
Abstract
Abstract
Objectives:
This report is aimed at describing our preliminary experience with the preperitoneoscopic approach to the bladder neck for rectus fascial sling suspension in neurogenic bladder.
Materials and Methods:
A 13-year-old boy with spina bifida was admitted to our institution to treat bladder incontinence. A bladder neck suspension and bladder augmentation was planned. The preperitoneal space was progressively gained by blunt dissection under direct vision (laparoscopy with a single left subcostal trocar), and a total of three preperitoneal ports were inserted. Dissection of the bladder proved to be relatively easy, and the retropubic space as well as the deep pelvis were safely exposed. Owing to the excellent endoscopic visualization, the bladder was dissected downward from the rectum. Once complete mobilization of the bladder neck was achieved, an umbilical tape was passed around the proximal urethra to create an adequate passage for the fascial sling.
Results:
The preperitoneoscopic procedure lasted 2 hours. No complications occurred. A good daytime dry period was achieved at the 4-month follow-up.
Discussion:
Direct visualization of the bladder neck and minimal dissection to the deep pelvis are the key points of this approach. Provided certain technical details are considered, the minimally invasive preperitoneal access is a valuable alternative to the open approach for the rectus fascial sling procedure, particularly when dealing with male patients. Technical advances will, presumably, lead to a complete minimally invasive treatment of urinary incontinence in male patients with spina bifida.
Introduction
The conventional approach requires manipulation and circumferential dissection of the bladder neck and proximal urethra. To reduce the risk of manipulation-related damages, some researchers have suggested technical modifications, including the combined preperitoneal-perineal approach in males and the transvaginal procedure in females. 1 Minimally invasive and robotic-assisted laparoscopic radical prostatectomy and cystoprostatectomy are well-established procedures in adults.13,14 To the best of our knowledge, a preliminary experience in 2 girls with neurogenic bladder treated by robotic-assisted laparoscopic sling suspension has been described, demonstrating feasibility of the minimally invasive approach in children. 3 This is the first report of preperitoneoscopic bladder neck surgery in a boy. The aim of this article is to present our case focusing on technical details and pitfalls.
Materials and Methods
Patient
The patient was a 13-year-old boy (weight, 65 kg) affected by lumbosacral myelomeningocele, neurogenic bladder, and incontinence. The patient also carried a ventriculoperitoneal shunt (VPS). The patient had been treated with anticholinergic drugs (oxybutinin) and antibiotic prophylaxis (amoxicillin/clavulanic acid). Although the patient self-performed CIC 4 times a day, he only achieved a dry period shorter than 1 hour.
Preoperatively, the patient underwent accurate nephrourologic assessment, with the urodynamic study demonstrating neurogenic bladder with low capacity (180 ml), high pressure (more than 50 cm H2O), and low compliance (less than 4 ml/cm H2O). A voiding cystourethrogram (VCUG) demonstrated a right vesicoureteric reflux. The patient was, therefore, scheduled for bladder neck suspension associated with bladder augmentation (enterocystoplasty). Appropriated, detailed informed consent was obtained.
Surgical technique
A large latex-free flatus tube and a 12-Ch Foley catheter were preoperatively inserted in the rectum and the urethra, respectively, in order to intraoperatively facilitate the identification of those structures. A 12-mm Hg carbon-dioxide (CO2) pneumoperitoneum was created with the Verress-needle technique, using a left subcostal incision. A 30-degree 10-mm camera was inserted, and a right paramedian operative preperitoneal access was positioned under direct vision in order to bluntly dissect the preperitoneal space (Fig. 1). The scope was then inserted into the preperitoneal trocar for a proper preperitoneoscopy, and the pneumoperitoneum was evacuated.
