
Abstract
Abstract
Background:
The invasiveness of laparoscopic cholecystectomy was further minimized by reducing the number of incisions with the introduction of single-incision laparoscopic surgery (SILS) cholecystectomy. In order to solve the challanges posed by SILS cholecytectomy, an increasing number of techniques have been reported with the advent of new surgical instruments and refinements to existing technology. We describe, in this article, two new techniques that utilize existing instrumentations: an access and a retraction technique.
Methods:
A consecutive series of 23 selected patients with symptomatic cholelithiasis underwent SILS cholecystectomy from April 10, 2009 to August 12, 2009. The overall procedure was similar to SILS cholecystectomy described in the literature. Hovewer, the access technique, with small-size arthroscopy cannules, was used to overcome the technical difficulty resulting from the collision of large-size caps of the laparoscopy trocars, and the retraction technique with a tacker was used to suspend the fundus of the gallbladder without taking the risk of gallbladder perforation.
Results:
All patients were female, and the mean age was 34 years (range, 27–65). The body mass index of all patients was below 30 kg/m2. The use of arthroscopy cannules provided a wider range of movement, and the retraction of the gallbladder was achieved safely with the tacker. These techniques reduced the operative times considerably.
Conclusions:
Most of the challanges posed by SILS cholecystectomy can be easily solved with simple technical modifications.
Introduction
SILS cholecystectomy was described as early as 1997 by Navara et al. 5 and, later, by Piskun and Rajpal. 6 For the stabilization of gallbladder, they used additional suspension sutures, and this innovation has now been applied to a wide variety of operations. 2 Hovewer, the main disadvantage of SILS is the restricted degrees of freedom of movement caused by the proximity of the instruments to each other during an operation. To overcome this problem, different surgical devices have been introduced, including access ports, small-profile trocars, a flexible endoscope, and instruments that provide angulations.1,7,8 In addition to this, the SILS cholecystectomy has been able to be performed with refinements to the existing technology.8,9
In this article, we report our initial experience in SILS cholecytectomy, with a detailed description of the new techniques, including the tack application for the suspension of gallbladder and use of small-size arthroscopy cannules to avoid clashing of the ports during the procedure. Familarity with this new approach was easily achieved, as LC is commonly performed in our instutitions.
Methods
Patients
From April 10, 2009 to August 12, 2009, a consecutive series of 23 selected patients with symptomatic cholelithiasis were prepared for an elective cholecystectomy. None of the patients had documented common bile duct stones on preoperative workup. Patients with complicated gallbladder disease were excluded from the study. Written consent was obtained from all patients after they were informed, concerning surgical technique, morbidities of laparoscopic surgery, and possible conversion to standard laparoscopic and/or open surgery. All patients were female, and the mean age was 34 years (range, 27–65). The body mass index of all patients was below 30 kg/m2. Two patients were in the early postpartum period. All operations were performed by the same surgeon (ME) in Istanbul University Cerrahpasa Medical School and Acibadem Kozyatagi Hospital (Istanbul, Turkey).
Operative technique
After the induction of general anesthesia, a single dose of cephalosporine was administered, and a nasogastric tube was placed. Patients were placed in the supine position with the operating surgeon on the patients' left and the assistant on the right. To perform a multiport technique in the first 21 cases, a 2-cm curvilinear skin incision was made, just below the umblicus, and the fascia was exposed. A Veress needle was inserted into the abdominal cavity, and carbon-dioxide (CO2) gas was insufflated to a pressure of 12 mm Hg. Three 5-mm trocars were placed into the peritoneal cavity, using three separate fascial sites. In the first 2 cases, clashing of the large-size caps of the laparoscopy trocars with one another resulted in technical difficulties during the procedures. In order to overcome this problem, we used two 5-mm small-size, single-use arthroscopy cannules (Arthrex, Naples, FL) (Fig. 1) and one 5-mm laparoscopy trocar for insufflation in the following 19 patients. The trocars were placed in a way that each port was positioned at the corners of an imaginary triangle, with its apex located superiorly. A 5-mm blunt-tip optical-viewing laparoscopy trocar was inserted at the apex, and the other two arthroscopy cannules were inserted at the other two corners of this triangle. To perform the single-port technique in the last 2 patients, an open approach, consisting of a 2-cm intraumblical vertical skin incision and fasciotomy, were made to place the SilsPort™ (Covidien, Bedford, MA) into the abdomen and the pneumoperitoneum was established.
