
Abstract
Abstract
Aim:
The aim of this work was to report the technique and result of thoracoscopic repair for a newborn with congenital diaphragmatic hernia (CDH) under high-frequency oscillatory ventilation (HFOV) in the neonatal intensive care unit (NICU).
Methods:
Ventilation was supported by HFOV. The patient was placed in the right lateral decubitus position. Thoracoscopic surgery was performed through three 5-mm trocars. Carbon dioxide insufflation was maintained in the thoracic cavity at a pressure of 6–8 mm Hg. The hernia defect was repaired by using interrupted sutures with extracorporeal knots.
Results:
The operation lasted 60 minutes. The intraoperative course was uneventful. Normal vital signs and PO2 value were maintained throughout the operation. The patient had a normal chest X-ray 1 month after discharge.
Conclusion:
Thoracoscopic repair of CDH in the NICU during HFOV is feasible and safe.
Introduction
Case Report
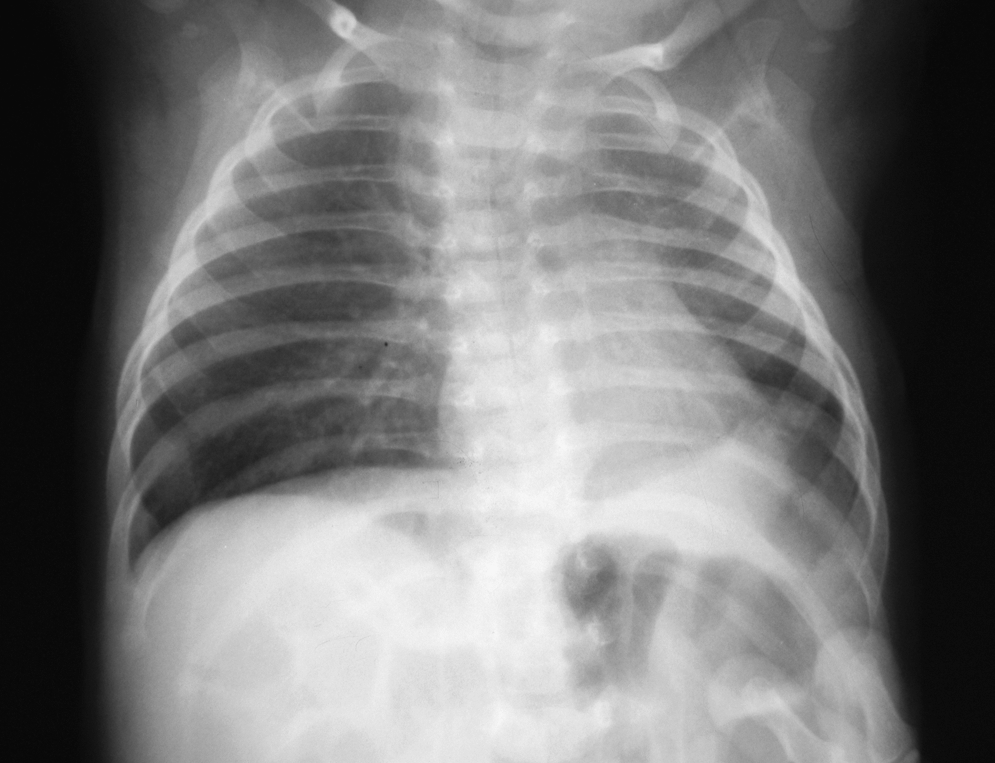
A 3500-g girl who appeared cyanotic immediately after birth was admitted to our hospital at 10 hours of age. The patient was placed on a conventional mechanical ventilator (PIP 18 cm H2O, PEEP 5 cm H2O, rate 40/min, FiO2 0.6). A chest X-ray showed left CDH (Fig. 1). Cardiac ultrasound revealed high pulmonary artery pressure, tricuspid regurgitation, and persistence of a patent foramen ovale. Arterial blood gas on admission showed pH 7.32, PCO2 46 mm Hg, PO2 186 mm Hg, HCO3 23.7 mmol/l, and BE −2.4.