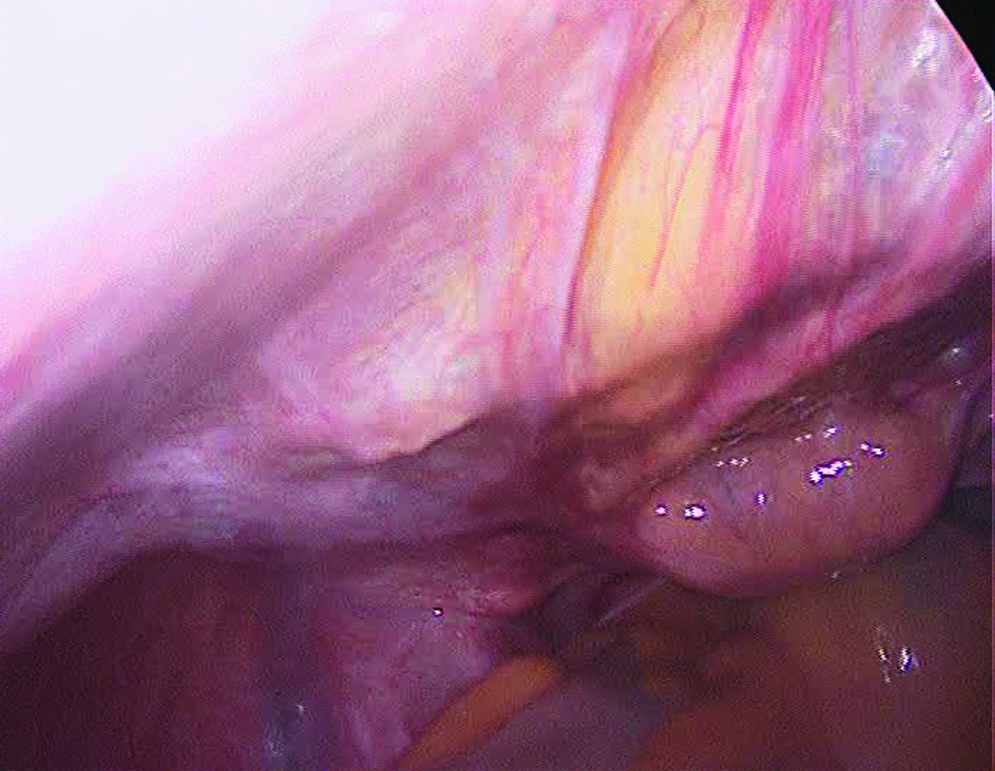
Preparation of the preperitoneal space under direct vision: The bladder and the urachus are identified. This is a well-established maneuver generally used to create the preperitoneal tunneling required for the peritoneal dialysis catheter placement. The prevesical space is achieved by blunt dissection.
Extreme care was taken in preparing the retropubic space and dissecting the prevesical fascia. Two additional preperitoneal operative trocars were placed just laterally to the margin of the rectus muscles on both sides, in order to preserve the integrity of the fascia required to perform the bladder neck sling suspension. The bladder neck was then gently dissected laterally from the obturator nerves and vessels (Figs. 2 and 3). Once the endopelvic fascia was reached, we identified vas and inferior vesical vessels to be spared on both sides. The Foley catheter balloon was easily identified at the level of the bladder neck, thus indicating the correct site for the fascial sling.

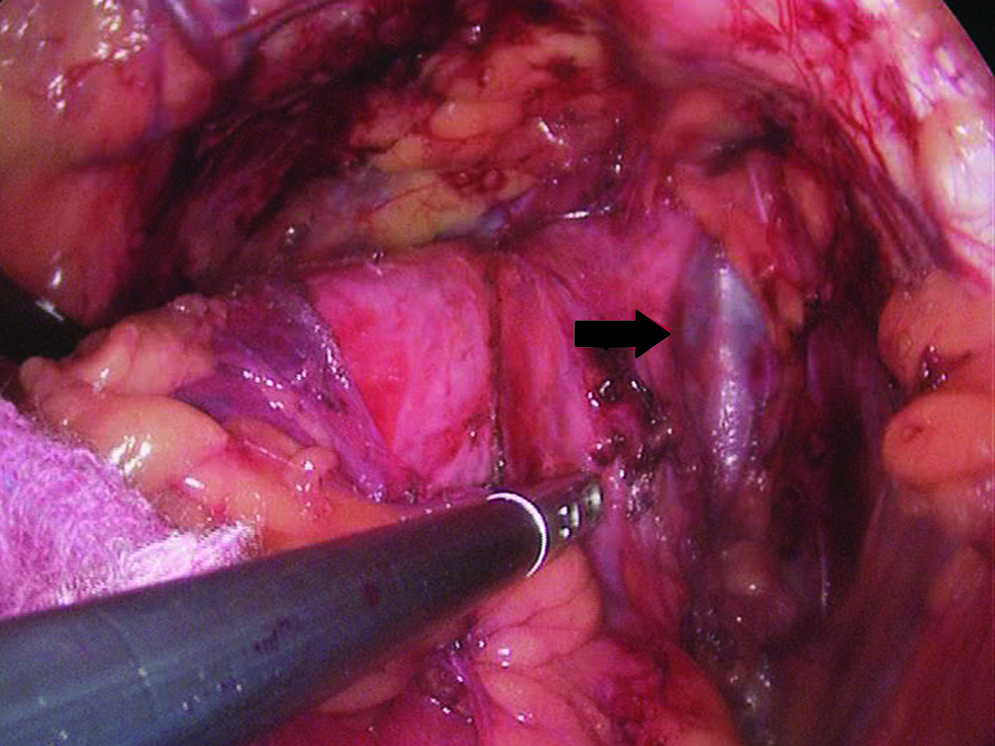
Left anterolateral dissection of the bladder neck: The right obturator nerve and vessels can be seen laterally to the bladder (black arrow), directed deep down into the obturator foramen.