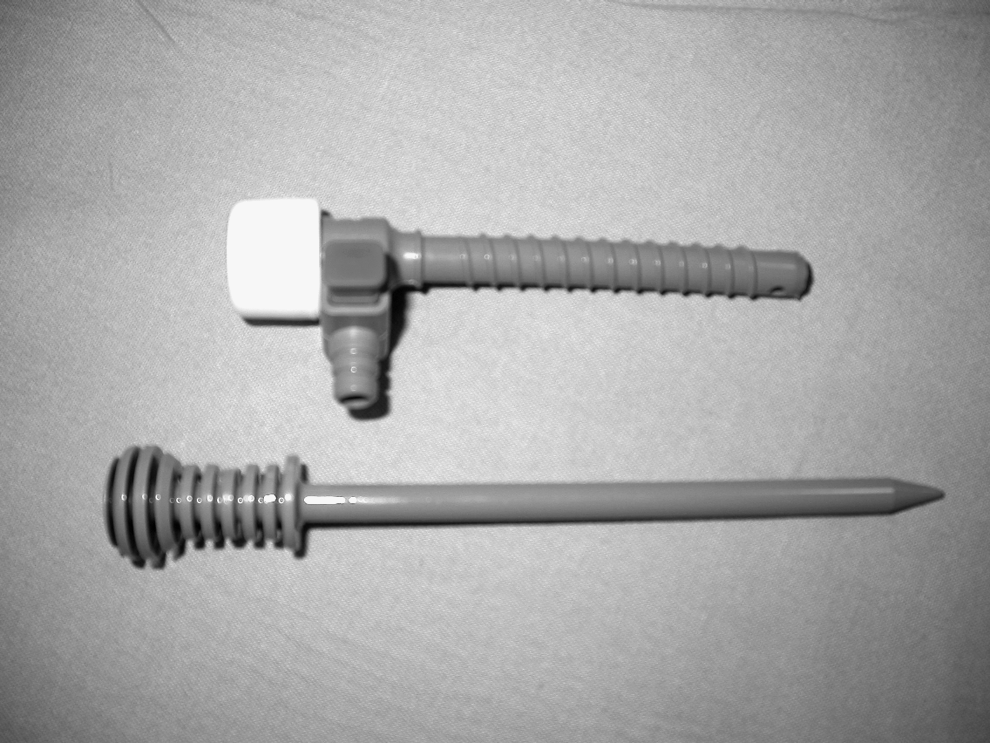
Single-use arthroscopy cannule (Arthrex, Naples, FL).
Following the exploration of the abdominal cavity, patients were placed in a reverse Trendelenburg position and rotated slightly to the left. The retraction of the fundus of the gallbladder was achieved by two techniques: suturing (18 patients) and tacking (5 patients). In the first 5 cases, a 2-0 atraumatic polyprolene suture, on a Keith needle, was inserted through the abdominal wall below the 10th rib at the midclavicular line. The needle was then grasped in the abdomen, placed through the fundus of the gallbladder, and then returned through the abdominal wall near the insertion side. The fundus was lifted up to the anterior abdominal wall to expose Hartmann's pouch. However, exposure with this technique was not satisfactory. So, the insertion side of the needle was changed to the 8th or 9th intercostal space, depending on the anatomy. In the tacking technique (Fig. 2A and B), the fundus of the gallbladder was lifted up with a grasper (Roticulator Endo Grasp, 5 mm; Covidien) and tacked to the anterior abdominal wall with a tack (ProTack®; TycoUSS, Norwalk, CT). Dissection of the gallbladder was performed in a infundibulum-to-fundal fashion. To expose the Calot's triangle, Hartmann's pouch was grasped and retracted laterally and slightly upward with a roticulating grasper. Dissection of the cytstic duct and then the cystic artery were completed with a hook monopolar cautery and then with a roticulating dissector (Roticulator EndoDissect, 5 mm; Covidien). Once these structures were clearly in view, the cystic duct and artery were clipped and divided. The gallbladder was dissected free off the liver bed with hook cautery. The suspended gallbladder was detached from the abdominal wall by either cutting the sling suture extracorporally or removing the tack intracorporally. In the multiport technique, two working ports were replaced by a 10-mm trocar and the gallbadder was extracted with a bag (EndoCatch Gold, 10 mm; Covidien). In the single-port technique, the specimen was extracted along with the SilsPort system. After meticulous hemostasis, no drain was left in place. The fascial defect and skin were closed with 2-0 nonabsorbable and subcuticular 4-0 absorbable sutures, respectively.
