
Abstract
Abstract
Objectives:
The aim of this study was to evaluate the feasibility, complications, margin status, and functional outcome (on urinary and sexual functions) of nerve-sparing radical hysterectomy (NSRH) performed laparoscopically.
Methods:
Patients with cervical carcinoma of stage Ia2 and Ib1 underwent laparoscopic NSRH along with pelvic lymphadenectomy. We performed the technique in simple comprehensible steps with anatomic delineation of the autonomic nerves and selective cutting of the uterine and cervical branches.
Results:
Laparoscopic NSRH was feasible in 85.7% of patients. Mean operative time was 160 minutes and all 7 patients had clear surgical margins. There were no complications and no blood transfusions were required. The median hospital stay was 3 days. The median return time for normal bladder function was 2 days and none of them required catheterization beyond 2 weeks. The mean residual urine volume was <50 mL. Urodynamic studies performed at 3 weeks after the operation showed no impairment of maximum flow rate (maximal flow rate: 20 ± 2 mL). The postoperative results of sexual dysfunction were inconclusive.
Conclusion:
Understanding this technique and the knowledge of laparoscopic anatomy of pelvic autonomic nerves is important in both benign and malignant pelvic surgeries. These preliminary results indicate that nerve sparing is easier done laparoscopically and its results are comparable to that of conventional laparoscopic radical hysterectomy in terms of lateral margin status and lymph node yield. Whether quality of life can be benefited by L-NRSH technique and its long-term oncological sequelae need further evaluation.
Introduction
In conventional RH, the paravaginal tissues are cut together with the posterior leaf of the vesicouterine ligament and the paracolpus. The Okabayashi method separates and divides the posterior leaf of the vesicouterine ligament to preserve the autonomic bladder branches. In open radical surgery and by the vaginal route, different nerve-sparing techniques have been adopted for rectal and early cervical cancer and these have been successful in the prevention of urinary, rectal, and sexual dysfunction without compromising surgical outcome.1–9 The indications of autonomic nerve-sparing radical hysterectomy (NSRH) and its advantages over non–nerve-sparing (conventional) RH have been also studied and reported.1–8,10
With advancing laparoscopic surgical techniques, laparoscopic radical hysterectomies (LRH) are now being performed routinely for operable cervical carcinoma. 11 Magnification enabled by laparoscopic surgery facilitates visualization of the surgical anatomy and precise dissection, thus resulting in better delineation of nerves. This in turn may improve bladder and sexual functions by better preservation of the superior hypogastric plexus, the inferior hypogastric plexus, and the pelvic splancnic nerves (PSN).
This led us to perform NSRH using laparoscopic techniques (L-NSRH) in cervical carcinoma International Federation of Gynecology and Obstetrics (FIGO) stage Ia2 and Ib1. The goal was to reduce the urinary and sexual adverse effects of RH without impairing the outcome. As more centers offer the laparoscopic approach, the results, possible complications, and operative difficulties during the early experience must be determined.
The aim of this prospective study was to evaluate the feasibility, complications, technical difficulties, margin status, and functional outcome (on urinary and sexual functions) of L-NSRH in cervical carcinoma.
Patients and Methods
From April 2004 to March 2007, all patients with cervical carcinoma of clinical FIGO stage Ia2 and Ib1 underwent L-NSRH along with pelvic lymphadenectomy at the Galaxy Laparoscopy Institute, Pune. All patients with positive pelvic nodes received postoperative adjuvant radiotherapy.
Preoperative assessment of the patients consisted of history, physical examination, biopsy, CAT scan of abdomen and pelvis, ultrasonography of abdomen and pelvis, chest X-ray, and routine biochemistry. Specific investigations to rule out existing urinary dysfunction were performed when deemed necessary. Urodynamic studies were performed preoperatively. Patients with preoperative bladder dysfunction did not undergo a nerve-sparing procedure.
All patients answered a questionnaire provided to subjectively assess their sexual functions and were assigned a score accordingly.
Examination under anesthesia was performed to rule out parametrial involvement or pelvic spread. Seven patients whose age ranged from 29 to 58 years (median: 50.42 years) underwent L-NSRH. The mean duration of surgery, blood loss, intraoperative and postoperative complications, and the mean duration of hospital stay were analyzed. The number of lymph nodes removed and surgical specimen margins were evaluated. Recurrences and survival were noted.
The Foley catheter was removed after 48 hours in all patients and the residual urine was measured. Urinary symptoms (e.g., overflow incontinence, retention) were noted. The catheter was reinserted if the patient had urinary retention and these patients were reassessed every 7 days. The patients were discharged on the third postoperative day. Urodynamic studies were repeated at 3 weeks after the operation and residual urine volume was again measured. All patients underwent subjective assessment of their sexual functions at 6 months. Any urinary complaints were again noted at 6 months.