Preoperative CXR.
After 3 hours of conventional mechanical ventilation, the patient's condition became worse, with arterial blood gas values showing pH 7.04, PCO2 111 mm Hg, PO2 27 mm Hg, HCO3− 30 mmol/L, and BE −0.6. Ventilation was switched to HFOV and continued for 5 days. Intravenous ilomedin 2 ng/kg/min was given continuously for 96 hours, dopamine 5–10 μg/kg/min for 102 hours, dobutamine 2.5–5 μg/kg/min for 95 hours, and norepinephrine 0.05–0.1 μg/kg/min for 52 hours. The patient's condition remained stable with HFOV support, but worsened whenever a change from HFOV to conventional ventilation was attempted. For this reason, thoracoscopic repair in the NICU was indicated on the day 5.
At operation, the patient was ventilated by using HFOV (R100 Rotary; Metran, Saitama, Japan): MAP 15–16 cm H2O, frequency 9 Hz, FiO2 0.8. General intravenous anesthesia was carried out with midazolam (0.2 mg/kg), fentanyl (4 μg/kg), and norcuron (0.3 mg/kg) for induction and midazolam (0.1 mg/kg/h), fentanyl (10 μg/kg/h), and norcuron (0.15 mg/kg) for maintenance. The operation was performed with Carl Storz (Tuttlingen, Germany) apparatus. The patient was placed in the right lateral decubitus position with the head elevated. A 5-mm trocar was introduced for a thoracoscope at the mid axillary line in the third intercostal space. A second 5-mm trocar was placed in the fourth intercostal space anteriorly, and a third 5-mm trocar was placed in the fourth intercostal space posteriorly. Carbon dioxide (CO2) insufflation was maintained in the thoracic cavity at a pressure of 6–8 mm Hg. A large posterior lateral diaphragmatic hernia with a sac was found during thoracoscopy. The sac was removed after reducing the hernia contents in the abdominal cavity. The hernia defect was repaired by using nonabsorbable interrupted (Ethibond 3/0; Ethicon France, Neully/Seine, France) sutures, encompassing two borders of the diaphragmatic muscular defect with extracorporeal knots. The lung tissue remained inflated throughout the procedure, and the low amplitude lung vibration did not interfere with surgical manipulations. Operative time was 60 minutes. There were no complications and no blood loss during the operation. Preoperative, perioperative, and postoperative values for SpO2, indirect blood pressure, pulse, and blood gas measurements are presented in Table 1.
IBP, indirect blood pressure.
Postoperatively, HFOV was required for 48 hours, followed by conventional ventilation for 44 hours. Dopamine 5–10 μg/kg/min was given postoperatively for 62 hours, dobutamine 2.5–5 μg/kg/min for 45 hours, and ilomedin 2 ng/kg/min for 24 hours. Extubation was successful on the day 5 postoperatively, and a chest X-ray showed a normal left diaphragmatic curve with good lung expansion. However, prolonged vomiting occurred after surgery, requiring gastrointestinal studies. X-ray findings suggested a gastric volvulus (Fig. 2). Laparoscopy was carried out on the day 27 postoperatively, showing an adhesion between the liver and the greater curve of the stomach. The adhesion was released laparoscopically. After this second operation, the clinical course was uneventful, with no vomiting or dypsnea. The patient was discharged 8 days after the second operation, at 40 days of age. On follow-up 1 month after discharge, the patient was growing and developing well. Chest X-ray was normal at that time (Fig. 3).