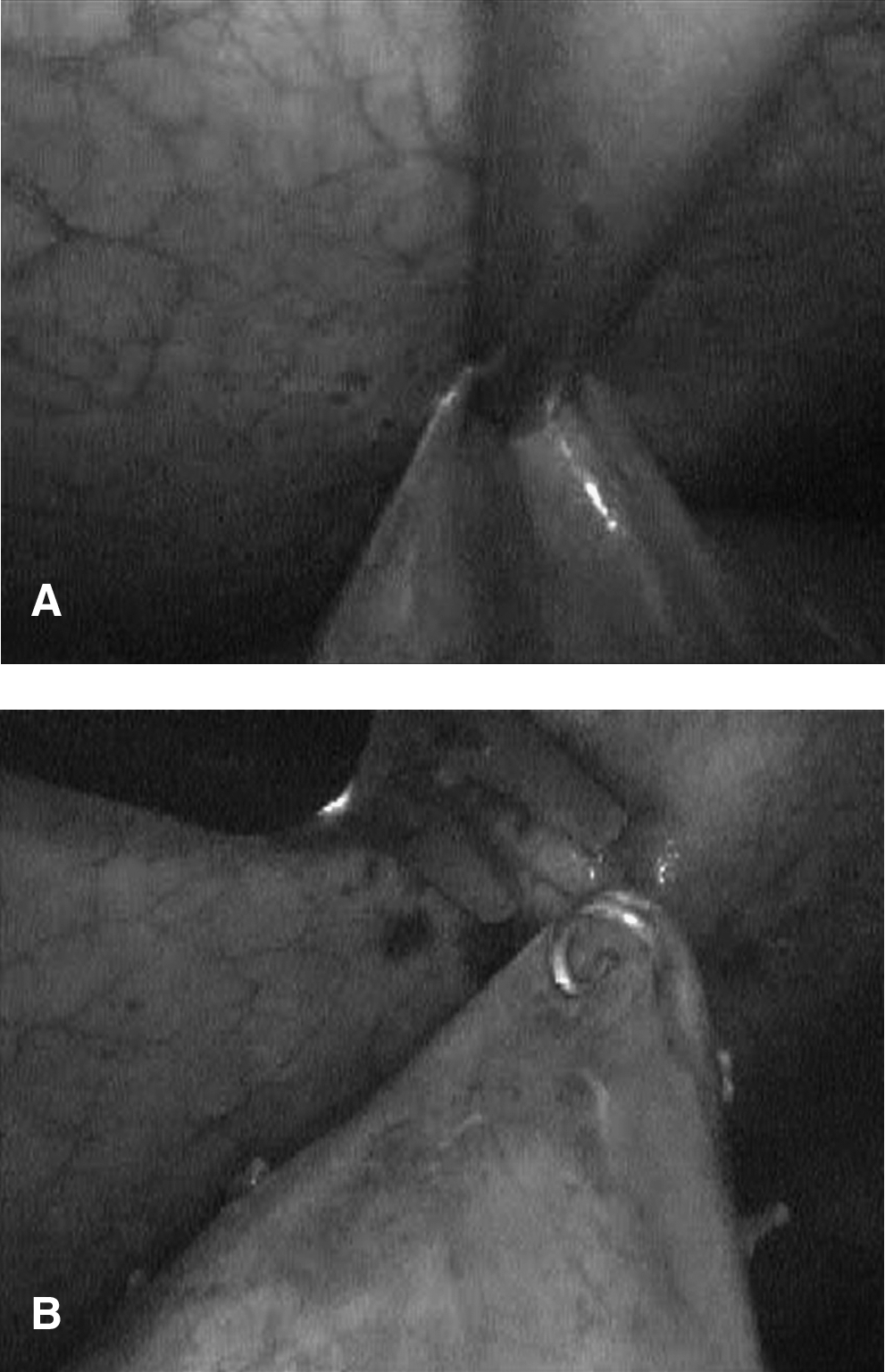
Approximation of the fundus of the gallbladder to the abdominal wall (
Results
All operations were succesfully completed. No procedures required any extraumblical skin incision for additional trocars or conversion to a standard laparoscopy or open surgery. The mean operative time was 46 minutes. The operative times in the first 2 cases were longer (90 and 80 minutes) due to the technical difficulty that resulted from the collision of the caps of the laparoscopy trocars. The shortest operative times were observed in the five operations where the fundus of the gallbladder was suspended to the abdominal wall with a tack (mean, 41 minutes). Blood loss was minimal in all cases. Neither perforation of the gallbladder nor biliary injuries happened in any case. During the postoperative period, all patients were mobilized within 4 hours, were allowed to feed orally within 6 hours, and discharged within 18 hours of hospitalization. Patients were seen in the out-patient clinic 7 days after surgery. No postoperative complications were observed.