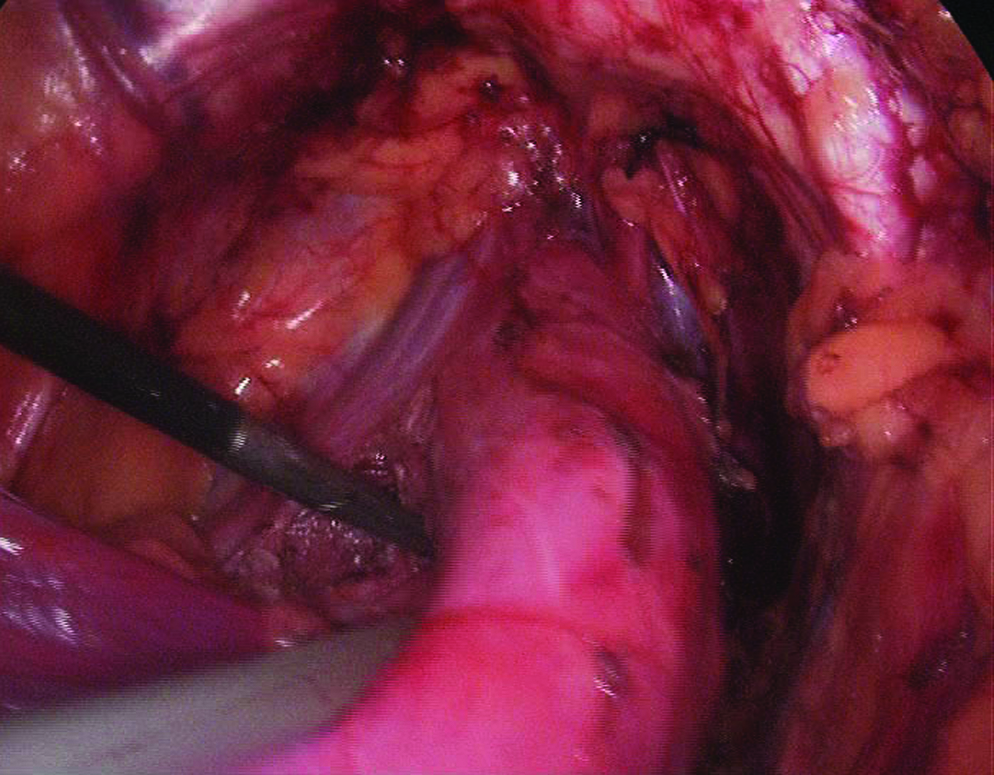
Right lateral bladder neck dissection: Blunt dissection should preserve the inferior vesical vessels (arrow). The Foley balloon is pushed laterally by the tip of the Johan forcep.
Moving further down, a plane between the prostatic urethra and the rectum was gained posteriorly and on both sides to complete bladder neck dissection (Figs. 4 and 5). An adequate window between the posterior urethra and the rectum was easily created by blunt dissection owing to the magnification of endoscopic view. A thin umbilical tape was inserted through one of the operative trocars and gently passed around the bladder neck in order to track the way for the fascial sling (Fig. 6). The procedure was then moved to the open operative step: Through a Pfannenstiel incision, a 15 × 2.5 cm fascia sling was harvested from the left rectus muscle, without interrupting its caudal insertion to the pubic bone. The sling was passed around the bladder neck from left to right and tightly stitched to the left tubercle of the pubic bone. A conventional enterocistoplasty, using the sigmoid colon, was performed through to the same Pfannenstiel incision.
Completion of the bladder neck left lateral dissection and preparation of the posterior dissection from the rectum.