Procedure (step-by-step technique)
Step 1: Posterior “U” cut and identification of hypogastric nerve
The ureter is identified medial to the infundibulopelvic ligament and the peritoneum overlying the ureter is cut. The ureter is retracted laterally and the hypogastric nerve is identified posteromedial to the ureter. The peritoneal cut is extended to the pouch of Douglas, keeping the ureter and the nerve constantly under vision. The relation of the uterosacral ligament and hypogastric nerve is clearly seen at this stage (Fig. 1). The rectum is dissected off the posterior vaginal wall keeping in the plane between the fat on the rectum and the posterior vaginal wall to reach the levator ani caudally. This is the plane between the two layers of Denonvillers fascia.
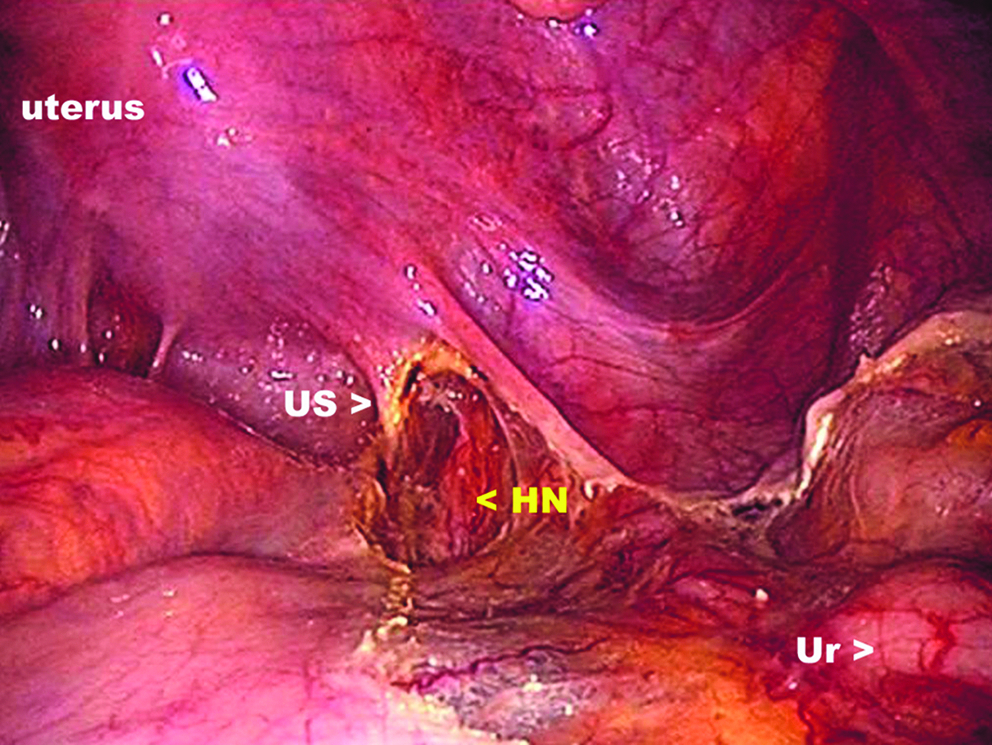
Identification of the hypogastric nerve. The right hypogastric nerve is identified medial to the ureter. Here it is being separated from the uterosacral ligament and the nerve lies just lateral to this ligament, as seen with the laparoscopic magnification.
Step 2: Dissection in pararectal space and dissection superficial to the level of uterine veins, sparing branches of the PSN
The pararectal space, lateral to the ureter, is dissected. The uterine artery is identified, clamped, and cut near its origin. The uterine veins pass below the ureter and are not cut at this stage. The dissection is continued caudally in the plane just anterior to the uterine arteries. This area contains fat and loose areolar tissue, which are easily separated, and the caudal limit of dissection, and the levator ani can be seen (Fig. 2). Posterior to this paravesical area is the cardinal ligament. The cardinal ligament and the uterosacral ligaments together form a fan-shaped structure extending from here to the pouch of Douglas. The deep uterine veins pass through the superficial part of the cardinal ligament and are cut. Below the uterine veins are the branches of the PSN, which run toward the inferior hypogastric plexus (IHP).
