
Abstract
Abstract
Objective:
To describe the technique and report patient outcomes of a left lateral approach for robotic transperitoneal infrarenal aortic lymphadenectomy with subsequent pelvic surgery in patients with gynecologic malignancy.
Methods:
Outcome data were collected retrospectively from March 2009 to September 2010 for all patients undergoing a left lateral approach for robotic transperitoneal aortic lymphadenectomy using a right lateral decubitus position by a single surgeon. Outcomes were analyzed and compared.
Results:
The median total operating time was 213 minutes (range, 186–265). The median body mass index was 25.2 kg/m2 (range, 22.5–32.1). The median estimated blood loss was 150 mL (range, 50–550). The median length of hospital stay was 1 day (range, 1–2). The mean number of para-aortic lymph nodes was 8.2 (range 4–17). There were no conversions or perioperative complications in this 5-patient series. The mean follow-up was 12.8 months (range, 8–20). All patients underwent concomitant robotic hysterectomy and pelvic lymphadenectomy.
Conclusions:
A left lateral approach for robotic transperitoneal infrarenal aortic lymphadenectomy using a right lateral decubitus position is safe and feasible. Minimal patient repositioning provides access for pelvic surgery using the same abdominal trocar placement.
Introduction
Endometrial carcinoma is the most common gynecologic malignancy in the United States. Practice guidelines recommend surgical staging consisting of hysterectomy and bilateral salpingo-oophorectomy, with pelvic and/or aortic lymphadenectomy. The presence or absence of lymphatic spread influences the prognosis and adjuvant therapy. Prospective data from Mariani et al. demonstrated that para-aortic nodal involvement occurs in 67% of patients with lymphatic dissemination. Furthermore, 77% of patients with para-aortic node involvement had metastasis above the inferior mesenteric artery (IMA). 2
Exposing the aortic region via a minimally invasive approach can be challenging. This is particularly true of the infrarenal aorta, between the IMA and left renal vein. One drawback of the current da Vinci robotic system (Intuitive Surgical Inc, Sunnyvale, CA) is the limited ability to access the entire abdominal and pelvic cavity without relocating the robotic column. We previously described a technique for robotic transperitoneal infrarenal aortic lymphadenectomy that involved a 180° rotation of the operating table and additional trocar placement. 3 This technique requires a coordinated anesthesia, surgical, and perioperative team.
This study was designed to evaluate a left lateral approach for infrarenal aortic lymphadenectomy using a right lateral decubitus position with minimal patient repositioning to achieve an adequate pelvic and aortic dissection. The concept for this operative approach was gleaned from our urology colleagues who utilize this novel patient position for laparoscopic renal surgery. Martin et al. reported on over 1240 cases utilizing this method without any adverse events secondary to positioning. 4 We describe our initial experience utilizing a right lateral decubitus position to provide upper abdominal access robotically.
Materials and Methods
A left lateral approach for robotic transperitoneal infrarenal aortic lymphadenectomy using a right lateral decubitus position was used for 5 patients between March 2009 to March 2010 at the Mayo Clinic in Arizona. All patients had known endometrial carcinoma with suspected risk factors indicating aortic lymphadenectomy (i.e., myometrial invasion >50%, large tumor diameter, and grade 3 or nonendometrioid pathology). Patient data were collected retrospectively and included patient age, body mass index (BMI), tumor grade and diameter, blood loss, co-morbidities, total operative time (abdominal and pelvic dissections), length of hospital stay, intraoperative and postoperative complications, pathology, lymph node count and status, and follow-up. Approval was obtained by the institutional review board.
Patients were positioned on the operating table as described by Martin et al. with a slight modification. 4 The patient rested supine atop an underlying antiskid material with a 10-pound sand bag bump placed under the left flank. The left arm was supported, padded, and tucked to the left side. The right arm was secured and extended outward on an arm board. The legs were slightly flexed at the knees with pillow support and a pillow between the knees. The torso, hips, and knees were secured with padding and tape, allowing for extreme rotation of the table to the right exposing the patient's left flank. Allen stirrups were secured and rotated beneath the table so that they could be rotated outward for placement of the patient's legs when the pelvic portion of the procedure ensued. The security of the patient was verified by carefully rotating the patient into extreme right tilt before surgical preparation and draping (Fig. 1).
