
Abstract
Abstract
Background:
THUNDERBEAT™ (TB) (Olympus, Japan) simultaneously delivers ultrasonically generated frictional heat energy and electrically generated bipolar energy. The aim of this study was to evaluate the versatility, bursting pressure, thermal spread, and dissection time of the TB compared with commercially available devices: Harmonic® ACE (HA) (Ethicon Endo-Surgery, USA), LigaSure™ V (LIG) (Covidien, USA), and EnSeal® (Ethicon).
Methods:
An acute study was done with 10 female Yorkshire pigs (weighing 30–35 kg). Samples 2 cm long of small (2–3 mm)-, medium (4–5 mm)-, and large (6–7 mm)-diameter vessels were created. One end of the sample was sent for histological evaluation, and the other was used for burst pressure testing in a blinded fashion. Versatility was defined as the performance of the surgical instrument based on the following five variables, using a score from 1 to 5 (1=worst, 5=best), adjusted by coefficient of variable importance with weighted distribution: hemostasis, 0.275; histologic sealing, 0.275; cutting, 0.2; dissection, 0.15; and tissue manipulation, 0.1. There were 80 trials per vessel group and 60 trials per instrument group, giving a total of 240 samples.
Results:
Versatility score was higher (P<.01) and dissection time was shorter (P<.01) using TB compared with the other three devices. Bursting pressure was similar among TB and the other three instruments. Thermal spread at surgery was similar between TB and HA (P=.4167), TB and EnSeal (P=.6817), and TB and LIG (P=.8254). Difference in thermal spread was noted between EnSeal and HA (P=.0087) and HA and LIG (P=.0167).
Conclusion:
TB has a higher versatility compared with the other instruments tested with faster dissection speed, similar bursting pressure, and acceptable thermal spread. This new energy device is an appealing, safe alternative for cutting, coagulation, and tissue dissection during surgery and should decrease time and increase versatility during surgical procedures.
Introduction
Three energy-based methods currently used during surgical procedures for vessel ligation and dissection include monopolar electrosurgery, bipolar electrosurgery, and ultrasonically activated surgery. Monopolar electrosurgery results in greater thermal tissue damage and intraperitoneal temperature variations compared with ultrasonically activated surgery and bipolar electrosurgery, respectively. Bipolar electrosurgical technology has been considered as possibly a safer method for dissection and vessel ligation in laparoscopic colon and rectal surgery in particular because electrical energy is used differently, preventing undesirable injuries.1,2 Some studies evaluating vascular control during laparoscopic surgery between electrosurgical devices have reported that electrothermal bipolar vessel sealing has better results and effectiveness, less blood loss, and a slight advantage in operating time.3,4 Ultrasonically activated surgery devices are multifunctional and are equipped for coagulation, cutting, dissection, and grasping. A study comparing ultrasonic and bipolar devices in a porcine bowel mesentery model reported that ultrasonically activated surgery provides a reduced resection time with no difference in thermal bowel wall damage. 5 Among the current ultrasonic devices, laparoscopic dissection time in a porcine bowel mesentery model was shorter with AutoSonix™ (Covidien, USA) and Sonosurg™ (Olympus, Japan) technology compared with UltraCision® (USA) technology. 6 Technical advances in electrosurgery and other energy sources are increasing over time, with devices becoming more powerful and efficient.
A new laparoscopic device, THUNDERBEAT™ (TB) (Olympus), has been developed that delivers simultaneously ultrasonically generated frictional heat energy and electrically generated bipolar energy. This tool is also multifunctional, and the surgeon will be able to coagulate (even large blood vessels), cut, and dissect during surgery and potentially reduce the need for instrument exchange.
Thus the aim of this study was to evaluate the versatility, bursting pressure, thermal spread, and dissection time of the new TB device in comparison with commercially available ultrasonic and bipolar energy devices: Harmonic® ACE (HA) (Ethicon Endo-Surgery, USA), LigaSure™ V (LIG) (Covidien), and EnSeal® (Ethicon).
