
Abstract
Abstract
Embryonic–natural orifice transumbilical endoscopic surgery is currently used for adnexectomy or hysterectomy. Embryonic–natural orifice transumbilical endoscopic surgery for myomectomy with traction of two directional sutures in a 32-year-old woman enabled the minimal surgical approach for myomectomy and efficient and safe morcellation and retrieving of myoma. This novel surgical approach could be used as part of minimal surgery in the surgical management of myoma.
Introduction
During single-port surgery or embryonic NOTES (E-NOTES) via an umbilicus, handling of myoma into different directions could be quite a big challenge. Fortunately, myoma is enough hard to pull with string and has a tendency not to rupture during manipulation of these strings. These concepts lead to traction of anchoring sutures during E-NOTES for myomectomy applied in the current case. Safe morcellation could be guaranteed, because direction morcellation via an umbilicus is possible in an endobag.
Surgical Technique
A 32-year-old woman had lower abdominal discomfort and dysmenorrhea caused by myoma. She was healthy but had transient and mild dermographism. At pelvic examination, uterine myoma was palpated on the posterior and lower uterine wall. Transvaginal sonography revealed a 7.2 cm sized myoma at the posterior cervix (Fig. 1). Recently, papillary thyroid cancer was identified in neck mass. She wanted to remove the myoma at the same time of the thyroidectomy.
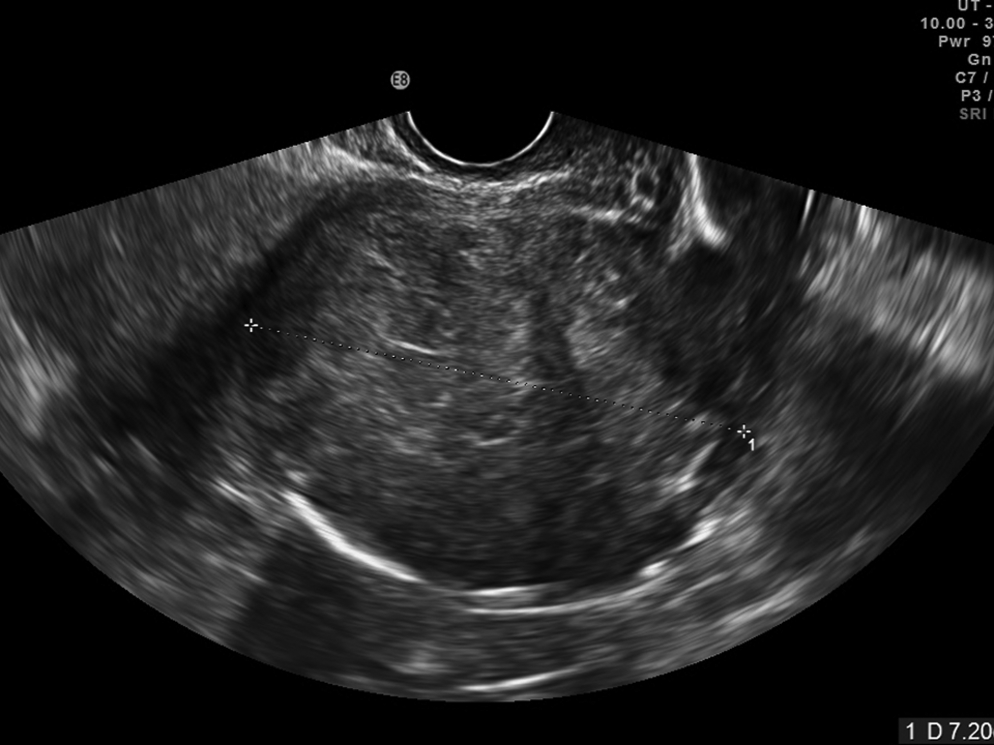
Transvaginal sonography showing a 7.2 cm sized myoma in posterior and lower part of the uterus.
She strongly desired to remove the myoma with conservation of the uterus. Treatment strategies for myomectomy such as mini-laparotomy, conventional laparoscopy, and E-NOTES were discussed with the patient. Finally, E-NOTES was selected because of the cosmesis and possibility of less postoperative pain.
The patient was positioned in the supine position with the leg extended and prepped and draped in an out routine sterile fashion. 5 The legs were protected with foam padding. At the start of surgery, a 2.5 cm intraumblical incision was made. The incision was larger than that in a previous report dealing with adnexal tumors for effective morcellation of myoma. 5 The single-port system was made as previously mentioned, by using a wound protractor (Alexis® X-small for 2–4 cm incisions; Applied Medical and a surgical glove (TriflexLP, 7-0; Cardinal Health). 5 Carbon dioxide was insufflated to maintain the intra-abdominal pressure at 12 mmHg. Only one 5 mm trocar was replaced in the finger portion of the glove for frequently changeable laparoscopic instruments (Fig. 2). A camera and a holding grasper were inserted into small incisions directly in the finger portion of the surgical glove without application of trocars.
