
Abstract
Abstract
Introduction:
The safety and feasibility of laparoscopic liver resections have recently been confirmed. This has encouraged laparoscopic surgeons to widen the indications and push the boundaries in laparoscopic liver resections. However, a complete laparoscopic two-stage liver resection has not been reported previously.
Aim:
The aim of this work was to assess the feasibility and safety of the two-stage laparoscopic liver resection for metastatic disease.
Methods:
The two-stage laparoscopic liver resection was safely performed in a 58-year-old man with colorectal liver metastasis (one in segment 2/3 and one in the right lobe). A left lateral sectionectomy was first performed, followed by right portal vein embolization 1 week later, and a nonanatomic resection of the right liver was performed after 6 weeks.
Conclusions:
Laparoscopic liver surgery is gaining popularity and major procedures can now be performed in centers with wide experience. The laparoscopic approach should always be considered for left lateral sectionectomy, and in selected cases, a complete laparoscopic two-stage resection can safely be performed.
Introduction
Case Report
A 58-year-old man was referred to our unit for colorectal liver metastasis. He underwent a low anterior resection for a rectal carcinoma 2 years ago, and the histopathology results showed moderately differentiated Duke's C (PT3N2) carcinoma of the rectum with infiltration into five lymph nodes. He received postoperative chemotherapy, based on oxaliplatin and capecitabine. He had previous history of asthma and was on regular nebulization for it. His preoperative magnetic resonance imaging (MRI) scan suggested two lesions: one in segment 2/3 (Fig. 1) and one in segment 6/7, which was confirmed on an MRI scan (Fig. 2–4). His scans were discussed in the multidisciplinary meeting and the decision was taken for a one-stage laparoscopic left lateral sectionectomy with segment 6/7 metastatectomy. During explorative laparoscopy and intraoperative ultrasound, the segment 6/7 lesions were found to be bigger than they had appeared on the preoperative MRI scan (which was done 9 weeks before the operation, as surgery was delayed for a few weeks due to the patient's personal reasons) and was extending in the right anterior section. The patient had a small segment 4 and 1. Therefore, an intraoperative decision was taken for a two-stage operation. A left lateral sectionectomy (LLS) was completed laparoscopically, as described previously, 9 using an ultrasonic dissector (Lotus™; Laparoscopic Operation by Torsional Ultrasound, Devon, UK) and endoscopic stapler (Echelon 60; Ethicon Endo-Surgery, Cincinnati, OH). The patient had an uneventful recovery and was discharged 1 day after his operation. One week later, he was readmitted for 1 day for a right portal vein embolization. This was performed under sedation and the right portal vein was embolized with gelfoam slurry alone. A repeat computed tomography (CT) scan was performed after 4 weeks, which showed hypertrophy of segments I and IV (Fig. 5). Figure 6 demonstrates the increase in the size of the segment 6 lesion after the first-stage LLS.
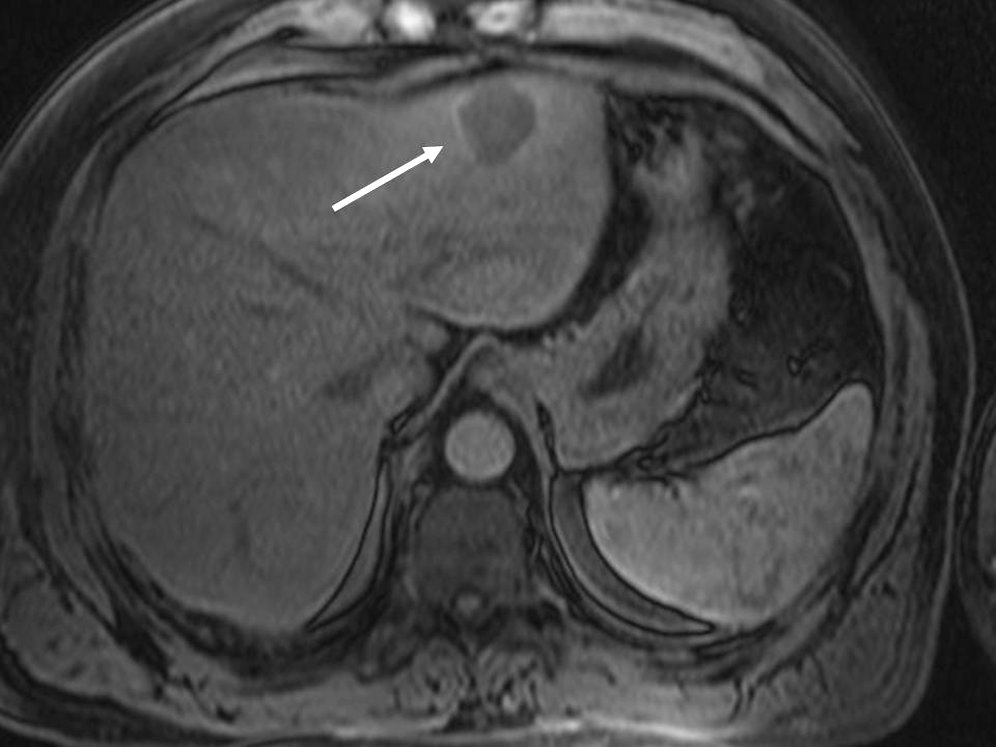
Post–supraparamagnetic iron oxide contrast-enhanced arterial phase T1 VIBE magnetic resonance imaging image demonstrating a well-defined lesion in segment 2 (arrow).