Materials and Methods
The project was an acute (nonsurvival) study with 10 female Yorkshire pigs (weighing 30–35 kg) conducted in accordance with Institutional Animal Care and Use Committee requirements regarding research with large animals in a single institution.
Hypotheses, primary variables, and definitions of primary variables
We tested the following four hypotheses: (1) TB will have a higher versatility score compared with the other instruments (see definition below); (2) TB will have a similar heat safety profile (thermal spread) compared with the other instruments; (3) TB will demonstrate faster dissection time compared with the other instruments; and (4) TB will have similar bursting pressure compared with the other instruments.
Primary variables were versatility score, thermal spread, time to dissection, and bursting pressure. Other variables evaluated were charring, sticking level, and number of ligations attempted.
Versatility
Versatility was defined as performance of the surgical instrument based on the following five variables, using a score from 1 to 5 (1=worst, 5=best) (Table 1), adjusted by coefficient of variable importance with weighted distribution: hemostasis, 0.275; histologic sealing, 0.275; cutting, 0.2; dissection, 0.15; and tissue manipulation, 0.1. An average score above 3.5 was considered as high versatility, and a score of 3.5 and below as low versatility.
Thermal spread
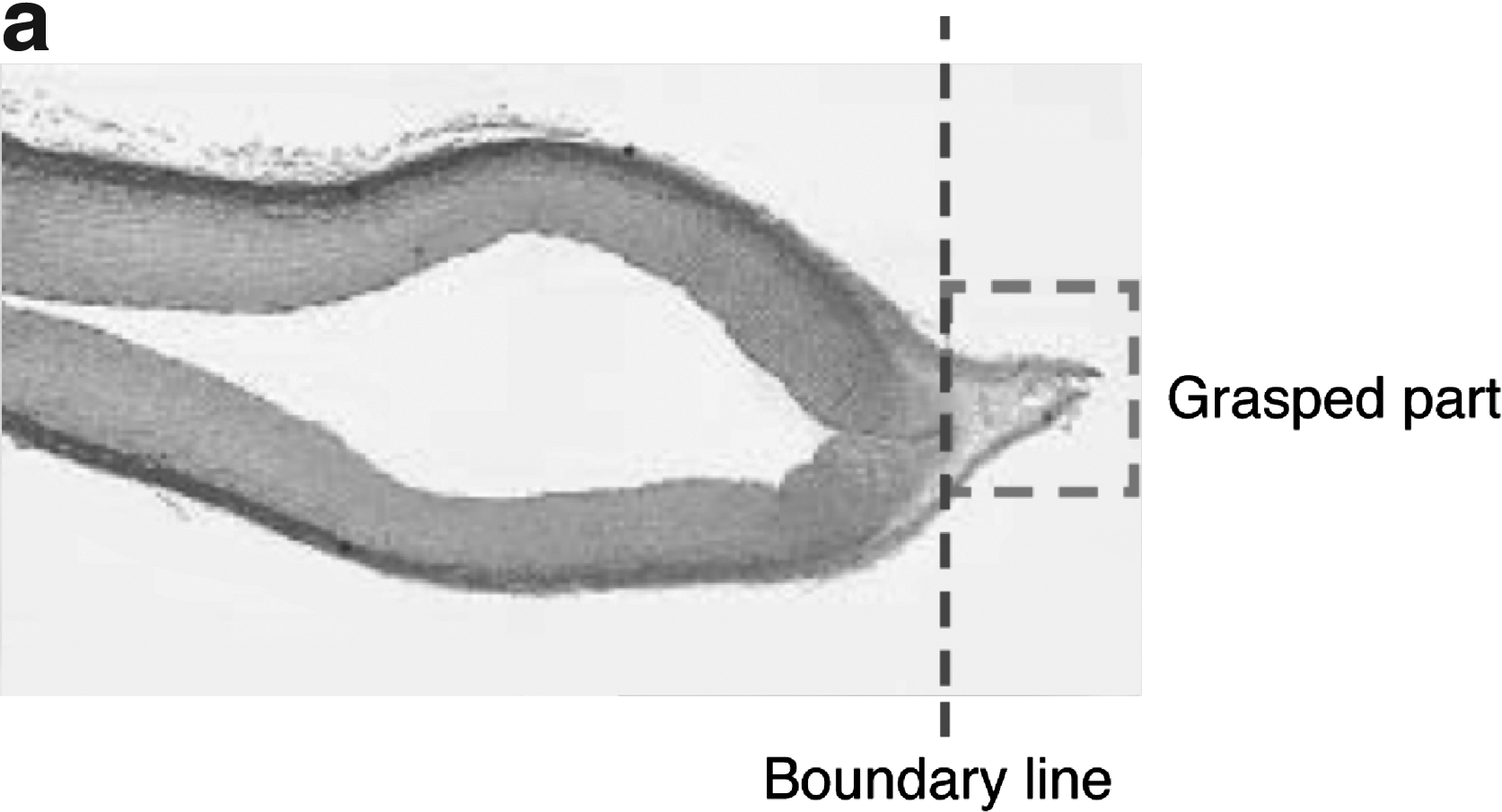
Thermal spread was defined as the width (in mm) of the collateral denatured tissues of the grasped vessel on both sides of the instrument jaw. Thermal spread was measured by the surgeon at the time of surgery by measuring the width of the blanched tissue on both sides of the instrument jaw using digital calipers (Fig. 1a).
Histological evaluation of the sealing and of thermal changes in the internal and external parts of the vessel was done by a pathologist. The pathologist was blinded to the type of surgical instrument by the use of coded labels. The samples were stained using hematoxylin–eosin, and a sealing score was assigned based on completeness of sealing and degree of the thermal effect at the sealed site measured in millimeters from the edge of the coagulated sample.
