
Abstract
Abstract
Introduction:
Secondary diverticula initially serve as a pop-off mechanism in high-pressure voiding. Large diverticula, however, have been implicated in bladder-neck and ureteral obstruction and frequently demand definitive treatment, which, so far, has usually meant excision. We present this first report on using the diverticulum for laparoscopic urothelialized bladder augmentation as a novel procedure.
Patients and Methods:
We performed laparoscopic freehand sutured diverticulocystoplasty in 3 adult male patients suffering from low-capacity, low-compliance bladders accompanied by hydroureteronephrosis. All 3 patients had a dominant large diverticulum with very poor drainage by voiding and catheterization. The technique is described in detail. Patients were followed for upper tract changes and bladder anatomy by cystogram, sonography antegrade pyelography (per case), and laboratory studies.
Results:
The procedures lasted 114–152 minutes. Patients were discharged uneventfully on postoperative day 3. At the 9-month follow-up, mean functional bladder capacity had increased by 266% (range, 195–351), and mean maximum detrusor pressure had dropped by 190% (range, 167–234). At 15–32 months, upper tract dilation has improved in all 3 patients. All patients remain on intermittent catheterization, though with far less frequency than before surgery.
Conclusion:
When there is a dominant bladder diverticulum with poor evacuation, and the bladder is noncompliant, laparoscopic bladder augmentation by the diverticulum (instead of standard diverticulectomy) can afford functional improvement with minimal morbidity.
Introduction
Patients and Methods
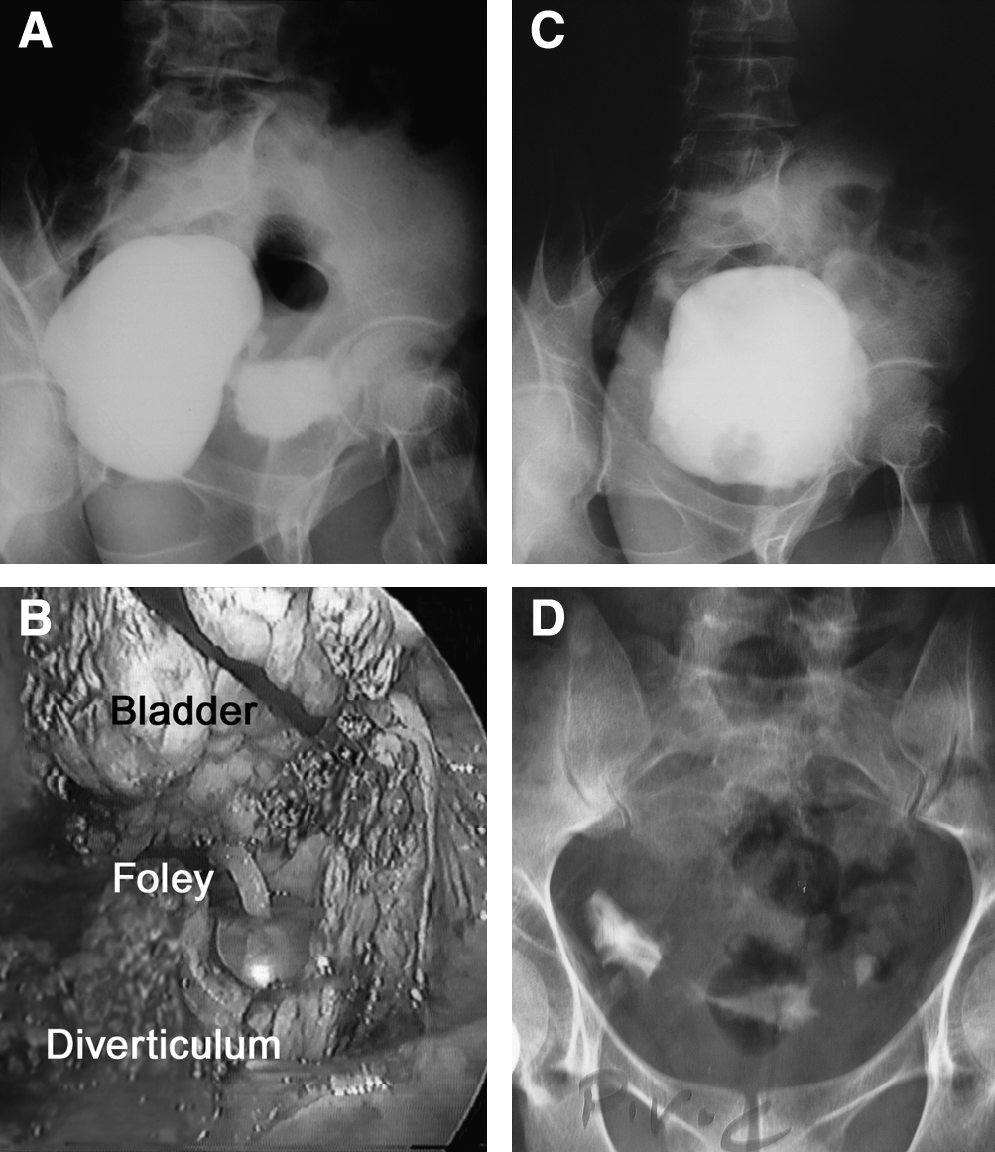
Three adult male patients with dysfunctional voiding were found to have a single (or one dominant) large bladder diverticulum, distinct in its very poor drainage at both voiding and catheterization (Fig. 1A). They had presented with obstructive voiding symptoms and occasional incontinence, yet no anatomic outlet obstruction could be found on cystoscopy, and their cystogram and urodynamics corroborated the assumption of low-capacity, low-compliance bladder with dyssynergy. As outlined in Table 1, all 3 patients were objectively proven to have functional bladder capacities (measured by voiding and catheterization) well below that of the normal adult. This amounted to a 60–70% decrease in reservoir capacity. The combination of outlet obstruction and low compliance (i.e., high-pressure storage) was producing anatomic changes in the upper tract, too, in the form of