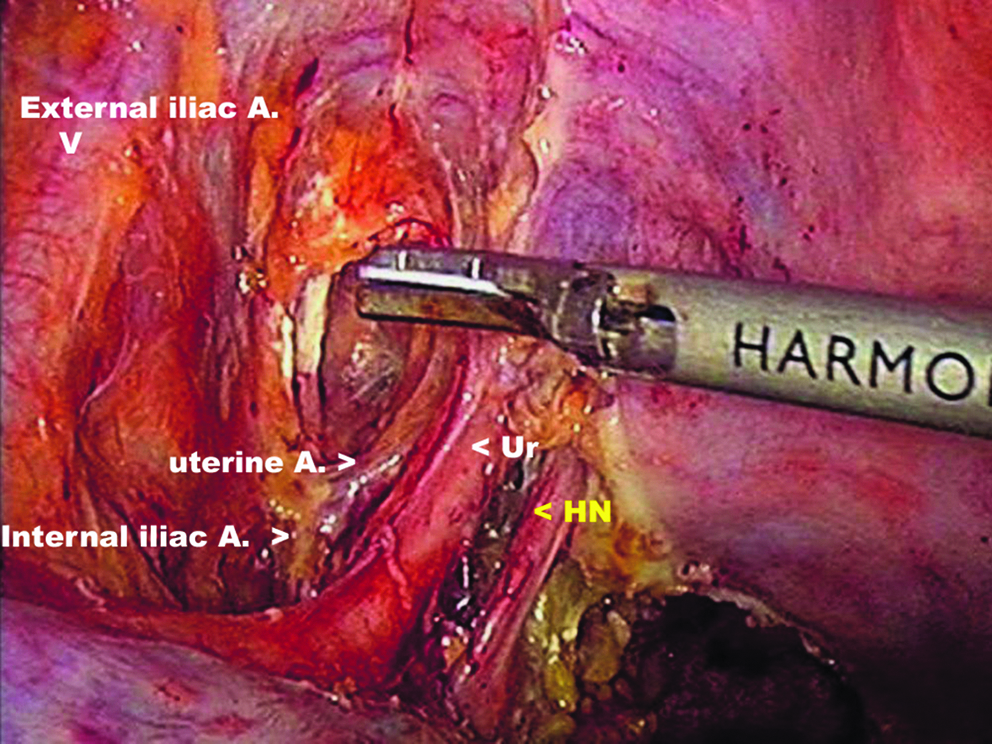
Laparoscopic anatomy of autonomic nerves: Dissection of the pararectal space. Caudal dissection is performed just anterior to the left uterine artery, until the endopelvic fascia covering the levator ani muscle is visualized. The Hypogastric nerve is again seen medial to the ureter and lateral to the uterosacral ligament that has now been cut.
The uterine veins are now well exposed and can be individually clamped and cut, after retracting the ureter. The cardinal ligament, which is superficial and does not contain any nerve fibers, is cut as laterally as possible, thus sparing the PSN (Figs. 3 and 4).
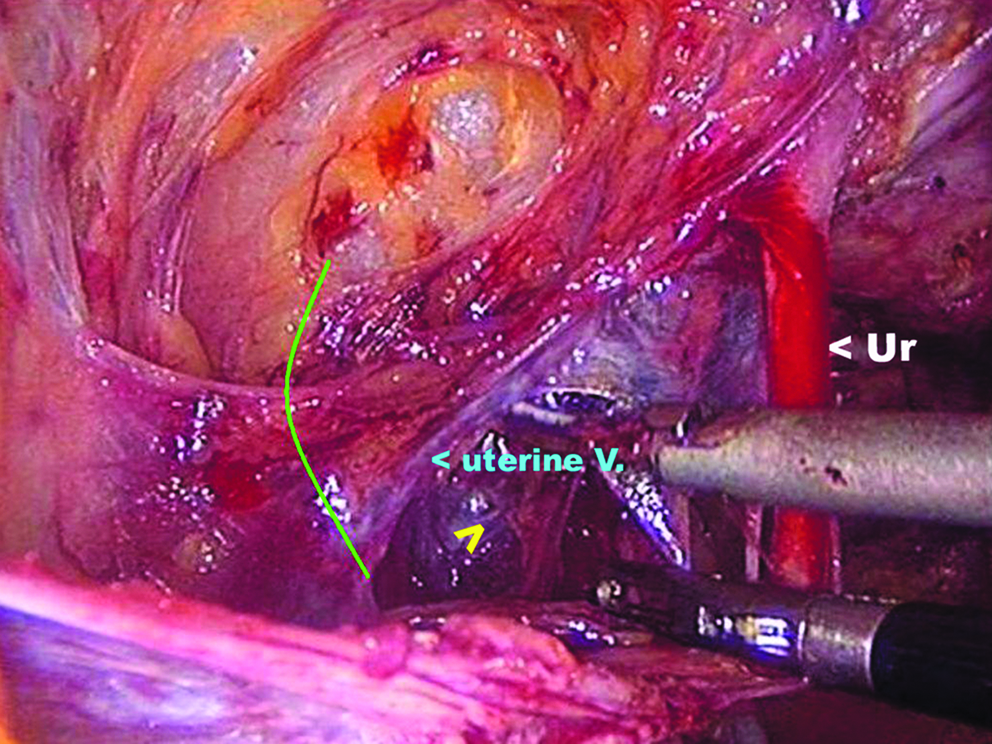
Laparoscopic anatomy of autonomic nerves: Identification of the uterine vein and PSN (pelvic splancnic nerves). The uterine artery has been cut and the left uterine vein is seen passing below the ureter. The PSN lie below this in the bottom of the pararectal space and are indicated by the yellow arrow. The green line indicates the cardinal ligament.