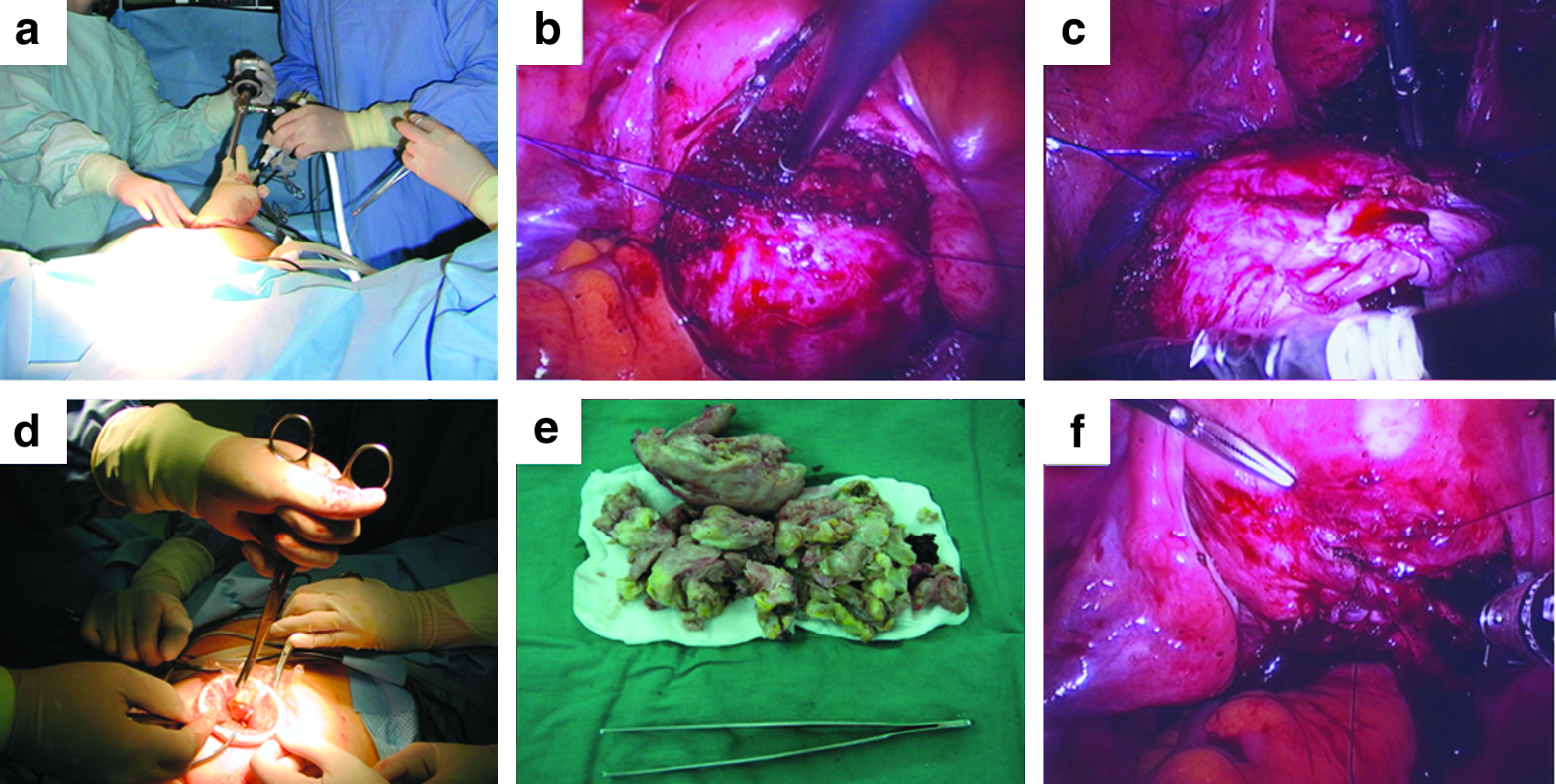
Surgical procedures for embryonic-natural orifice transumblical endoscopic surgery (E-NOTES) for myomectomy.