hydroureteronephrosis. Hyposthenuria, a manifestation of established chronic renal tubular dysfunction in our second case, was itself contributing to the progressive deterioration of the upper urinary tract by burdening the poorly evacuating bladder with a much larger fluid load than it could safely handle. Our first patient had even undergone transurethral resection of about 18 g of prostatic tissue elsewhere, to no avail. The preoperative findings had shown no further improvement on anticholinergics and in temporarily increasing the frequency of clean intermittent catheterization (CIC) to every 2 hours. Recurrent urinary tract infection (manifesting as epididymitis in case 3) and inability to comply with the intense catheterization schedule mandated the need for increased reservoir volume.
(
Description of technique
A flexible guidewire is initially negotiated into the diverticular orifice by cystoscopy, over which an open-ended 12-F Foley catheter is inserted and the balloon inflated to 7 cc. Transperitoneal laparoscopy proceeds in the supine Trendelenburg position, using one 10 mm umbilical and two 5-mm ports on either side of the rectus. Properitoneal fat can encumber the distinction between the bladder and diverticulum, and selective distention of the latter through the Foley catheter, as described, can greatly facilitate identifying the target diverticulum. Using endoshears, beginning on the dome of the diverticulum, an incision is carried down to the catheter, through the orifice, and up along the apposing bladder wall (Fig. 1B). Respective edges of the trabeculated bladder and diverticulum are then anastomosed by using 2-0 polyglactin, in a single layer of continuous locking sutures. The procedure ends by replacing the first catheter with an 18-F standard Foley. We routinely place a closed gravity drain in the retroperitoneum for 3–4 days and repair the peritoneal incision by using the same suture material.
Patients resumed oral fluid intake on postoperative day 1 and were discharged on regular diet and continuous bladder drainage for 2 weeks before resuming CIC every 3 hours. They were followed for clinical evaluation, renal function tests, and sonography of the upper tracts at 1, 3, and 9 months postop. A cystogram was obtained at the 3-month visit. Urodynamic studies were repeated at 9 months. We also documented the improvement in upper tract obstruction in our second patient (who had renal failure) on the 3-month visit, by comparing pre- and postop antegrade pyelograms at 2 hours postinjection of 5 cc of contrast material (Fig. 2A and 2B, respectively).