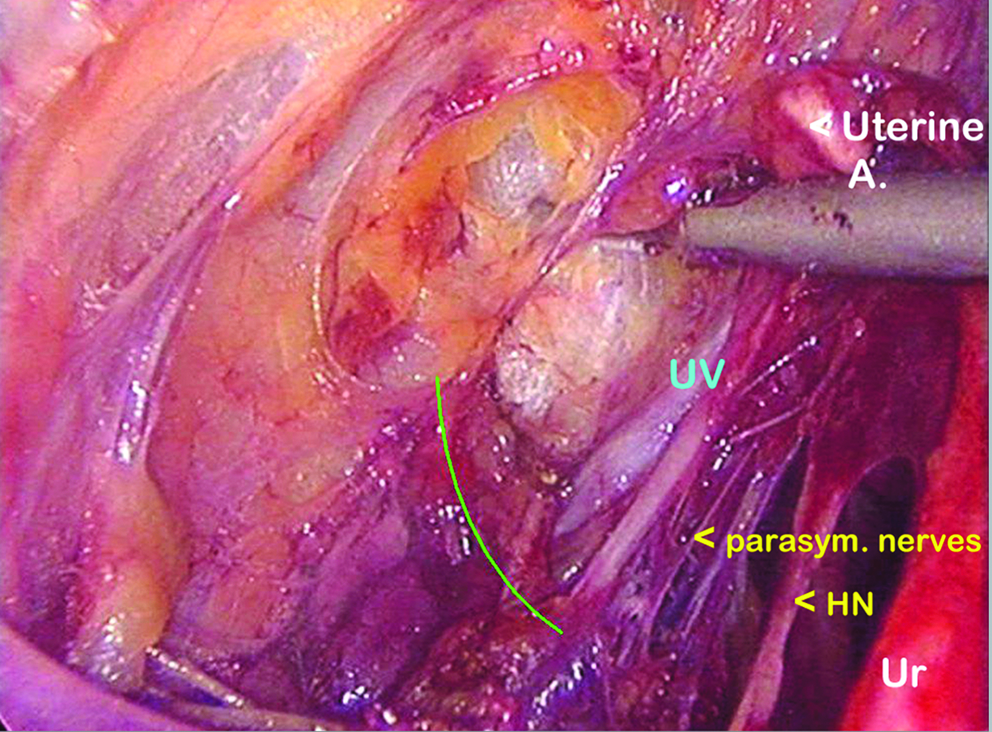
Laparoscopic anatomy of autonomic nerves: Identification of the PSN. The anterior part of the cardinal ligament has been cut (green line), but the left uterine vein (UV) remains intact. The PSN are below the connective tissue fibers, just dorsomedial to the vein.
Step 3: Sparing the hypogastric nerves at the level of the uterosacral ligaments
The hypogastric nerves lie lateral to the uterosacral ligaments. The uterosacral ligament is divided without including the hypogastric nerve. The uterosacrals are cut with the Harmonic ACE™ (Ethicon Endo-Surgery; LLC), protecting the nerve by placing the inactive probe of the ultrasonic shears laterally (Figs. 1 and 2).
Step 4: Selectively cutting some of the uterine branches during posterior dissection
Dissection is continued with a suction probe/scissors in an anterior direction, remaining medial to the hypogastric nerve. The branches of the hypogastric nerve and IHP going to the uterus are identified in the connective tissue just posterolateral to the vagina (Fig. 5). These branches are selectively cut and the nerve plane is lateralized on the posterior side. This completes the posterior part of the dissection. Some branches of the IHP to the uterus and vagina remain intact and these are selectively cut at a later stage during the anterior part of the dissection. The ultimate aim is to spare the bladder branch of the IHP and to lateralize the nerve plane and the ureter.