After incision of a serosa covering the posterior myoma, the protruded myoma was sutured with a polypropylene monofilament with a 70 mm double straight taper needle (2/0 Prolene W8400, Ethicon, JJMEDCAL GmbH), which was directly inserted into the pelvic cavity using a needle holder and was returned outside the body using a laparoscopic needle holder at the right and left lower quadrants of the abdomen. Traction of the sutures enables easy exposure of the surgical plane between the myoma and uterus. A Roticulator (Covidien) was used for an additional manipulation of uterus. While the myoma was raised with traction of the sutures, the myoma was easily retrieved in the endobag (LapBag®, Sejong Medical). The myoma was directly morcellated via an umbilicus. The uterine wall was repaired using an Endo Stitch™ 10 mm (Covidien, AG). Operative time was 230 minutes. No intraoperative complication was identified, and the postoperative courses were uneventful.
Discussion
To the best of our knowledge, this is the first report of E-NOTES for myomectomy with traction of anchoring sutures. We believe that this surgical prototype can ensure facilitation of lesser invasive surgery with safe morcellation of the myoma at the same time (Fig. 3).
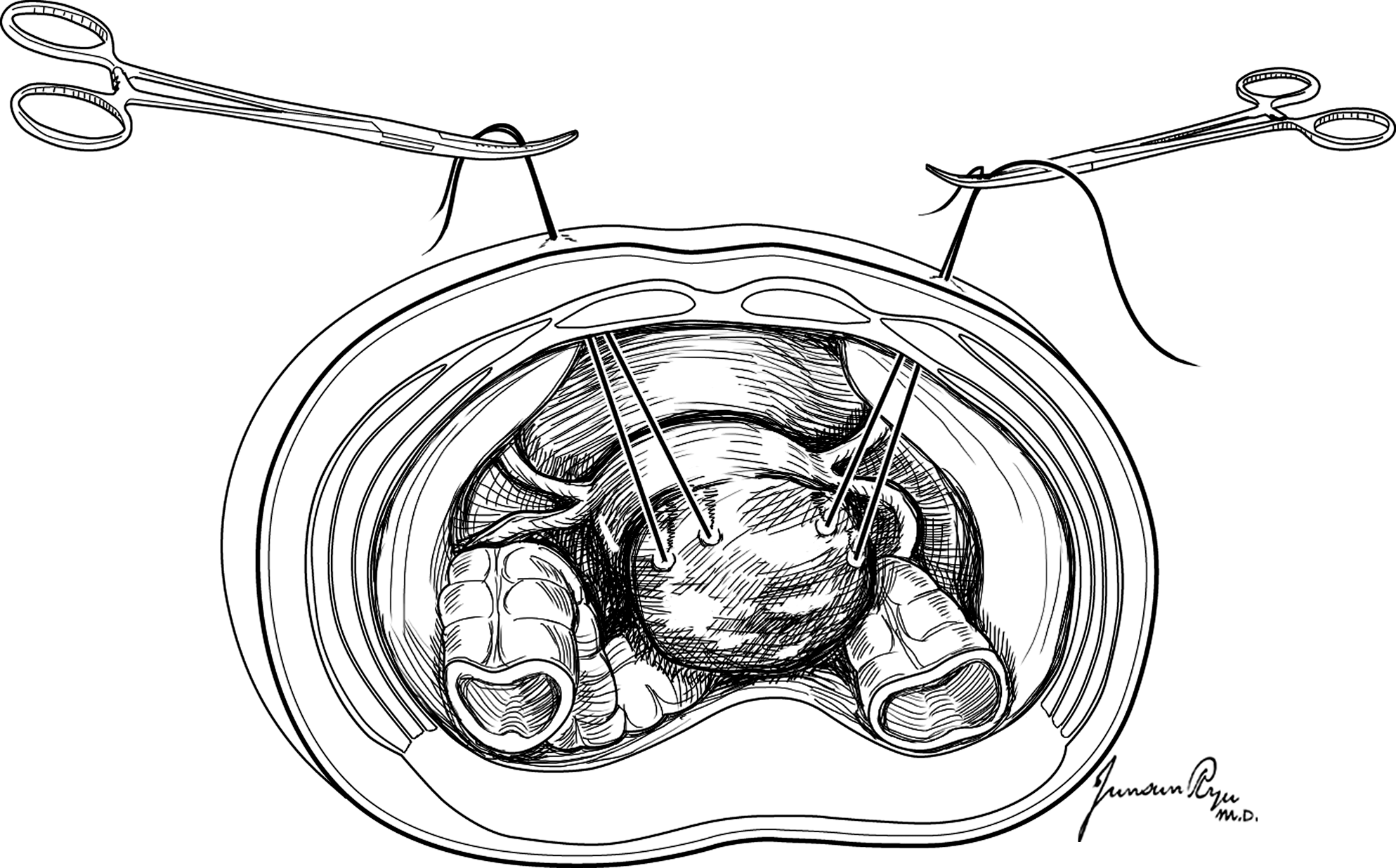
The multidirectional traction suture resulting in lesser pain, better cosmesis, no need of wound repair for trocar site, and easier grasping and traction of the myoma during E-NOTES for myomectomy.