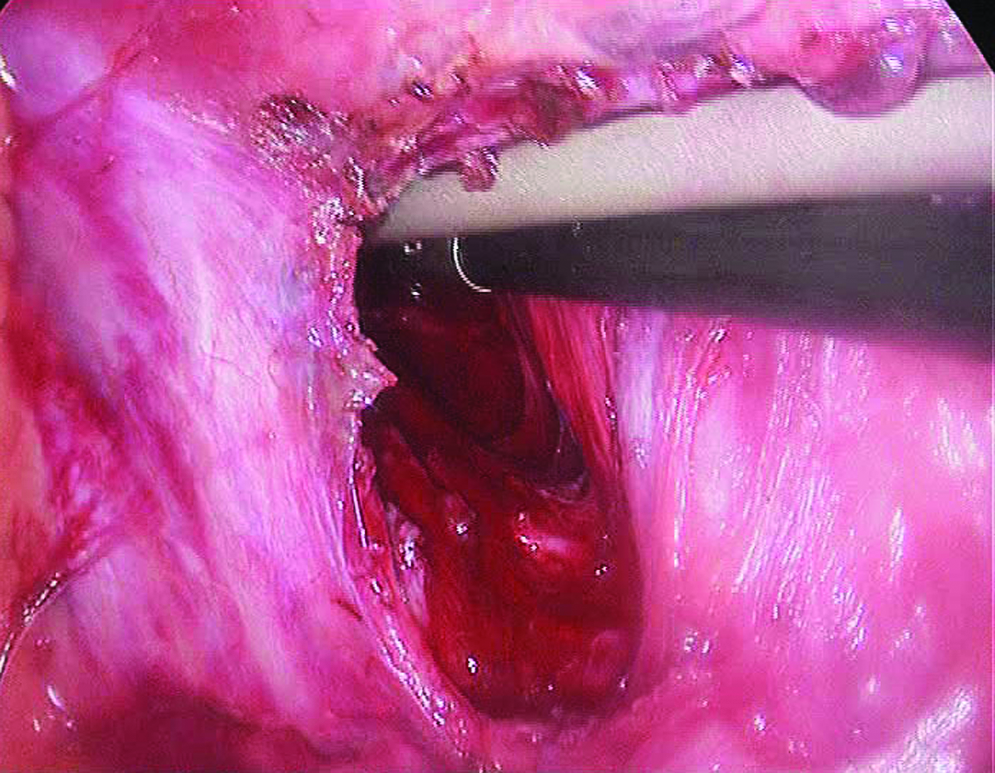
Posterior bladder neck dissection: Dissection from the rectum is usually achieved through a perineal incision. A wide passage between the retrovesical space and the rectum can be easily obtained under direct preperitoneoscopic vision.
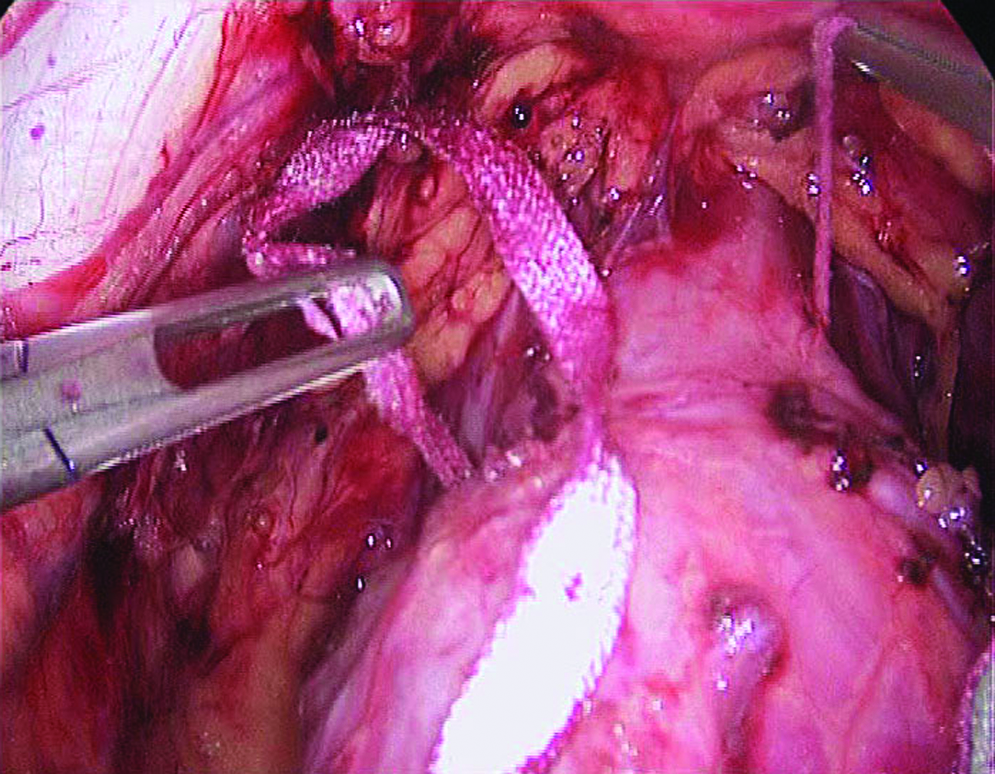
Once the dissection is completed, an umbilical tape is passed around the bladder neck. The tape will then be replaced by the fascia sling. The lumping of the Foley balloon can be seen immediately proximal to the tape.