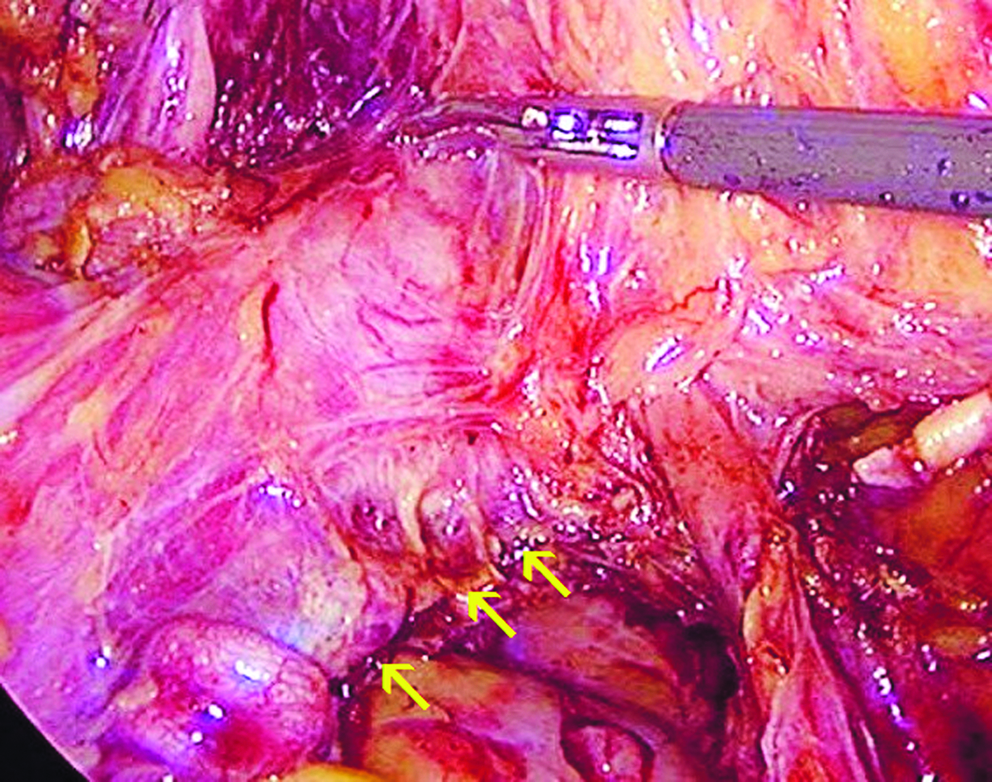
Laparoscopic anatomy of autonomic nerves: Selectively cutting the uterine branches during posterior dissection. The branches of the hypogastric nerve and inferior hypogastric plexus going to the uterus are identified in the connective tissue just posterolateral to the vagina and are selectively cut.
Step 5: The anterior “U” cut and dissection in the anterior leaf of the vesicouterine ligament
The peritoneum is cut from one round ligament to the other. The peritoneum between the infundibulopelvic ligament and the round ligament is cut and a window is created in the broad ligament to visualize the ureter from the anterior side as it enters the ureteric tunnel. The medial stump of the uterine artery is grasped and the ureteric tunnel is bluntly dissected with a Maryland forceps (Fig. 6). Two to three veins course through the roof of the ureteric tunnel (anterior vesicouterine ligament) and these veins are individually identified, clipped, and cut with scissors, and the ureter is pushed laterally. Use of any energy source is avoided in this region to prevent damage to the ureter.
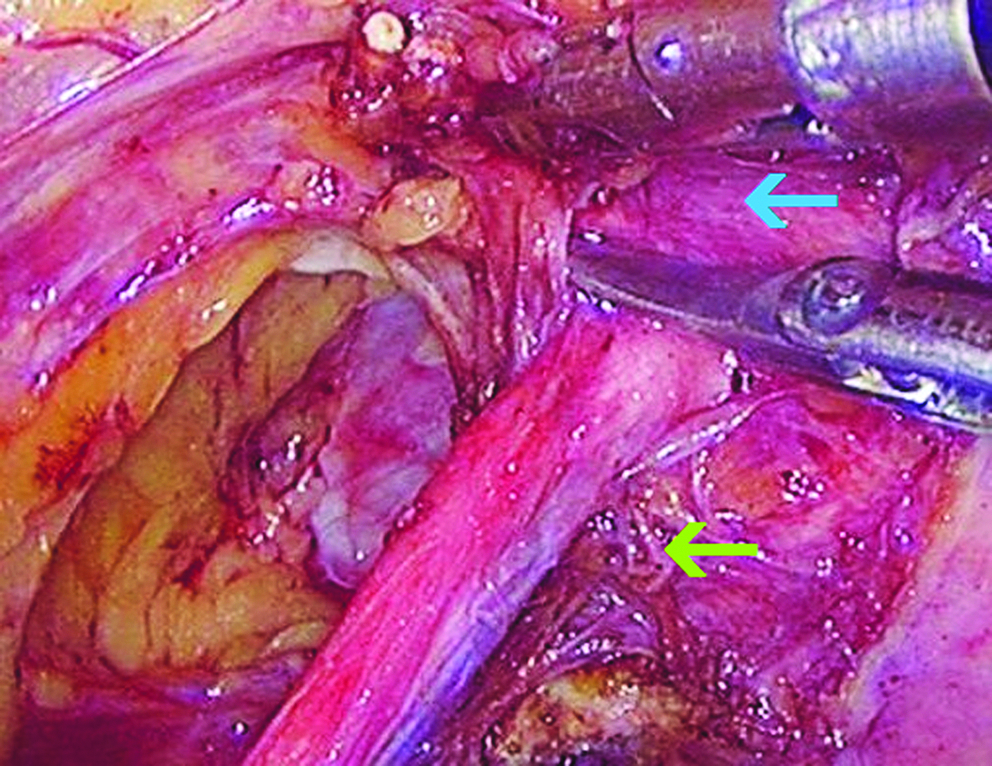
Dissection of the anterior leaf of the vesicouterine ligament (blue arrow). The posterior leaf of the vesicouterine ligament contains the nerves (green arrow).