The traction of anchoring sutures with E-NOTES proposes several advantages compared with conventional laparoscopic ports in terms of less pain, cosmesis, and no need of wound repair for trocar sites. The myoma is hard enough to be sutured and tracked by multiple anchoring sutures in several directions. The location of traction via an abdomen could be easily reassigned compared with fixed conventional laparoscopic ports. This secures a clear surgical view for E-NOTES myomectomy. Most of all, compared with conventional laparoscopy, grasping and traction of myoma is easier, because strong grip is not required.
Laparoscopic morcellation has a chance of peritoneal seeding of undiagnosed leiomyosarcoma. 4 During conventional laparoscopy, myoma is morcellated in the uncovered peritoneum. In the current case, morcellation in a laparoscopic bag seems to be potentially safer than conventional laparoscopic morcellation in uncovered peritoneum. Intraoperative cutting of leiomyosarcoma including myomectomy is suggested to be related with a worse prognosis than intact removal of leiomyosarcoma such as total hysterectomy. 4 Therefore, intact tumor removal of leiomyoma is important most of all, because most of leiomyosarcoma are diagnosed during postoperative pathological examination. Easier and faster retrieval is possible via a larger surgical incision in E-NOTES compared with conventional laparoscopy (4.9 cm2 versus 1.1 cm2 in 2.5-cm skin incisions compared with 1.2-cm skin incisions, respectively). 5
E-NOTES could be popularly performed with development of more intuitive and ergonomic surgical instruments including camera system, port system, laparoscopic instruments for holding, cutting, and coagulating, and strings. Currently available new surgical instruments such as a flexible scope with a long shaft, a bidirectional barbed suture, and an absorbable suture such as a LapraTy may facilitate E-NOTES.
Dr. Kikuchi reported the usefulness of a flexible scope to minimize extra-corporeal and intracorporeal clashing with rigid straight forceps. 6 The flexible scope provides an adequate surgical field without reference to the angle of insertion. 6 Dr. Einarsson reported E-NOTES myomectomy and unique surgical string for the first time. 2 A 5 mm bronchoscope with a 30-degree optic was used to avoid crowding among hand grips of laparoscopic surgical instruments and camera head. A 14 × 14 cm O-polydioxanone (O PDO) bidirectional barbed suture facilitates myometrial closure because of no back-sliding of the suture. Dr. Einarsson insisted that even distribution of tensile strength through the myometrial repair and no need of knotting trying are advantages in E-NOTES myomectomy. Laparoscopic knot tying after sutures is one of the most challenging kinds during myomectomy. An absorbable clip is widely alternative to intracorporeal tying during partial nephrectomy. 7 An absorbable clip that is made of biocompatible polydioxanone polymer (LapraTy; Ethicon Endosurgery) could be one of the examples to substitute intra- or extracorporeal suture during myomectomy. 7 Safeness and efficiency of the LapraTy instead of knotting during cavotomy, small bowel enterotomy with repair, partial nephrectomy, and cystotomy have been reported in a porcine model. 8 In the gynecologic field, LapryTy could be potentially used in reconstructive procedures such as myomectomy repair, vaginal stump repair, or peritoneal approximation after para-aortic lymph node dissection.
Several innate limitations of E-NOTES such as loss of triangulation, inappropriate instruments, limited visualization, and familiarity of surgeons with the procedures still remain to be solved. 9 Rising cost owing to use of new disposable articulating instruments could be one of the potential barriers for popular use of E-NOTES. A new surgical approach should be developed for secure myometrial repair during E-NOTES comparable to laparotomic procedures. Although the potential benefit in terms of cosmetic outcomes was suggested, the benefit of E-NOTES over conventional laparoscopic surgery is not definitively estimated. 2
Currently, we are facing new and various problems related to E-NOTES. The challenge we meet during E-NOTES have to be solved by developing novel applications of more intuitive and ergonomic instruments continuously. We believe that our trial is potentially applicable to selected patients with myoma. A well-designed prospective study on this issue is required before an introduction to routine surgical practice.
Disclosure Statement
No competing financial interests exist.