
Abstract
Abstract
The management of neonates with esophageal atresia (EA) associated with right-sided aortic arch (RAA) is often difficult technically. Many surgeons would advise for repair through left-chest access. In this article, we report our experience of repairing 2 patients with EA associated with RAA thoracoscopically. We conclude that thoracoscopic repair is ideal for all patients with EA.
Introduction
The recent introduction of the thoracoscopic approach for the repair of EA has dramatically improved both intraoperative stability and, also, postoperative outcomes. 9 With thoracoscopy, the operative view is magnified significantly to help with dissection and anastomosis. However, no report exists on the thoracoscopic approach in the event of RAA. In this article, we report our series of using thoracoscopic repair for 2 patients with EA and RAA. We showed that the existence of RAA did not interfere with the right-sided approach. We, therefore, recommend the use of thoracoscopic repair for all patients with EA.
Case 1
A newborn baby boy was transferred to us from another hospital with a clinical diagnosis of EA with distal TEF. He was born at 39 weeks with a birth weight of 2.8 kg. Antenatally, polyhydramnios was noted and a nasogastric tube could not be passed after birth. X-ray confirmed the diagnosis, with the tip of the nasogastric tube being at the T3/4 level. Routine echocardiography showed the presence of RAA. No other associated anomaly was noted. Since we were familiar with the thoracoscopic repair of EA, it was decided that we would approach this patient also from the right side. At the operation, the RAA was confirmed. The upper pouch of the esophagus was mobilized and brought anterior to the aorta and then anastomosed to the lower pouch after the ligation and division of the fistula. The baby made an excellent recovery and was discharged on day 18 after the operation.
Case 2
The second baby was also a boy with an antenatal history of polyhydramnios. He was born at 38 weeks by emergency caesarian section because of fetal distress. A copious amount of saliva was noted after birth, and EA was suspected. A nasogastric tube was attempted but could not be passed. A chest X-ray performed showed the tip of the nasogastric tube to be at the T4 level, with the presence of intestinal gas. Thus, EA with distal TEF was diagnosed. Echocardiography showed a 4-mm ventricular septal defect but no apparent RAA. Thirteen pairs of ribs were noted on X-ray. The ultrasonogram of the urinary system was normal.
Thoracoscopic repair of the EA was carried out the following day through the right side. At the operation, RAA, which had not been diagnosed preoperatively, was noted (Fig. 1). The repair was performed in the usual manner with no difficulty. The patient resumed oral feeding on day 5 and was discharged 2 weeks after the operation.
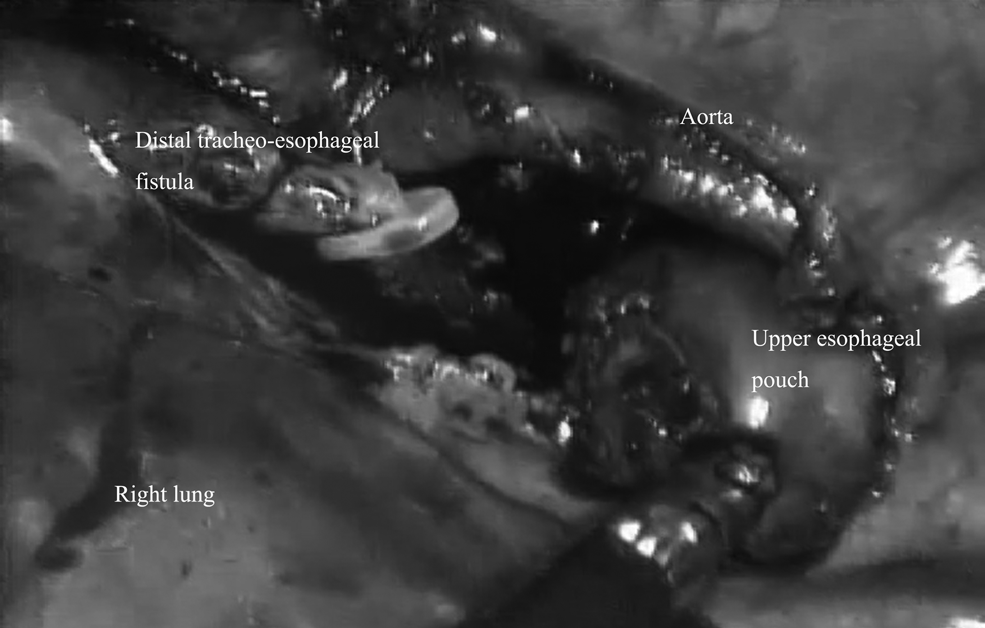
A photo taken intraoperatively during thoracoscopic repair of esophageal atresia showing the presence of right-sided aortic arch.
Discussion
EA and TEF may accompany various cardiac anomalies, including tetralogy of Fallot, transposition of great vessels, atrioventricular defects, and RAA. 10 The incidence of RAA in combination with EA has been suggested to be found in between 5 and 13% of patients.3,4 For traditional open repair of EA, the presence of RAA has been reported by many researchers to increase the technical difficulty of the operation, due to the aortic arch being in front of the esophagus, and that a conversion to a left-sided thoracotomy may be needed. Although the presence of RAA is not a contraindication for the right-sided thoracic approach, many surgeons, including us in the past, would opt to gain access through the left thorax, if the diagnosis of RAA is known preoperatively.7,8 Indeed, in the series of 104 patients described by Holcomb et al., 6 patients who were found to have RAA, either pre- or postoperatively, all received their operative repair through the left chest. 9 As a result, echocardiography has been used to as a noninvasive technique to screen for its presence preoperatively. Despite this, the sensitivity of echocardiography is low, and, as illustrated in patient 2 in our series, the RAA was not diagnosed until during the operation. For patient 1, although we knew of the presence of RAA, we believed that, with a magnified view under thoracoscopic guidance, a right-sided approach was possible. This, indeed, was proven to be the case. Both patients underwent repair with no significant difficulty.
Conclusions
In conclusion, we show that thoracoscopic repair of EA is an advance in surgical technique, and access through the right chest is still feasible in patients with RAA and, therefore, remains our preferential side for the operation of all patients with EA.
Footnotes
Disclosure Statement
No competing financial interests exist.