregnancy ambivalence, or worry about contraceptive side effects.19,28 In one qualitative study of reproductive-aged women with autoimmune diseases, emergent themes included concern of contraceptive safety in the context of their rheumatic conditions and feeling like they already take too many medications. 29 In the same study, one participant expressed tension with her health care provider who insisted she use a more effective contraceptive method when she preferred to use condoms. Other research has described a similar tension between and among patients and health care providers in reproductive health, calling attention to the risk of reproductive coercion in contraceptive counseling.30–32 Several validated tools measuring patient-centered contraceptive counseling have been developed to ensure shared decision-making and avoid contraceptive coercion by health care providers.33,34 Women with autoimmune diseases who wish to prevent pregnancy, especially those with complex disease states or fetotoxic medication use, could benefit from patient-centered contraceptive counseling that honors their bodily autonomy and contraceptive values and preferences, including the decision to not use prescription contraception or to use nonprescription methods.
The primary strength of this analysis is the use of a large, nationwide insurance claims database. However, the study is subject to several limitations. MarketScan’s commercial claims dataset is based on a convenience sample of large, employer-based insurance plans, so the sample might not be representative of all commercially insured women; additionally, the Medicaid database does not include all states, limiting generalizability to all Medicaid-insured women. 10 Furthermore, MarketScan does not identify which states are included in the Medicaid database, and states with and without Medicaid expansion may be included together, contributing to data heterogeneity. This analysis does not include Medicare-insured women, which may include young people with disability from chronic conditions such as autoimmune diseases. In one analysis, approximately 10 per 1,000 Medicare beneficiaries younger than 65 years of age had SLE. 35
This analysis was restricted to women who had prescription drug coverage in 2019; therefore, these data may not be generalizable to those without prescription drug coverage. Additionally, we included women enrolled in health care coverage for ≥11 months per year annually from 2016 to 2019, so we cannot characterize contraceptive claims among women without insurance or with gaps in insurance. Among insured women in our analytic sample, we may also have missed contraceptive services that did not result in an insurance claim, especially those who received contraceptive services at publicly funded clinics (e.g., Title X clinics).36,37 This point is particularly salient for adolescents and young adults who may be covered under their parent’s insurance plans and who have concerns about confidentiality. 38
As this is a descriptive analysis, we were not able to assess the temporal relationship between initiation of a contraceptive method and diagnosis of the autoimmune diseases. We attempted to account for multiple contraceptive methods used in a single calendar year (e.g., using the most recent short-acting reversible contraceptive claim if an individual had more than one short-acting reversible contraceptive claim in 2019); however, we may have misclassified users or nonusers based on the current algorithm. Additionally, we were unable to assess all types of contraceptive methods, including barrier methods, fertility-awareness-based methods, emergency contraception, or reliance on a partner’s vasectomy. This likely underestimates contraceptive prevalence among our sample. Because we only evaluated permanent contraception or LARC use over a 3-year period prior to the index year, we might have misclassified women using these methods in 2019 who initiated them before 2016. A previous sensitivity analysis of MarketScan data that searched for LARC or sterilization codes over a 7-year period rather than a 3-year period found an additional 1% permanent contraception codes and an additional 1% IUD insertions 16 ; therefore, we assessed it was acceptable to use only a 3-year period for this analysis.
General limitations of using administrative claims data include potential inaccuracies in coding and variability in coding practices by clinicians, practices, or states. Using contraceptive claims as a proxy for contraceptive use may also lead to misclassification, especially for user-dependent methods for which there is documentation of filled prescriptions but no information on actual use. Given the number and variety of autoimmune diseases studied in this analysis, we chose the conventional method of claims identification and diagnosis (i.e., one inpatient or two outpatient claims >30 days apart); however, more sensitive and specific individual algorithms have been validated for IBD and MS.39,40 Our sample included lower prevalence of women with SLE subgroups than reported elsewhere, which may indicate that additional validation of these diagnoses in administrative health claims datasets is needed.41,42 Furthermore, we used diagnosis codes for APS and could not characterize antiphospholipid antibody positivity outside of APS. As highlighted above, the U.S. MEC and the American College of Rheumatology stratify contraceptive guidelines by antibody positivity.2,7 Similarly, the present analysis does not account for disease severity within selected autoimmune diseases. Finally, comparison groups of women without selected autoimmune diseases might have included women with other autoimmune diseases or chronic medical conditions not analyzed in this study that would affect contraceptive method mix, potentially minimizing differences between groups.
Finally, our analysis lacks information on important covariates that affect contraceptive use, such as type and frequency of sexual activity, pregnancy intention, and contraceptive preferences, and social determinants of health such as employment status, income, housing stability, and education level, 43 which might differ between women with and without selected autoimmune diseases. Some of these covariates may be more important for adolescent populations, who have lower rates of sexual activity and higher rates of condom use. 44
Conclusions
In 2019, most insured women with IBD, MS, RA, and SLE did not have permanent or prescription contraception claims. Contraception claims prevalence varied by autoimmune disease group, with CHCs and IUDs being the most common. CHC claims were lower among women with SLE with APS or SLE with lupus nephritis, consistent with professional organization recommendations to avoid estrogen-containing contraception in these groups. Among women with selected autoimmune diseases with commercial or Medicaid insurance, those with selected fetotoxic medication codes had a lower prevalence of any contraception claim than those with selected autoimmune diseases without these medication codes. Most forms of contraception are safe and effective for women with selected autoimmune diseases; training in evidence-based and patient-centered contraceptive management can improve access to contraception for women with autoimmune diseases.
Authors’ Contributions
J.A.R.: Study conceptualization (lead), methodology (equal), project administration (lead), data visualization (lead), writing—original draft (lead), and writing—review and editing (equal). M.B.T.: Study conceptualization (supporting), methodology (equal), supervision (equal), and writing—review and editing (equal). G.J.: Methodology (equal), data curation (lead), data analysis (lead), data visualization (supporting), writing—original draft (supporting), and writing—review and editing (equal). A.N.: Methodology (equal) and writing—review and editing (equal). K.K.: Data validation (lead) and writing—review and editing (equal). M.W.: Supervision (supporting) and writing—review and editing (equal). K.M.C.: Study conceptualization (supporting), methodology (equal), project administration (lead), supervision (lead), data visualization (supporting), and writing—review and editing (equal).
Footnotes
Author Disclosure Statement
All authors report no conflicts of interest.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention.
Funding Information
No funding was provided for the study.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.