Post–supraparamagnetic iron oxide contrast-enhanced arterial phase T1 VIBE magnetic resonance imaging image demonstrating a well-defined lesion in segment 6 (arrow).
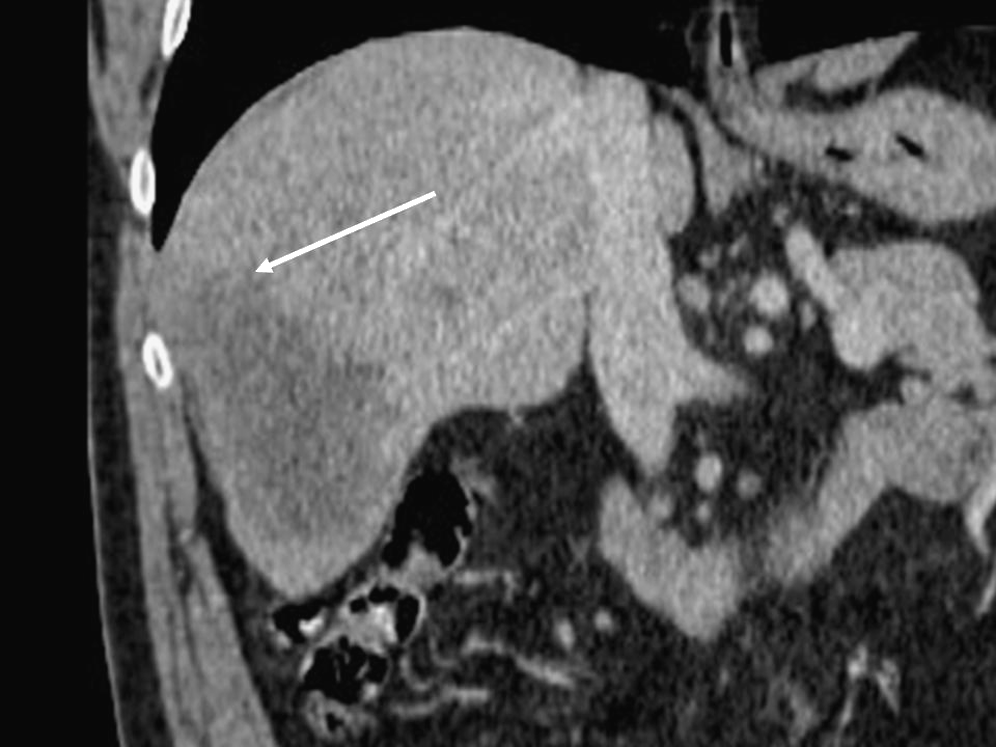
Coronally reformatted portal venous phase IV contrast-enhanced computed tomography demonstrating involvement of the inferior aspect of segment 7 (arrow) by the large, predominantly segment 6, tumor.