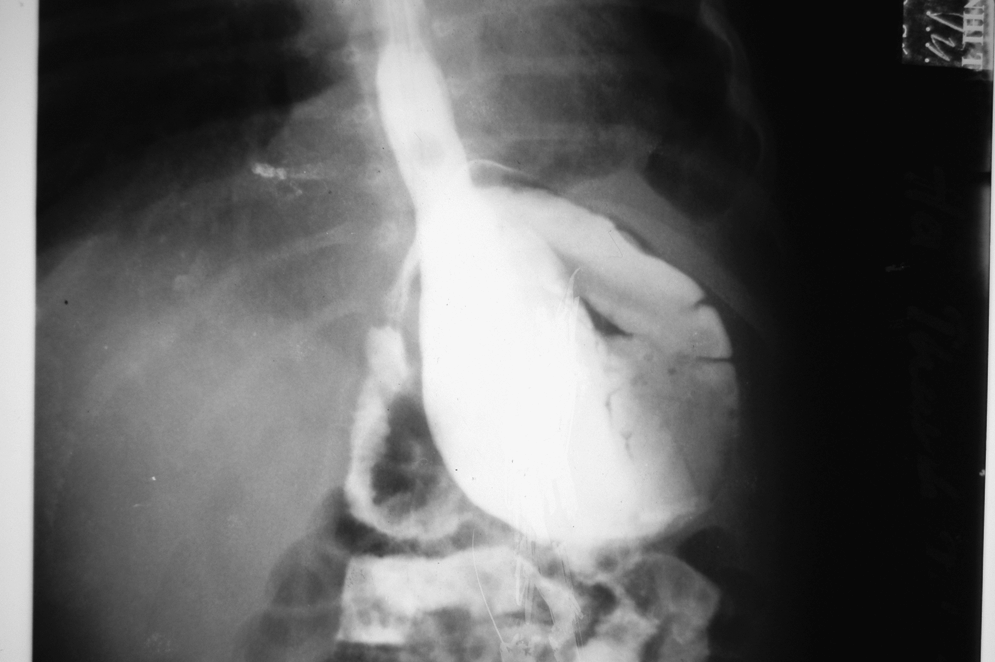
Upper gastrointestinal contract study.
Postoperative CXR.
Discussion
A number of surgeons have used the laparoscopic approach to repair CDH.1–5 However, a thoracoscopic approach has recently become more popular.6–18 According to some reports, the thoracoscopic approach has some important advantages in comparison with laparoscopy.8,10,14,18 It can be applied safely for newborns in stable condition.10–12,14,18
Delayed surgery after good preoperative stabilization of the patient is currently widely accepted.19–22 For the newborn whose condition cannot be stabilized with conventional ventilation, HFOV has been shown to be a useful option to reduce mortality.19–22 Preoperative HFOV can provide adequate gas exchange, reduce lung trauma, correct respiratory acidosis, and reduce pulmonary hypertension.19–21 In 2000, Bouchut et al. successfully performed open surgery to repair CDH during HFOV. 21 They concluded that HFOV appears to be a simple, safe mode of mechanical ventilation during CDH repair. Surgery for CDH can be performed in an operating room or in an NICU. Transfering a critical, unstable newborn from the NICU to the operating room could pose an excessive additional risk. To avoid this risk, some surgeons prefer to carry out open surgery for CDH in the NICU instead of in the operating room. Although there are some important advantages when surgery is carried out in the NICU, the risk of infection may be higher in comparison with surgery in an operating room. 23 Our thoracoscopic operation was performed in the NICU during HFOV without any difficulty. Chest movements and lung vibration at low amplitude did not interfere with surgical manipulations. Normal vital signs and SpO2 value were maintained during the operation (Table 1). CO2 pressure between 6 and 8 mm Hg did not interfere with vital signs or SpO2 values during HFOV. Because surgery was performed through three small incisions, infection risk was reduced in comparison with open surgery. 23 Our patient had no findings of postoperative infection. Operative time was 60 minutes, comparable with open surgery. 23 The thoracoscopic approach causes less trauma for the patient because muscles are not split, as is seen in thoracotomy or laparotomy—very important for a patient in critical condition.
Conclusion
In conclusion, thoracoscopic repair of CDH in the NICU during HFOV support can be carried out safely. This option may decrease the mortality rate in the severe CDH patient who required HFOV. However, more experience is mandatory to fully evaluate this procedure.
Footnotes
Acknowledgment
The authors thank John Taylor, MD, PhD, from the Department of Pediatrics School of Medicine at the University of Washington, Seattle, WA, for his careful reading and valuable comments on the manuscript.
Disclosure Statement
No competing financial interests exist.