Step 6: Dissection in the posterior leaf of the vesicouterine ligament and selectively cutting the remaining uterine branches of IHP, sparing the bladder branch
The lateralization of the ureter also pushes the ureteric and the bladder branches of the IHP laterally. The posterior leaf of the vesicouterine ligament contains vesical veins that drain into the deep uterine veins. These are individually clipped and cut. The bladder branch that passes just below this (inferior) vesical vein is now clearly seen and is spared. The uterine and cervical branches of the IHP in the anterior part are selectively cut and this achieves further lateralization of the ureter and the nerve plane (Figs. 7 and 8).
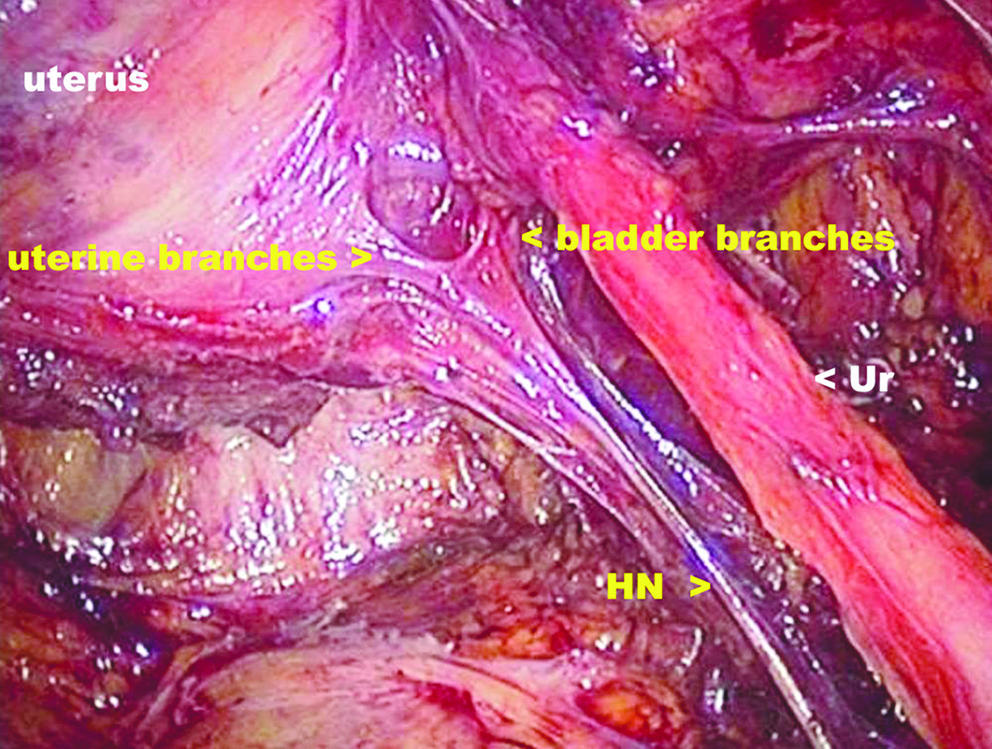
Cutting of the cervical branches: Lateralization of the ureter and further separation of the bladder from the cervix and the vagina. Yellow arrows indicate the cut ends of the nerves to the uterus and cervix.

Lateralization of the ureter and the nerve plane. The yellow arrow points to the preserved bladder branch, which is further lateralized.
Step 7: Dissection of the paracolpos and colpotomy
Further dissection remains medial to the ureter and the bladder branch. These are further lateralized and the paracolpos is cut. At this stage, the nerve appears to be lateral to the ureter (though during the initial part of dissection, the hypogastric nerve and IHP were anatomically posteromedial to the ureter). The bladder is dissected further off the vagina to achieve an adequate vaginal margin.