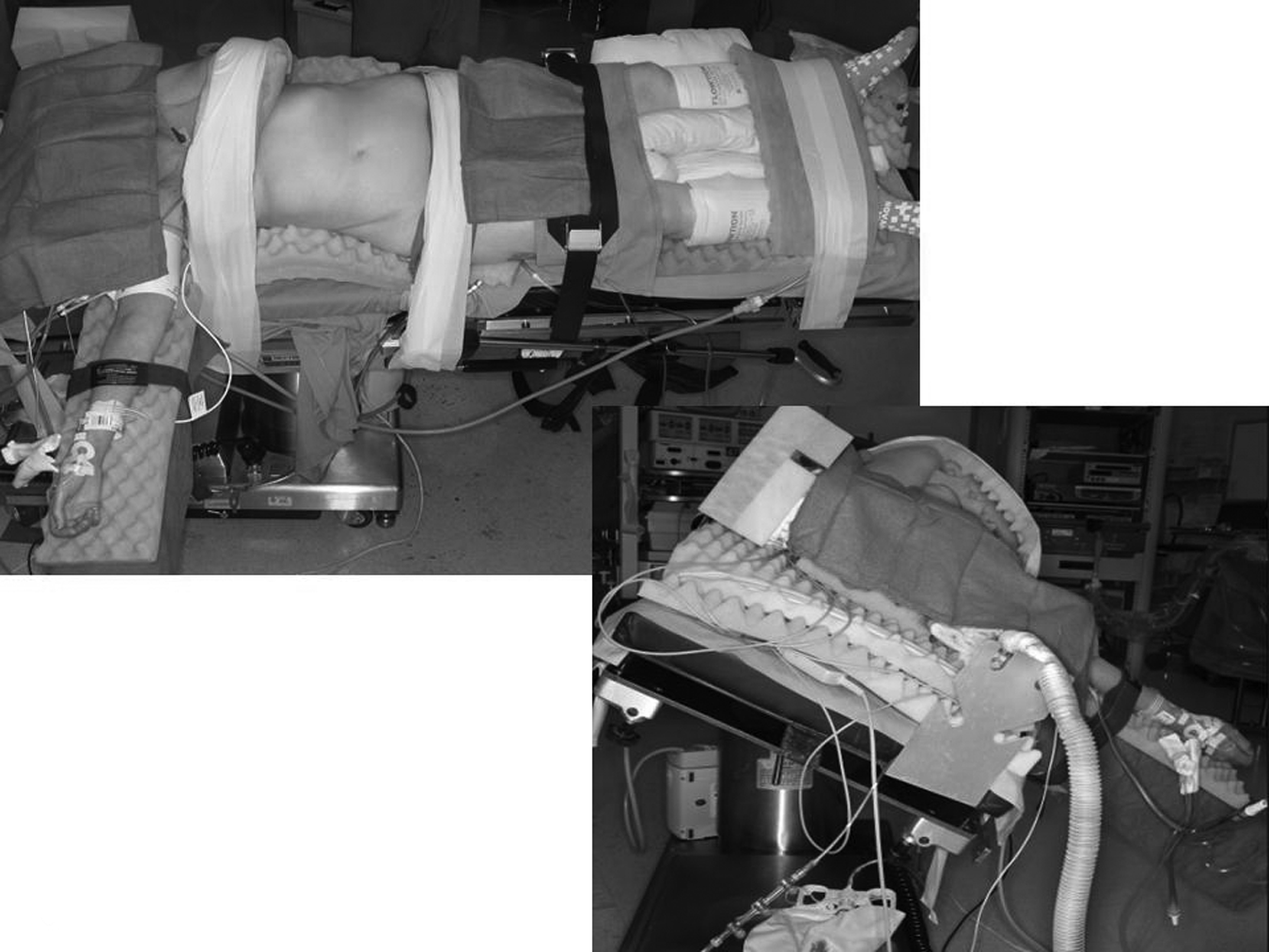
Patient positioning: View from the patient's right side (left); view from head of right lateral table tilt (right).