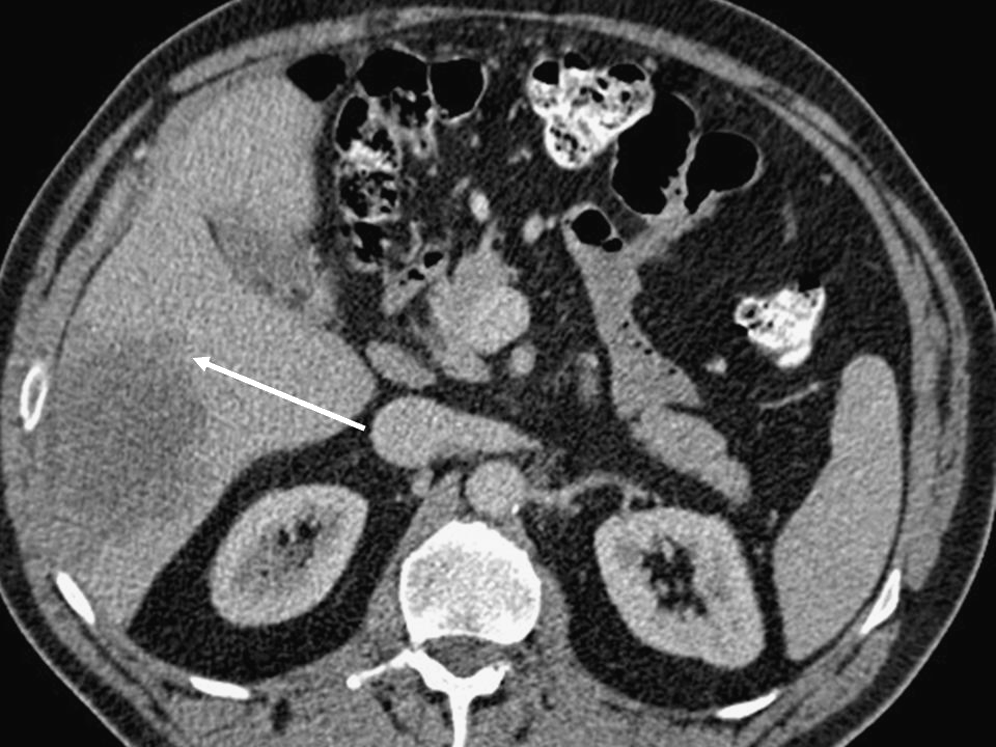
Portal venous phase IV contrast-enhanced computed tomography demonstrating tumor impinging on segment 5 (arrow).
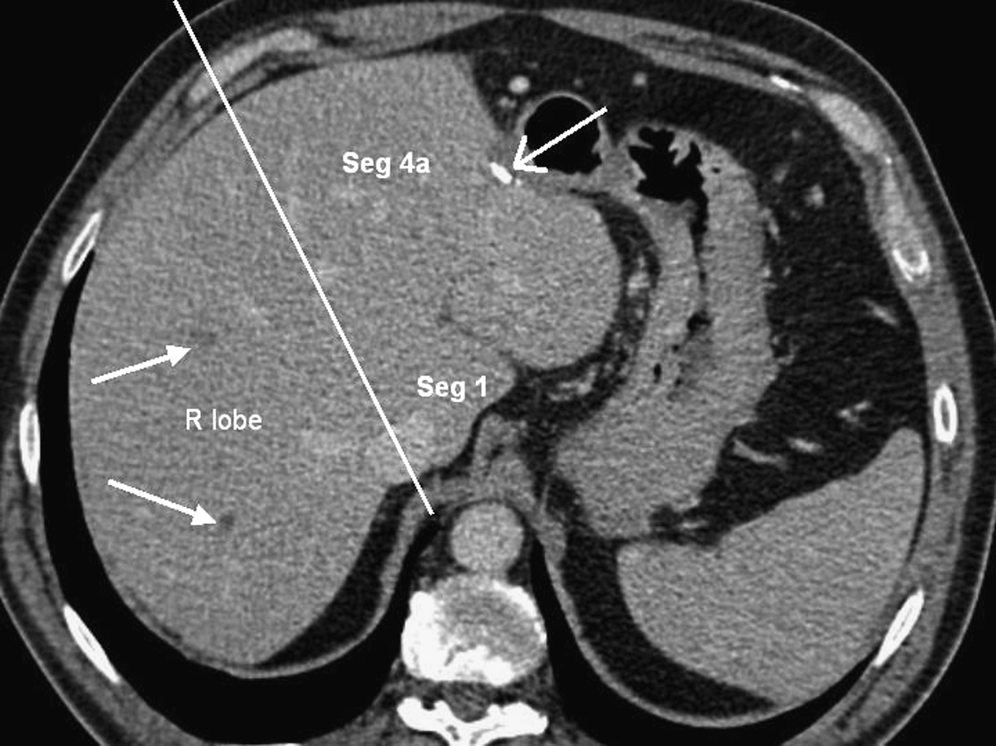
Portal venous phase IV contrast-enhanced computed tomography (CT) demonstrating good hypertrophy of segments 1 and 4 with a clot demonstrated in the right portal vein branches (arrows). CT obtained 4 weeks post–portal vein embolization. Surgical clips demonstrate the previous left lateral sectionectomy (open arrow).

Portal venous phase IV contrast-enhanced computed tomography demonstrating increase in size of the segment 6/7 lesion (arrow); segment 6 component illustrated.