A similar procedure is performed on the other side. The vagina is then opened and the specimen is separated. The specimen is placed in an endobag. Bilateral pelvic lymphadenectomy is performed and the nodes are also placed in the endobag, which is removed vaginally. Frozen section is performed on any enlarged pelvic nodes, and if positive, para-aortic lymphadenectomy is performed. The vaginal vault is closed intracorporeally with 2,0 polyglycolic acid sutures.
Results
The procedures were completed laparoscopically in all patients. In one patient, only the nerves on the left side could be spared. There were no intraoperative or postoperative complications.
The number of lymph nodes removed and surgical specimen margins (mean) are given in Table 1.
All patients had negative surgical margins. One patient had lymph node positivity (2/22 nodes) and was given postoperative adjuvant radiation.
The mean duration of surgery, blood loss, and the mean duration of hospital stay are given in Table 2.
The Foley catheter was removed on the second postoperative day in all patients. The residual urine volume was <50 mL in 5 patients. The patient with unilateral preservation of the nerves required recatheterization. In all, 2 patients had overflow incontinence and the catheter was reinserted. The time for return of bladder function is given in Table 2.
Autonomic nerves could be successfully preserved bilaterally in 6 patients. None of the patients required any catheter beyond 2 weeks. At 21 days after operation, there was no impairment of residual volume. Urodynamic studies performed at 3 weeks after the operation were comparable to the preoperative studies. There was no impairment of maximum flow rate (maximal flow rate: 20 ± 2 mL), but bladder compliance was impaired. There was no impairment of the urinary function at 6-months follow-up.
The postoperative results of sexual dysfunction were inconclusive (Table 3).
During the study period, no patients had recurrences and no patients died. Two patients have completed a 5-year follow-up and are alive and disease free. The median follow-up is 4 years (range: 1–5 years).
Discussion
Invasive carcinoma with disease confined to the cervix or upper vagina (FIGO stage Ia, Ib, IIa) are conventionally treated by open RH, Piver's Type III. There is no treatment of choice for early-stage cervical carcinoma in terms of overall or disease-free survival. Optimal treatment for each patient should take into account clinical factors such as menopausal status, age, medical illness, histological type, and cervical diameter to yield the best cure with minimal complications. Thus, the surgery preserving the autonomic nerves to the pelvic organs, thereby avoiding sexual and urinary dysfunctions, is preferred over radiation in early cervical carcinoma where results are comparable.
A number of patterns of urinary dysfunction have been described following RH.12,13 Urinary dysfunction can manifest as hypotonic or hypertonic vesical dysfunction, loss of bladder sensation, urgency, stress incontinence, vesicourethral reflux, cystocoele, inability to void, high residual urine volume, and detrusor instability.
Problems of urinary functions are a result of myriad contributory factors. Dissection of the bladder off the vagina results in loss of angulation and support to bladder base. The trigone of the bladder rests on the upper 1/3 of the anterior vaginal wall, which is removed during RH. The fibers of pubovaginalis, which are present inserted in the vagina, are also cut, contributing to incontinence. This may be further aggravated in LRH, if longer vaginal margins are obtained during laparoscopic surgery. If there is weakening of the pelvic diaphragm, downward displacement and funneling of posterior urethra and vesicourethral junction lead to decreased intraurethral pressure (IUP), causing urethral incompetence (stress incompetence).
Our experience with LRH 11 after 3 years of follow-up indicated that these patients had the same sexual and urinary dysfunctions as with the open method. We noted that with laparoscopy the vaginal margins are longer (mean: 3.5 cm). This is probably due to better dissection in the depths of the pelvis. This in turn may also adversely affect the bladder and sexual functions.
Postoperative voiding dysfunction as a result of damage to the pelvic autonomic nerves is well known after colorectal resection for digestive tract carcinoma (60%). 14
Reported cases in literature have used magnifying lenses-assisted NSRH for prevention of nerve plexus trauma. 15
Fujii et al. have also used magnification (2.5 times) to clarify the anatomy necessary for the nerve-sparing Okabayashi RH. 16 They meticulously separated the blood vessels and connective tissues to preserve the PSN, the hypogastric nerve, and the bladder branch of the IHP under magnification (2.5 × ) during the Okabayashi RH performed in 24 patients (FIGO stage IB, n = 22, and stage IIA, n = 2) with cervical carcinoma.16,17 Thus, magnification greatly aids dissection of nerves.15–17 The uterine vein is an important landmark in a nerve-sparing procedure. In our technique, we have identified the nerves, preserving the hypogastric nerves, PSN, and the autonomic branches to the bladder using laparoscopic magnification and access, for precise nerve dissection. In addition, unlike open surgery, no retraction of the nerves was required when dissecting lateral or medial to the nerves. It has to be noted that no energy sources were used during dissection near the nerves, to avoid inadvertent nerve damage.