A 12-mm trocar was inserted at the umbilicus. Assessment of the entire abdomino-pelvic cavity was performed assessing for any evidence of gross metastatic disease. Ancillary trocars were placed with the patient in the supine position as follows (Figs. 2 and 3): (1) A 12-mm trocar at the left mid-clavicular line 3–4 cephalad to the umbilicus. This port housed the 0° robotic camera. (2) An 8-mm robotic trocar placed 2 cm left of midline just below the costal margin. (3) A 8-mm robotic trocar 4 cm above the pubic symphysis and 2 cm left of midline. (4) A 5-mm bladeless trocar placed 10 cm left lateral of the umbilicus for the assistant. The patient was then placed in extreme right lateral decubitus and the da Vinci S robotic system docked over the patients left hip at a 60° angle to the legs. Robotic EndoWrist (Intuitive Surgical) instrumentation included a fenestrated bipolar grasper on the left and monopolar scissors on the right. The assistant sat on the right side of the patient and provided tissue retraction, clip application, vessel-sealing, and suction/irrigation via the umbilical and the left lateral trocar.
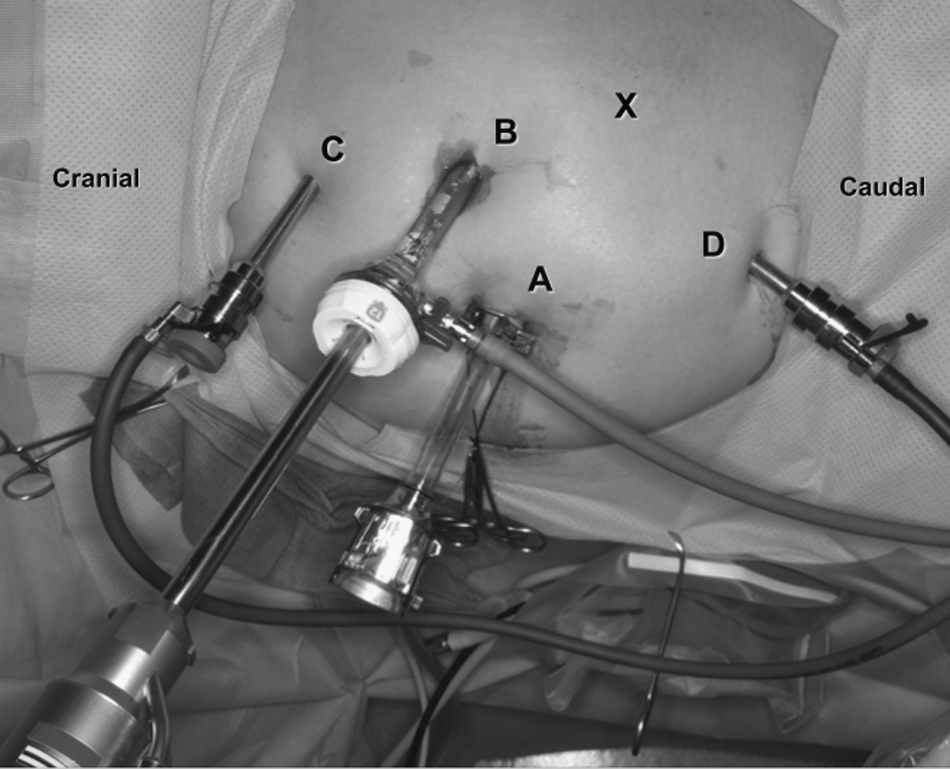
Trocar placement for aortic dissection while in right lateral decubitus position: (A) Umbilical assistant port; (B) Left midclavicular, robotic camera; (C) Subcostal robotic left arm; (D) Suprapubic robotic right arm; (X) Left lateral assistant port, later used as robotic left arm for pelvic dissection.
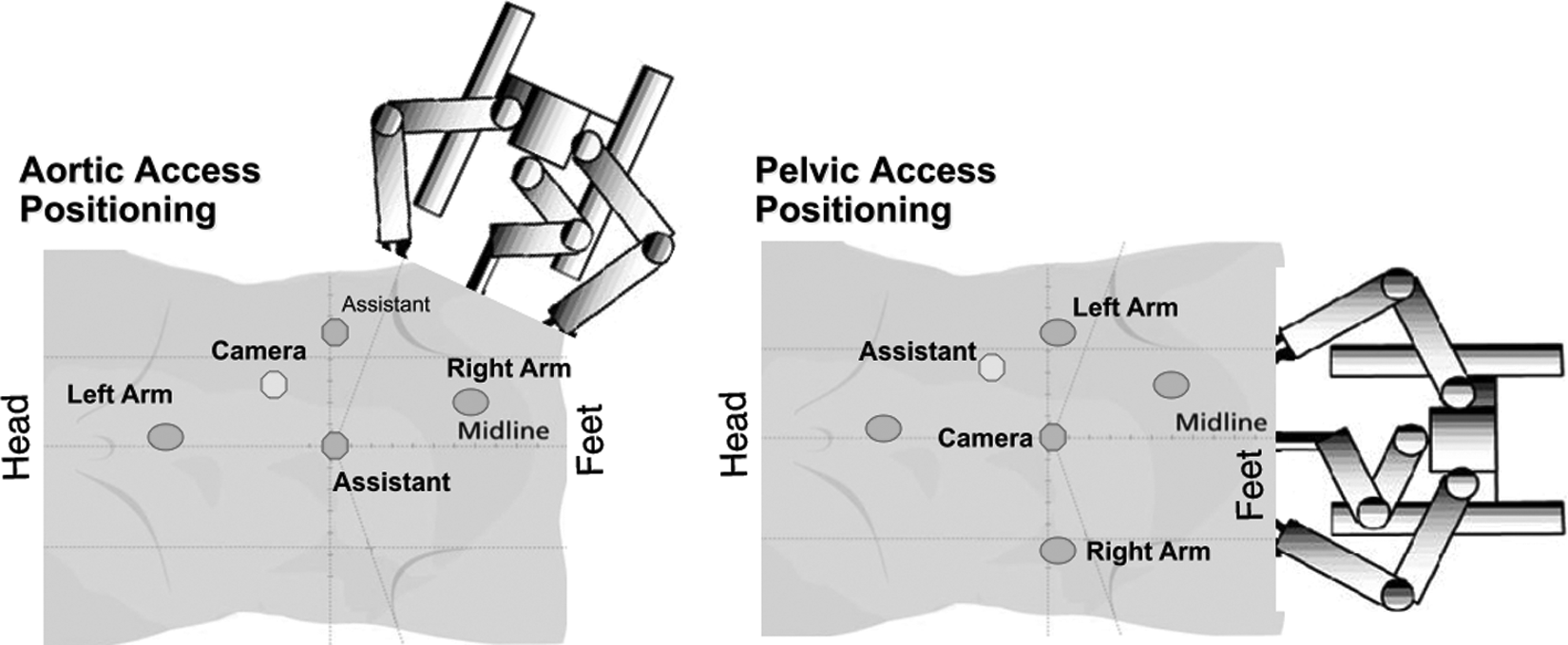
Aortic and pelvic access: Trocar, patient, and robotic column positioning.
The infrarenal aortic lymphadenectomy was performed first due to complications or technical difficulties of this portion of the procedure being the most likely to require conversion to laparotomy. The white line of Toldt was incised from the pelvic brim to the splenic flexure to mobilize the descending colon medially exposing the aortic nodes. Gravity directed the colon out of the operative field. Peritoneum overlying the psoas muscle was elevated and the left ureter isolated and mobilized laterally. The left gonadal vein was transected distally and dissected cephalad to its insertion into the renal vein. Endoscopic clips were applied at the insertion into the left renal vein that delineated the most cephalad border of the aortic lymphadenectomy. The nodal dissection was started at the mid left common iliac artery and continued cephalad removing all nodal tissue anterior and lateral to the aorta up to the left renal vein. The right aortic nodes were removed from the mid-right common iliac artery to the insertion of the right gonadal vein at the inferior vena cava, the cephalad border of the right lymphadenectomy. Division of the IMA was occasionally necessary to obtain adequate exposure and accessibility to underlying lymphatics.
Once the aortic lymphadenectomy was completed, the robotic system was undocked. The patient was positioned supine, sand bag removed, Allen stirrups rotated outward, and the legs positioned in the standard low dorsal lithotomy position. The operating table was rotated 45° and the patient placed in steep Trendelenburg. This was accomplished without removing the sterile drapes. One additional 8-mm trocar was inserted 10 cm to the right of the umbilical port for the right robotic arm. The left 5-mm trocar was converted to an 8-mm trocar for the left robotic arm and the robotic system docked caudally between the legs. The camera was advanced transumbilically and the left mid-clavicular port was used for the assistant. A hysterectomy, salpingo-oophorectomy, with pelvic lymphadenectomy was performed as customary. A total of six trocars were used for both the dissection of the aortic lymphadenectomy as well as the pelvic dissections.
Results
All five operations were completed with the robotic surgical system without conversion. All patients tolerated the procedure and positioning well, and none required readmission or reoperation in the 6-week perioperative period. The median patient age was 67 years (range, 61–75). Five patients underwent concomitant robotic pelvic lymphadenectomy and hysterectomy. The median total operating time was 213 minutes (range, 186–265). The median body mass index was 25.2 kg/m2 (range, 22.5–32.1). The median estimated blood loss was 150 mL (range, 50–550). No blood transfusions occurred. The median length of hospital stay was 1 day (range, 1–2). There were no conversions or perioperative complications in this 5 patient series.
The mean number of para-aortic lymph nodes was 8.2 (range 4–17). The mean number of pelvic lymph nodes was 13 (range, 10–21). Five patients had uterine malignancies: 4 endometrioid adenocarcinomas and 1 mixed mesodermal tumor. Positive aortic nodes were detected in 1 patient with endometrial cancer, notably having absent pelvic nodal disease.
There were no early postoperative complications (<42 days). Late complications (>42 days) included 1 patient with chylous ascites who responded to conservative management, and 1 patient who required an umbilical trocar site hernia repair 8 months after surgery. The follow-up of all patients continued on an outpatient basis in our department (mean 12.8 months, range 8–20).
Discussion
We describe a novel technique of robotic transperitoneal infrarenal aortic lymphadenectomy and concomitant pelvic surgery utilizing patient lateral rotation, efficient trocar placement, and minimal adjustment in the location of the robotic column. Our new technique uses six abdominal trocars total for pelvic and upper abdominal dissection. The left lateral approach with medial mobilization of the descending colon provides exposure of bilateral infrarenal aortic regions. The patient is rotated 60° and the robot is docked caudally for pelvic dissection. Further development of our technique, following this patient series, revealed that the pelvic dissection (including lymphadenectomy) may also be carried out without patient rotation using a left lateral sided docking approach.
We have previously described an approach of transperitoneal infrarenal aortic lymphadenectomy involving a 180° rotation of the patient when proceeding from the pelvic to aortic dissection. 3 Although this technique has been very successful, it has the disadvantages of requiring the placement several additional trocars and a well-trained, rehearsed surgical team. Our perioperative complications and postoperative outcomes were similar to previous robotic and laparoscopic aortic dissection reports. The mean BMI in this series is 25.2 kg/m2 as a result of selection bias during the experimentation phase of technique design. We now plan to proceed with more women with gynecologic malignancies.
It is our opinion that aortic lymphadenectomy in patients with endometrial cancer should include dissection to the level of the left renal vein. Reports that address the routes of lymphatic dissemination suggest that although the principal connections are between the uterine corpus and the external iliac and obturator basins, a direct route may exist from the corpus to the aortic node-bearing basins. This is thought to occur via the lymphatic channels adjacent to the gonadal vessels within the infundibulopelvic ligament. 5 Mariani et al. support this theory and noted that 77% of patients with para-aortic involvement had metastasis above the IMA, whereas para-aortic nodes below the IMA were not involved in 60% of patients. Hence, if an aortic lymphadenectomy is to be performed, it should include a bilateral resection of the aortic nodes between the IMA and renal vein. 2
Robotic technology is ideal for complex dissection near the great vessels providing enhanced observation, stability, and precise ergonomic control. Data from the GOG LAP 2 Study demonstrated a 25% conversion rate from laparoscopy to laparotomy in a population of patients surgically staged for carcinoma of the uterine corpus. 6 This high rate of conversion is a testament to some of the inherent difficulties associated with traditional laparoscopic surgery. Hence, many gynecologic oncologists are embracing robotic technology as a means of offering more patients a minimally invasive approach to their operative procedure. 1 A problem, however, remains with the current robotic system in that the surgeon is limited to essentially two quadrants of the abdomino-pelvic cavity. This can be circumvented by patient rotation or by relocation of the robotic column. This, however, is time consuming and requires a well-trained surgical and anesthesia team. While formulation of our technique continues to evolve, our initial experience confirms the feasibility and safety of a left lateral approach for transperitoneal infrarenal aortic lymphadenectomy using a right lateral decubitus position.
Authors' Contributions
All of the authors contributed to the development of the surgical technique described herein. All authors were actively involved in maintaining patient safety, data collection, and article formulation.
Footnotes
Disclosure Statement
No competing financial interests exist.