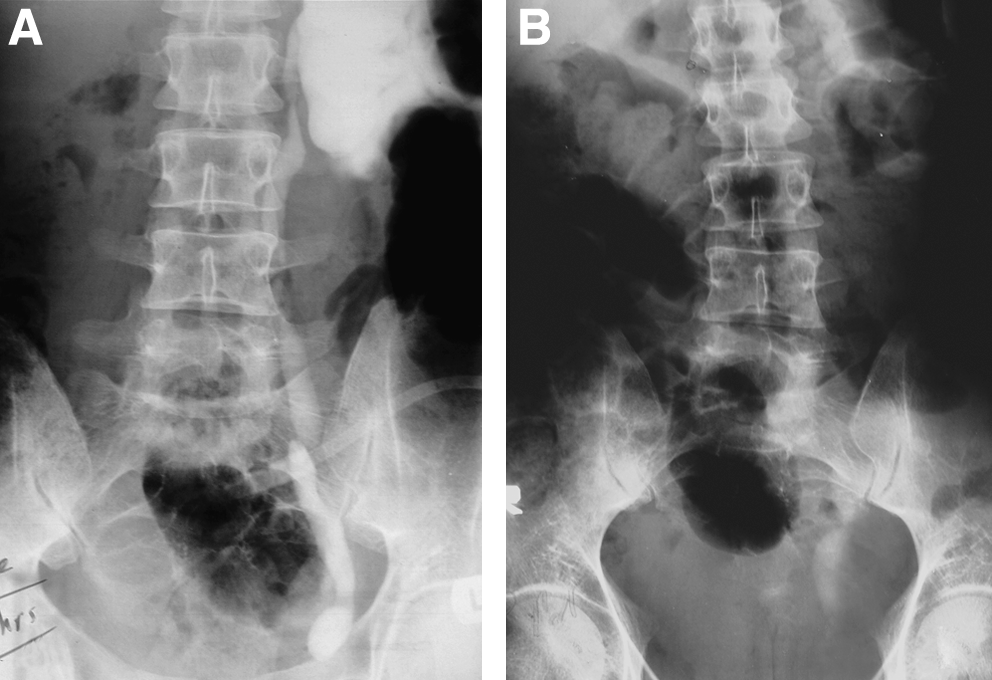
Antegrade pyelogram delayed film at 2 hours: comparing
Results
The procedures lasted 114–152 minutes, including cystoscopy. Blood loss was estimated at 35–70 mL. The hospital stay was uneventful, and patients were discharged on a regular diet and free activity on postoperative day 3. In follow-up, all 3 patients can drain to completion (Fig. 1D), although none could be weaned from CIC. At 9-month follow-up, mean functional bladder capacity had increased by 266% (range, 195–351) and mean maximum detrusor pressure had dropped by 190% (range, 167–234). Catheterization interval has been increased to 4 hours in our second patient and 3–4 times a day in the other 2 cases. Upper tract dilation has resolved in 2 patients and downgraded in the other (Fig. 2B). Reflux ceased in the third patient without any specific surgical intervention (Table 2).
Discussion
The bladder diverticula in our select group of patients were distinct for having markedly impaired drainage. Their capacity, therefore, no longer served as a pop-off, but rather occupied much of the pelvic cavity, leaving little space to accommodate the bladder proper. In addition, the bladder itself was of low compliance and could have benefited from augmentation. The standard approach to such a problem in the lower urinary tract would be augmentation enterocystoplasty, which obviously includes bowel surgery as part of the procedure and forces many more variables into consideration in both short- and long-term management of the patient to curb the unwanted metabolic effects of incorporating the bowel into the urinary system. Using a urothelial lined patch, on the other hand, has proven metabolic advantages over enterocystoplasty, owing to its low absorptive potential and lack of mucus production. 4 The major impediment to the universal use of ureters for ureterocystoplasty, in all cases requiring bladder augmentation, has been the absence of sufficiently dilated upper tracts to provide enough tissue for an effective augmenting segment in many patients. Qualities mentioned as the merits of a urothelialized augmenting patch are shared by the typical bladder diverticulum, plus the fact that, by definition, its lining contains minimal muscular tissue and is, therefore, acontractile.
The longstanding diverticulum tends to acquire a reactive fibrotic backing, however, 1 and this is a potential drawback to its mural tension-relieving function. To date, investigators have almost exclusively described diverticulectomy as the sole surgical solution to any complication attributable to bladder diverticula.1,5 The technique for diverticulectomy, of course, has evolved, along with surgical innovation, from the standard open approach to the endoscopic 6 and laparoscopic. 7 A review of the current literature revealed but one attempt (by Dewan and Lorenz 8 ) at incorporating the diverticulum into the bladder in lieu of its excision, which was performed by open surgery with acceptable results. Building upon our previous experience with laparoscopic ureterocystoplasty, 9 and the presented case series, we conclude that laparoscopic diverticulocystoplasty can likewise represent a less-invasive, cosmetically acceptable option in the surgical management of poorly draining large bladder diverticulae accompanied by a noncompliant bladder. As exemplified by our present 3 cases, sometimes when the ureters are not serviceable or insufficiently dilated to be used as the donor site for augmentation, a secluded bladder diverticulum may be available to provide a less physiologically demanding alternative to seemingly unavoidable enterocystoplasty.
Conclusion
Our proposed reversal in the current paradigm of how to approach a large occlusive bladder diverticulum, where indicated, can also provide a much welcome simplification in the surgical management of these already complex cases.
Footnotes
Disclosure Statement
No competing financial interests exist.