Six weeks after the first operation, patient was readmitted for a second-stage laparoscopic liver resection. The pneumoperitoeum was created by the open technique at the right-upper quadrant. Three more ports were inserted in the right-upper quadrant. Due to previous surgery, dense adhesions were encountered, and passing a sling round the porta hepatis was found to be risky, so Pringle's maneuver (intermittent 10:5 minutes) was performed using a laparoscopic endovascular Debakey Tangential Occlusion Clamp (B/Braun®; Aesculap, Melsungen, Germany). An intraoperative ultrasound scan showed a solitary lesion 2–3 cm away from the middle hepatic vein, and a limited right hemihepatectomy was performed. The liver parenchyma was dissected by using a combination of instruments: Lotus (Laparoscopic Operation by Torsional Ultrasound); the Cavitron Ultrasonic Surgical Aspirator (CUSA, Valleylab, Boulder, CO); and Ultrasonic coagulating shears (Harmonic shears; Ethicon Endo-Surgery). Endoscopic staplers (Echelon 60; Ethicon Endo-Surgery) were used to control major in- and outflow vessels. Medium-size structures (4–6 mm) were controlled with Hem-o-lock clips (Weck Closure Systems, Research Triangle Park, NC), and smaller structures were controlled by diathermy, stitches, and legaclips.
The specimen was retrieved in a leakproof endobag (Autosuture™; Autosuture, Norwalk, CT) and delivered through the lower aspect of the previous midline incision. Two peritoneal drains were inserted close to the resection margins. Patient received 2 doses of antibiotics postoperatively. Two days postoperatively, the patient developed tachycardia and hypoxia and a CT scan revealed a bilateral basal consolidation, which was treated with antibiotics and chest physiotherapy. All the drains were removed on day 6, and the patient was discharged home 7 days following his surgery. The histopathology results confirmed adenocarcinoma with at least 1 cm of free resection margins. The patient was seen in the follow-up clinic and is doing very well 6 months after the surgery.
Discussion
Colorectal cancer is one of the most common malignancies in the UK, and up to 50% of patients develop metastasis to the liver at some point in the natural course of the disease. 10 Liver resection has been recognized as the treatment of choice for these patients.11,12 Historically, only 20% of these patients would have to be deemed resectable, 10 but with the new multidisciplinary therapies (i.e., portal vein embolization, 13 neoadjuvant chemotherapy, 14 transarterial neoadjuvant immunochemotherapy, 15 local tumoral destruction 16 ), along with the improvement in cross-sectional imaging and techniques of surgical resection, the resectability rate has been increased drastically in patients previously been thought to be “nonresectable.” 17 Laparoscopic liver resection was slow to gain popularity, initially due to the perceived greater operative risk of bleeding from the resection planes, gas embolism, oncologic risks of positive resection margins, potential for tumor seedlings, and inability to palpate the tumor. 2 Recently, various series have confirmed the feasibility, safety, and efficacy of laparoscopic liver resection,3,6,18 and further, different studies have demonstrated better outcomes after laparoscopic liver resection, as compared to open.2,19,20 This has encouraged us and other laparoscopic liver surgeons to widen the indications and to push the boundaries in laparoscopic liver surgery.
In the present case, the one-stage laparoscopic resection of segment 2/3 with segment 6/7 metastatectomy was planned initially, but the intraoperative detection of large-size tumor affecting segments 6, 7, and 5 suggested the need of a more extended resection. The relatively small size of segments 4 and 1 may have not been enough as functional liver remnants, especially after aggressive chemotherapy; thus, the decision was taken for a two-stage liver resection. The two-stage resection is a common standard method of treating bilobar liver disease in open surgery. 21 In our previously published series, 9 5 of our laparoscopic left lateral sectionectomies were performed as a first-stage liver resection. The second stages were always completed open, as they were expected to be difficult due to adhesions and the difficulty of performing the pringle maneuver.
The successful laparoscopic completion of this case has demonstrated that, in selected cases, this approach could be safe, feasible, and efficient. Adhesinolysis added some extra time to the surgery but was completed safely. The use of a laparoscopic endovascular clamp safely and efficiently replaced the need for a sling for the Pringle's maneuver. As the patient had portal vein embolization, we did not go for a hilar dissection and extrahepatic inflow control, and the artery was controlled intraparechymally. This saved a good amount of operative time (total operative time, 250 minutes) with acceptable blood loss (800 mL) and no need for a blood transfusion.
Conclusions
Laparoscopic liver surgery is expanding rapidly. In selected cases, the two-stage laparoscopic liver resection is feasible, safe, and efficient. However, this surgery should be only performed in specialized centers with extensive experience in liver and laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.