Discussion
SILS cholecyetectomy was already reported in the literature more than a decade ago,5,6 but did not gain widespread use due to the technical difficulties. With the advent of new surgical instruments and refinements of existing technology, scattered articles have been reported in the literature concerning different methods to overcome these difficulties.1,4,7–9 Compared to standard cholecystectomy with four trocars, one of the major challenges posed by SILS is the limited range of motion. This can be remedied, in part, with the use of small-profile trocars. In our experience, with the first 2 cases, collision of the caps of the laparoscopy trocars further made the procedure difficult, even though we used end-articulating instruments. A simple modification of the two working trocars with the small-size arthroscopy cannules enabled us a wider range of movement and reduced operative times considerably in the following operations. As an advantage, these cannules also have small-size stopcocks, which were used for the evacuation of smoke created by the use of monopolar electrocautery. This issue was also reported by Hong et al. 3 and Romanelli et al., 10 who used a single-port system that had no venting for the evacuation of the smoke. The arthroscopy cannules are also cheaper than the laparoscopy trocars.
Retraction of the fundus of the gallbladder is an important step in order to delineate the anatomy of Callot's triangle adequately. This is also simply performed through the fourth trocar in our routine standard laparoscopy practice. However, SILS cholecytectomy has necessitated the need for different approaches for the retraction of the gallbladder. Several techniques have been described regarding retraction techniques. Three transabdominal stay sutures were placed in the first SILS cholecystectomy in 1997 by Navara et al., 5 and later, a two-suture technique was introduced by Piskun and Rajpal. 6 The retraction-stitch technique has become a common approach, as it has minimized additional gallbladder retraction. However, this required additional punctures through the abdominal wall. Elazary et al. 1 introduced a different method of transabdominal anchoring of the gallbladder's fundus by using an endoloop, together with retraction of Hartmann's pouch, with a flexible endoscopic dissector in pigs. In the majority of patients, we performed the retraction-stitch technique with a single suture. A similar technique with one sling suture was previously reported by Ersin et al. 11 We experienced that exposure with this technique was not satisfactory when the suture was placed in subcostal region in the first 5 patients. So, the insertion side of the needle was changed to the 8th or 9th intercostal space, depending on the anatomy. Chamberlain et al. 2 criticized the sling-suture method for the increased risk of gallbladder perforation, leading to elevated risk of bile peritonitis. With this idea in mind, we developed a technique, the “tack technique,” which utilizes a tacker to suspend the gallbladder as was done in our 5 selected patients. We recommend this technique in cases where the fundus of the gallbladder is approximately 2 cm away from the liver edge and with the absence of a fragile gallbladder wall due to cholecystitis. One tack was adequate, and no bile leak was observed in all of these patients. Operative times were considerably reduced. To our knowledge, this method has not been reported, to date. We believe that surgeons who are performing SILS cholectectomy can benefit significantly from this tack technique. The operative times in our first 2 cases were 80 and 90 minutes, respectively. With the help of the aforementioned technical evolution through this series, the overall operative times were reduced considerably, with a mean of 46 minutes. Taking into account the differences in the technical aspects of the previously published studies, the mean operative time in our series was notably shorter than the 55 minutes reported by Tacchino et al., 9 the 72 minutes by Hodgett et al., 4 79 minutes by Hong et al., 3 94 minutes by Ersin et al., 11 and 154 minutes by Afthinos et al. 8
Conclusions
SILS holds a promise as an innovative approach in the field of minimally invasive surgery. Based on our experience with the selected group of patients, most of the challenges posed by SILS can easily be solved with the advancement of new surgical instruments and refinements to the existing technology.
Footnotes
Disclosure Statement
No competing financial interests exist.