Results
The preperitoneoscopic bladder neck dissection lasted 120 minutes. No blood transfusion was required, and no intra- or postoperative complications occurred. Systemic pain control with intravenous morphine was limited to 48 hours postoperatively. Bowel movements were reported on day 4, when oral feeding was reestablished. The vesical catheter was left in place for 8 days. The patient then resumed CIC. A limited, self-resolving urine leakage was observed, but a complete healing of the enterocistoplasty was conservately achieved without further occurrences.
The dry period at discharge ranged between 2 and 3 hours. Total hospital stay was 23 days, including 7 preoperative days required for bowel preparation of this severely constipated child. At 4-month postoperative follow-up, the patient showed significant improvement with a 3-hour dry period with occasional night-time wetting. A cystometric measurement of bladder capacity would be scheduled on due course. Anyway, the patient reports bladder-emptying volumes of about 300–350 ml when performing CIC.
Discussion
Since the first fascial sling procedure was described by Woodside and Borden in 1982, 15 many similar techniques and approaches have been reported.10,16–20 Results proved to be better in females than in males who proved to be significantly more challenging.16,20 The perineal approach was proposed to facilitate posterior bladder neck dissection in this subset of patients, though it carries some risks and morbidities related to possible lesions of posterior urethra. The combined preperitoneal-perineal approach provided better results, which still remain worse than those observed in female patients.1,21
The minimally invasive approach was aimed at avoiding perineal incisions and to take advantage of the magnification provided by endoscopic view. Our preliminary experience suggests that a complete bladder neck dissection, even posterior, can be safely and effectively performed preperitoneoscopically. In fact, the endoscopic approach allows direct vision and magnification with a detailed view of deep pelvic structures, which can hardly be obtained with conventional approaches. The dissection that resulted was feasible, safe, straightforward, and effective and provided some technical details:
The initial laparoscopic approach proved to be extremely helpful. It aimed at facilitating blunt preperitoneal dissection, thus preventing CO2 leakage due to serosal tearing. Three trocars are required in the preperitoneal space in order to safely, effectively perform the procedure. We suggest placing one 12-mm trocar on the midline or slightly paramedian, just below the umbilicus in the higher aspect of the preperitoneal space. Further, two 10-mm trocars (one on each side) should be inserted just by the lateral margin of the rectus muscle in order to spare the fascia to be used for the sling procedure and to avoid lesions to the iliac vessels. Bladder neck dissection should be carried out bluntly. When hemostasis is required, the use of the LigaSure™ sealing device (Valleylab, Boulder, CO) limits electric spread and thermal injuries to perivesical nerves and vessels. A large, latex-free, rigid rectal tube as well as a large, latex-free Foley tube are useful to identify the rectum, bladder neck, and posterior urethra. The posterior dissection should be started immediately distal to the level where the Foley balloon spontaneously sits, which identifies the distal aspect of the bladder neck. Once a wide posterior window has been created, an umbilical tape should be passed in order to maintain the route and to allow easier passage of the rectus fascia.
After completion of bladder neck dissection, the procedure can be carried on through an open approach to perform the fascia sling suspension and bladder augmentation, if needed. Indeed, the procedure could be entirely carried out preperitoneoscopically with the use of an acellular matrix sling obtained from small intestinal submucosa. 22 Further, a combined preperitoneoscopic or laparoscopic approach could be hypothesized in case a bladder augmentation is planned, though this would require a far longer length of surgery.
Conclusions
In conclusion, we demonstrated the feasibility of the preperitoneoscopic bladder neck dissection for fascial sling suspension, which, in our opinion, is a valid alternative to the traditional approaches. This new technique proved to be straightforward and safe and should be considered an alternative approach to the bladder neck. Yet, additional studies and careful follow-up are mandatory to confirm our results.
Footnotes
Acknowledgment
The authors would like to thank Mrs. Francesca Roncallo for her invaluable administrative support.
Disclosure Statement
No competing financial interests exist.