Querleu et al. have performed modified radical vaginal hysterectomy with laparoscopic nerve-sparing dissection of the lateral portion of the cardinal ligament. 18 Possover et al. have performed laparoscopically assisted vaginal hysterectomy in stage Ib1 and IIIa Ca cervix to reduce the rate of slow transit constipation after type III RH. They concluded that preparation of parasympathetic nerves and fixation of terminal rectum can prevent postoperative constipation. 5
We performed L-NSRH in patients with early cervical carcinoma, limited to the cervix only, with tumor size <4 cm and no paracervical spread.
Autonomic nerves could be successfully preserved during L-NSRH in 85.7% of patients. The catheter was removed on the second postoperative day in all patients. The mean residual urine volume was <50 mL. Only 2 patients required reinsertion of catheter. Possover et al. have evaluated that the mean time to return to normal bladder function is 11.2 days in patients undergoing NSRH by open method. We removed the catheter at 1 week in 1 patient and at 2 weeks in 1 patient.
There was no impairment of residual urine volume at 3 weeks after operation and the urodynamic studies showed no impairment of maximum flow rate, but bladder compliance was impaired in 2 patients. Thus, with L-NSRH, short-term urodynamic impairments associated with conventional non-NSRH were relieved.
Kato et al. have concluded that the bladder function of patients in the unilateral nerve-sparing group immediately after surgery was more damaged than that in the bilateral nerve-sparing group. 19 In our study, the nerves on one side could not be preserved in 1 patient and this patient had postoperative urinary dysfunction (retention with overflow) and sexual dysfunctions. In this patient, only unilateral preservation of the nerves was done because the main issue during this surgery is oncological safety and not quality of urinary or sexual function.
Patients treated with conventional RH and radiotherapy suffer from short-term sexual difficulties.12,13 The pathophysiology implicated in sexual dysfunction after surgery includes dysparunia, lack of vaginal lubrication, disturbed vaginal blood flow, and loss of libido.12,20,21
In our study, a subjective assessment of sexual dysfunction was done with a questionnaire answered by the patients preoperatively and 6 months postoperatively. The postoperative results were inconclusive. L-NSRH may improve sexual dysfunction; a larger series would be required to comment on the improvement of sexual dysfunction.
With the acceptance of laparoscopy in gynecological oncology, more procedures are being done laparoscopically. At our institute, we also have a good experience of preservation of autonomic nerves during laparoscopic radical prostatectomy and laparoscopic low anterior resection in colonic malignancy, where nerve damage can lead to sexual dysfunctions such as impotence and retrograde ejaculation. This experience definitely helped us in defining the anatomy of the pelvic autonomic nerves during L-NSRH.
The majority of patients with operable cervical carcinoma referred to our institute are with stage IIa disease and we perform non–nerve-sparing LRH with pelvic lymphadenectomy (LRH Pune Technique) 11 in these patients.
Our inclusion criteria for L-NSRH were only stage Ia2 and Ib1 disease. The disadvantage is that very few of our patients present with stage Ia2 and Ib1 disease, that is, with no parametrial involvement, which are the ideal indications of nerve sparing. We have presently not attempted L-NSRH in stage IIa. Various authors have established the feasibility of NSRH in stage IIa cervical cancers.2,4,5,16,22–24
Another drawback of L-NSRH is that it takes more time than conventional LRH. Our mean operative time is 88 minutes 11 for LRH and 160 minutes for L-NSRH.
Our pathological data revealed clear (negative) margins. The mean paracervical tissue margin was 3 cm, the mean breadth of poracolpos excised was 2.5 cm, and our average lymph node yield was 18 nodes.
Nerve-sparing techniques are also utilized in other pelvic surgeries. Possover et al. have performed laparoscopically assisted vaginal resection of rectovaginal endometriosis. 25 Landi et al. 26 have concluded that laparoscopic nerve-sparing complete excision of endometriosis seems to be feasible and offers good results in terms of bladder morbidity reduction.
We have successfully performed NSRH laparoscopically for early cervical carcinoma. Although this type of advanced laparoscopic procedure is associated with a steep learning curve, we have presented a reproducible technique, performed in comprehensible simple steps. The nerve-sparing technique performed laparoscopically can additionally be used in endometrial carcinoma. This technique of laparoscopic preservation of pelvic nerves also finds application in advanced endometriosis, where autonomic nerves are liable to be damaged.
Conclusion
Understanding this technique and the knowledge of laparoscopic anatomy of pelvic autonomic nerves are important to the surgeon and gynecologist in both benign and malignant pelvic surgeries. Nerve sparing is easier done laparoscopically and its results are comparable to that of conventional LRH in terms of lateral margin status and lymph node yield. Whether quality of life can be benefited by L-NRSH technique and its long-term oncological sequelae need further evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist.