
Abstract
Abstract
Purpose:
The aim of this study was to evaluate outcome of patients with congenital diaphragmatic hernia (CDH) undergoing open versus minimally invasive surgery.
Subjects and Methods:
Patient records of 33 children undergoing surgery for CDH between March 2002 and September 2008 were reviewed. Patient data were compared regarding operating time, intraoperative maximum CO2 partial pressure (pCO2max) values, postoperative ventilation time, complications, and recurrences.
Results:
Median age at time of operation was 4 days (range, 0–1017 days), and median weight was 3800 g (range, 2000–13,200 g). Laparotomy was performed in 12 children. Seventeen patients underwent thoracoscopic repair, and four children had a laparoscopic approach. Operating time was significantly longer (P=.004) in the minimally invasive group. Median values of pCO2max during operation were not significantly different (P=.25) in the minimally invasive surgery group. The pCO2max values in the postoperative course were significantly lower (P=.013) in the minimally invasive group, whereas median ventilation times postoperatively were significantly longer (P=.024) in the open surgery group.
Conclusions:
Median values of pCO2max in the postoperative course were significantly lower in the minimally invasive surgery group. In addition, postoperative ventilation time was shorter when children underwent minimally invasive surgery. In conclusion, minimally invasive surgery seems to offer advantages for selected patients with CDH.
Introduction

Setting and trocar positioning for thoracoscopic repair of congenital diaphragmatic hernia in a newborn.
Patients and Methods
Patient data
Patient records of 33 children undergoing surgery for CDH between March 2002 and 2009 were reviewed retrospectively. Data from patients who had undergone the open versus minimally invasive surgical approach were compared regarding operating time, intraoperative as well as postoperative maximum CO2 partial pressure (pCO2max) values, postoperative ventilation time, complications, and recurrences. Selection criteria for either a thoracoscopic or laparoscopic procedure were based on the clinical condition of the patient, in particular on the respiratory function and ventilation parameters, but also on circulatory function (Table 1).
Newborns and infants undergoing thoracoscopic repair were placed on a heating mattress in a prone position, the healthy side down, with an elevating pad beneath. Initially a 5-mm canula for the videoscope was placed one intercostal space below the tip of the scapula, followed by two 3-mm working ports placed under direct vision in the 7th or 8th intercostal space in the dorsal axillary line and ventrally, respectively, in order to facilitate a triangular position of the trocars directing towards the diaphragmatic defect. Insufflation of CO2 was initiated with 1–2 L/min, creating an intrathoracic pressure increasing from 2 to a maximum of 6 mm Hg in order to facilitate easy reducing of the enterothorax. Insufflation pressure was then decreased following repositioning of the bowel and spleen into the abdomen. If a true hernia sac was found, the sac was excised in order to provide proper healing. Manual approximation of both the diaphragmal rims was then anticipated in order to assess the feasibility of the closure of the hernia. The defect was then closed, using 2/0 or 3/0 nonabsorbable interrupted sutures (Mersilene, Ethicon, Norderstedt, Germany) intracorporeally knotted. If a posterior rim of the diaphragm could not be readily recognized or was absent, sutures were placed encircling the lowest rib. A chest drain was put under direct vision through the dorsal axillary line trocar site. Children who were operated on laparoscopically were placed supine on a heating mattress, using a 5-mm canula for the videoscope at the umbilicus and two 3-mm working ports in the right and left upper abdomen, respectively. Insufflation of CO2 was initiated with 1–2 L/min, creating an intraabdominal pressure as low as acceptable (8–10 mm Hg) for good vision, in order not to compromise the reducing of the viscera down to the abdomen against intraabdominal pressure. Insufflation pressure then was again decreased. Again the defect was closed by using 2/0 or 3/0 nonabsorbable interrupted sutures. All thoracoscopic and laparoscopic procedures were carried out by only two different surgeons, both of whom had at that time major experience with both laparoscopic as well as thoracoscopic procedures. Those included thoracoscopic lobectomies, laparoscopic dismembered pyeloplasties, and other reconstructive procedures.
Statistical evaluation
Data are reported with median and range if not otherwise indicated. To compare pCO2max values and the duration of postoperative ventilation in the two groups, the two-sample t test was performed on the log-transformed data. The level of statistical significance was set at P<.05. Statistical analysis was conducted with JMP® version 7.0.2 software (SAS Institute, Cary, NC).
Results
Patients had a left-sided CDH in 24 cases and a right-sided CDH in 9 cases. Median age at time of operation was 4 days (range, 0–1017 days). Median weight at time of operation was 3800 g (range, 2000–13,200 g). Laparotomy was performed in 12 children. Seventeen patients underwent thoracoscopic repair; in 7 cases a conversion to open surgery (laparotomy) was undertaken, with 5 of them requiring a GORE-TEX® patch (Gore Medical). Of those children undergoing thoracoscopic surgery, 11 were newborns. Four children had a laparoscopic approach for repair of their CDH. None of the children had pulmonary hypertension, and all children were on conventional ventilation at the time of operation. Patient data are given in Table 2.
CDH, congenital diaphragmatic hernia.
Median operating time was 90 min (range, 32–135 min) in the open group and significantly longer (P=.004) in the minimally invasive group with 120 min (range, 72–315 min). The pCO2max value during the operation was 43 mm Hg (range, 32–50 mm Hg) in patients undergoing open surgery versus 43 mm Hg (range, 31–78 mm Hg) for those undergoing a minimally invasive procedure; the difference was not significant (Fig. 2). However, pCO2max values in the postoperative course were significantly different (P=.013) with 58 mm Hg (range, 40–78 mm Hg) in the open and 42 mm Hg (range, 32–72 mm Hg) in the minimally invasive group (Fig. 3). There was a significant difference (P=.024) regarding postoperative duration of ventilation between the two groups: Patients with the open approach were on ventilation for 141 h (range, 2–504 h), whereas those who underwent minimally invasive surgery could get weaned after 20 h (range, 0–288 h) postoperatively (Fig. 4). None of the neonatal patients had any signs of intracranial bleeding in the postoperative course. Specific patient data are given in Table 3.
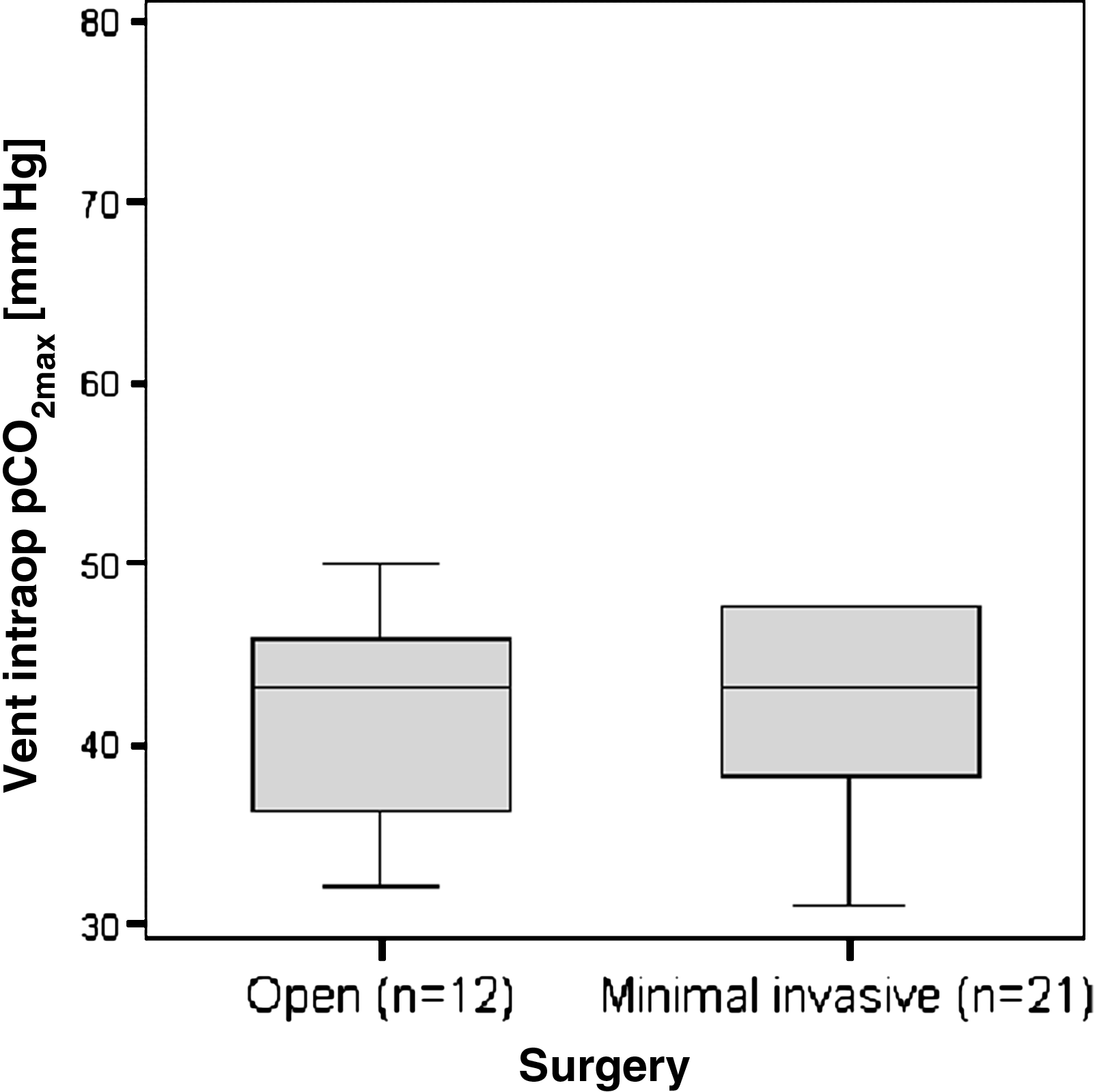
Intraoperative maximum CO2 partial pressure (pCO2max) values in patients undergoing open versus minimally invasive surgery.
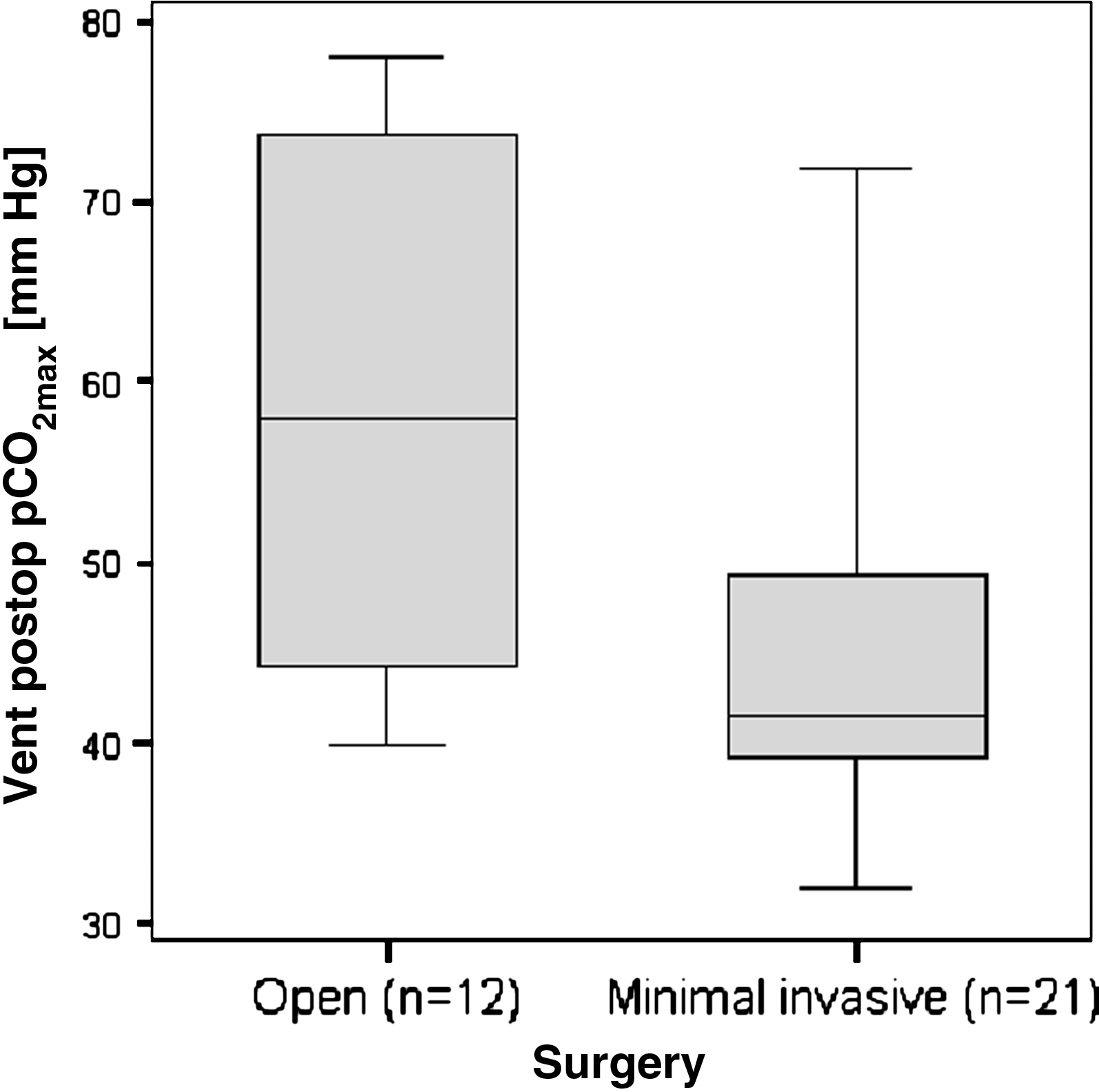
Postoperative pCO2max values in patients undergoing open versus minimally invasive surgery.
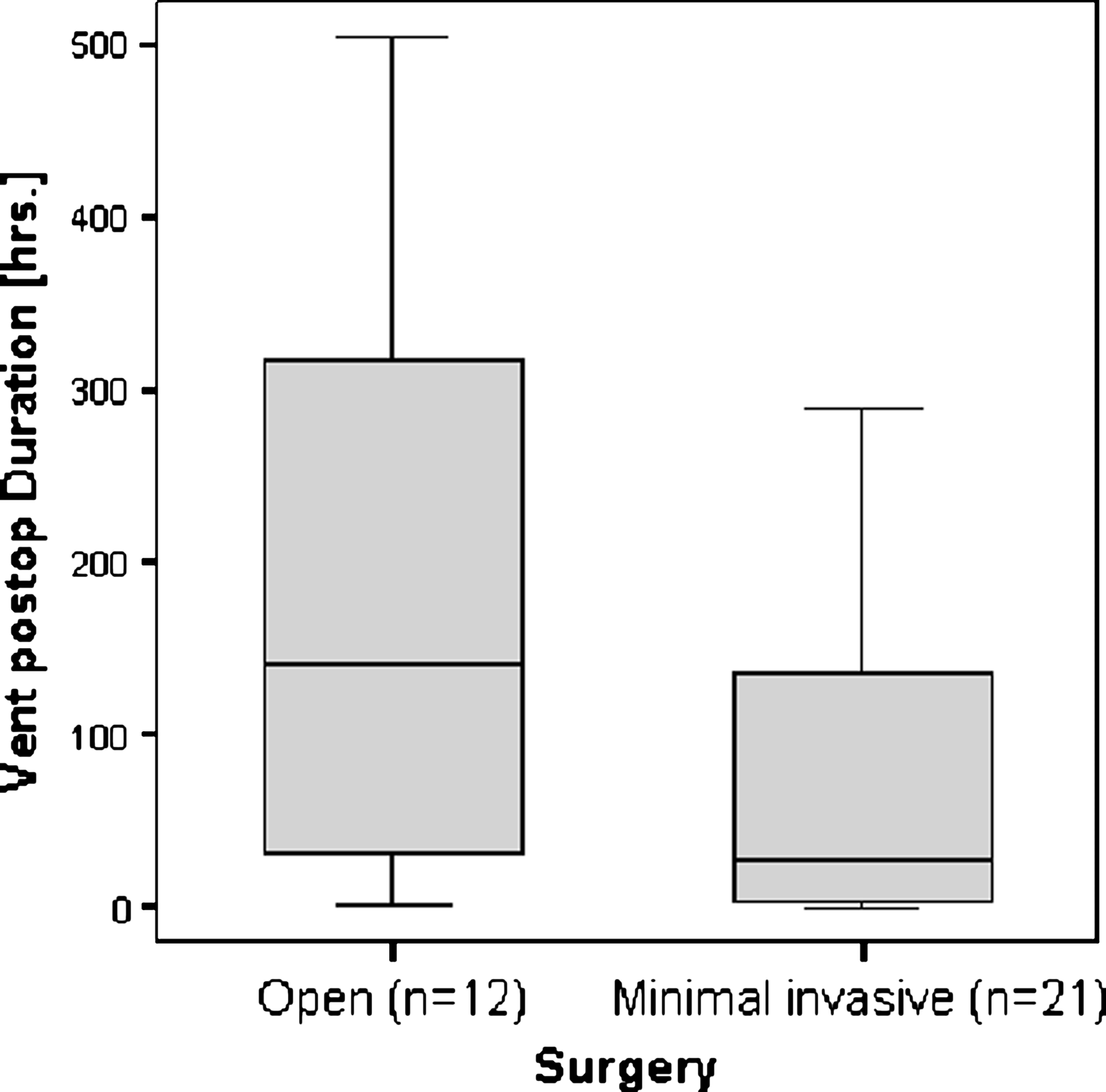
Postoperative ventilation time in patients undergoing open versus minimally invasive surgery.
By t test on log-transformed data.
NS, not significant; pCO2max, maximum CO2 partial pressure.
There was one complication in a child undergoing laparoscopic CDH repair (4.5%), suffering from jejunal perforation. Also, in the group undergoing minimally invasive surgery, five recurrences (23.8%) of the diaphragmatic hernia were noticed. Of these patients, three children underwent an open redo procedure, and two children could be operated on thoracoscopically and laparoscopically, respectively. No complications and no recurrences were noted in the open surgery group (Table 4).
Discussion
The use of minimally invasive techniques such as the thoracoscopic and laparoscopic approaches are proposed increasingly also for children with CDH.1–9 Although different studies published in the literature have described a superior outcome in patients undergoing a minimally invasive approach for the repair of their CDH (i.e., thoracoscopically),2,4 the immediate perioperative outcome has not been investigated so far.
This report reviews the authors' experience with different surgical approaches for CDH. Although median operating time was significantly longer for the group operated on by the minimally invasive approach, like in recent reports 1 there were no disadvantages in terms of hypercarbia or postoperative ventilation time. Median values of pCO2max during operation were not significantly different in the two groups; however, median values of pCO2max postoperatively were significantly lower in the minimally invasive surgery group. In addition, postoperative ventilation time was significantly shorter when children underwent minimally invasive surgery. This supports preliminary data from the literature that minimally invasive access for CDH repair results in good respiratory function and promotes quick recovery. Like in other published studies,1,2,5 predetermined selection criteria were not available to identify patients who could tolerate a minimally invasive, in particular a thoracoscopic, repair of their CDH. Therefore children were selected based on their clinical condition. From the surgical point of view selection criteria for either the thoracoscopic or laparoscopic approach were considered to depend on the anatomical site of the hernia. Therefore we preferred to operate on thoracoscopically in all cases of a left-sided Bochdalek hernia and for all kind of right-sided hernia. However, for left-sided ventral hernias (Morgagni) we found the laparoscopic approach more appropriate because of the accessibility, which proved to be much better and easier from the abdominal cavity. It was noted that, with insufflation, reducing of the viscera was easier to establish in the thoracoscopic procedures, whereas in patients undergoing laparoscopic repair preventing the bowel from herniating back into the thorax sometimes hindered the operation. However, one must consider that selection criteria (i.e., stable cardiorespiratory function) of patients for thoracoscopy or laparoscopy may be a bias towards less complicated postoperative courses. Selection of patients always was made by both surgeons and neonatologists; thus different aspects and opinions on how to treat the patient surgically in the best way had to be considered. One aim of this study was therefore to provide evidence that a minimally invasive approach does not compromise the patient, even when surgery is performed during the neonatal period. We could demonstrate that decreased postoperative ventilation time was associated with faster recovery and earlier discharge from the neonatal intensive care unit, whereas intraoperative values of pCO2max did not significantly differ. This also supports our opinion that intraoperative hypercarbia and acidosis in children undergoing thoracoscopic repair are not significantly worse than in open surgery. Reasons for intraoperative hypercarbia and acidosis are well identified, including a lateral positioning of the patient on the side with the “healthy” lung, the artificial pneumothorax on the operated side, along with the insufflated CO2, being absorbed by the pleura, thus even increasing the pCO2. However, those effects proved to be transient and tolerated by the patients, even in neonates like in other reports.1,2 However, all children operated on by the minimally invasive approach were on almost “normal” respiratory parameters when undergoing surgery, with one of the selection criteria being a peak inspiratory pressure below 25 mm Hg, which is according to recent opinions of other authors.2,3,5 Conversion of two patients to a laparotomy early in our series was due to failed respiratory adaptation under insufflation of CO2. With an increasing learning curve also for the anesthesiologist involved, this could be avoided in the subsequent patients. Another five children had been converted to either laparotomy or thoracotomy despite good respiratory parameters when the defect of the diaphragm was considered too large for endoscopic repair. However, recent studies3,4 have shown that patch repair of CDH can be performed also thoracoscopically and was later carried out successfully also at our institution. As previously published 7 and supported by other authors, 2 the presence of both a right-sided CDH or herniation of liver, spleen, or stomach into the chest may be a concern but not an exclusion for thoracoscopic repair.
Compared with previous reports, in our group minimally invasive CDH repair was associated with a relevant number of recurrences (5/21, 23.8%), whereas in children undergoing open surgery recurrences did not appear. Guner et al. 4 were first to report on experience with successful use of patches in using a minimally invasive technique; they noted a 20% recurrence rate. Other reports on thoracoscopic CDH repair have showed recurrence rates ranging from 2% to 14%,5,8,9 whereas recurrence rates in the literature for open CDH repair are reported to be on the order of 25%–44%.10,11 However, in a recent publication reporting the largest series of thoracoscopic CDH repair so far, the recurrence rate was 21%, 1 comparable to our own data. However, this series included also a 16% recurrence rate after patch repair, which compromises the comparison because in our own series patch repair was not performed thoracoscopically. Thus, the rather high rate of recurrences in our children undergoing minimally invasive CDH repair is still within the range known from previous reports. However, reasons for recurrence have yet to be analyzed critically. Therefore, long-term outcomes along with larger numbers of patients are anticipated for a more objective assessment. In our preliminary experience, we felt that anticipating a primary closure, thus avoiding the use of a patch, might be reflected in a rather high recurrence rate, when some of the closures of the diaphragmatic hernias could be only achieved with the acceptance of a certain tension of the sutures. With an increasing learning curve techniques for suturing as well for the use of a patch will further develop. Therefore we recommend the liberal use of a patch for closure of the defect as previously published in the literature,3,4 which was also performed successfully at our institution later, showing good results and no recurrences so far, but was not included in the present study.
Conclusions
In conclusion, despite skeptical considerations, minimally invasive surgery seems to offer advantages for selected patients with CDH. However, the authors are aware of the limitations of this retrospective study as well as that the selection criteria may be a bias towards less complicated postoperative courses when minimally invasive surgery is performed. To date, thoracoscopic repair of CDH seems to be superior to open surgery. However, decision-making on how to approach patients and especially neonates surgically should remain interdisciplinary and should include the surgeon, the anesthesiologist, and the neonatologists or pediatrician as well as the parents. Long-term results regarding functional results and recurrence rates are still pending.
Footnotes
Disclosure Statement
No competing financial interests exist.