Dissection speed
Dissection speed was the time (in seconds) needed to dissect a 15-cm mesenteric segment by one surgeon. A 10% difference in time was considered clinically significant.
Bursting pressure
Bursting pressure (the pressure needed to cause a leak at the sealed site of a sealed vessel segment) was measured (in mm Hg) using a 30 psi (1,550 mm Hg) gauge. Bursting pressure was measured by a separate team in a blinded manner using a Terumo (USA) manometer (model PG-208-103GP-3-S), Copal Electronics (Japan) syringe pump (model KDS-200), KD Scientific (USA) syringe (model SS-10LZ), and a Terumo injection needle (26 gauge×½ inches).
Charring
Charring was measured using a score from 0 to 3: 0=no charring, 1=mild to minimal charring with tissues darkened from the heat application but not burnt; 2=moderate charring with clear identification of darkened tissues and some charring from burnt tissues; and 3=excess charring with charring from burnt tissues observed entirely where the tissues/vessel was grasped for coagulation.
Sticking level
Sticking level was graded with a score from 1 to 5 (1=worst, 5=best) and defined as follows: 1=tissue sticking such that tissue is damaged or torn during removal process; 2=tissue sticking requiring countertension and extensive force to remove tissue; 3=tissue sticking requiring countertension to gently grasp and remove tissue; 4=minor sticking requiring activation of instrument to release tissue; and 5=no sticking, tissue falls off the instrument when opened.
Equipment
Commercially available devices used were as follows: HA model ACE36E (5 mm×36 cm); LIG model V 1500 (5 mm×37 cm); and EnSeal model NSEAL-535H (5 mm×35 cm).
The investigational device used was the TB prototype (5-mm×35-cm) surgical tissue management system from Olympus Medical Systems Corp. The instrument has a tapered jaw design with a wide opening aperture (Fig. 2).
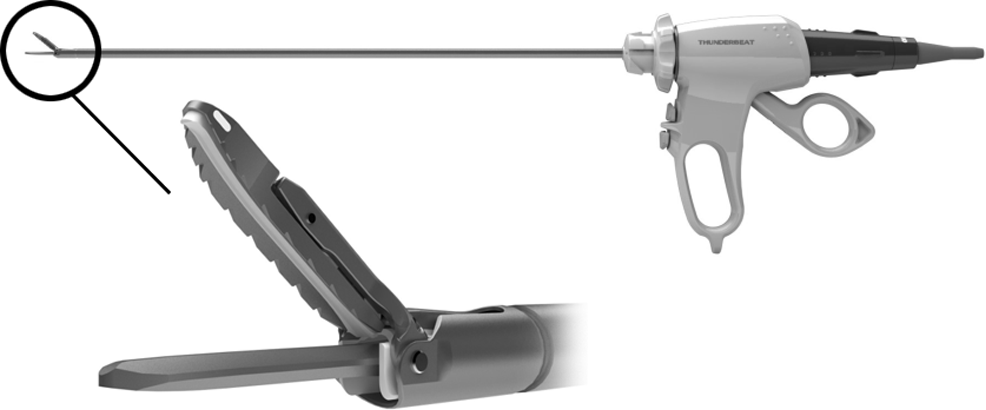
THUNDERBEAT. © 2010 Olympus Medical Systems Corp. All rights reserved.
The coagulation and cut levels of all generators were set up at a similar and constant level throughout the entire study (Table 2).
Surgical procedure
All operations were performed with the animal under general endotracheal anesthesia and under identical conditions, using the following agents: tiletamine–zolazepam (Telazol®; Wyeth Pharmaceuticals, USA), 4.4 mg/kg; glycopyrrolate, 0.07 mg/kg; buprenorphine (Buprenex®; Reckitt Benckiser, USA), 0.01 mg/kg; and the inhalant isoflurane. Bupivacaine was used to infiltrate the incision. Operations proceeded in a fashion similar to that used for human surgery. The animal was placed on the operating table in a supine position. The abdomen was shaved and draped. After making a midline abdominal incision (10–12 cm) we isolated the small and large bowel mesentery. Vessels were singly isolated and ligated; whether or not vessel ligation and dissection were effective was recorded for each trial by recording the number of the times the instrument was used to achieve ligation of the vessel. The following steps were followed during surgery: (1) isolate target vessels; (2) measure width of vessels; (3) ligate vessels and make samples for pathology and bust pressure measurement; (4) measure width of the visual thermal spread; and (5) measure burst pressure on the ligated samples.
Samples of small (diameter 2–3 mm), medium (4–5 mm), and large (6–7 mm) vessels were created in 2-cm segments during surgery, alternating the four instruments under investigation. One end of the sample was sent for histological evaluation, and the other was used for burst pressure testing in a blinded fashion. After completion of the vessel samples, a 15-cm mesenteric segment was dissected with each instrument, with the time to completion measured with a stopwatch. Surgical sites were inspected for bleeding, thermal injuries, and whether any iatrogenic injuries were suffered. This examination was performed by the surgeon visually.
Following completion of surgery each animal was euthanized while still under general anesthesia using 120 mg/kg sodium pentobarbital, i.v.
Arterial vessels used
For the purpose of this study, the arterial vessels have been categorized in three groups: Group 1, small-size vessels (2 and 3 mm); Group 2, medium-size vessels (4 and 5 mm); and Group 3, large-size vessels (6–7 mm). The following blood vessels were used during the study: gastroepiploic artery, gastrosplenic artery, mesenteric artery, splenic artery, and renal and iliac arteries.
Statistical analysis
In order to have an adequate number of trials, we performed 20 trials for each instrument with small-, medium-, and large-size vessels totaling 80 trials per vessel group and 60 trials per instrument group (total number of samples=240). Coefficient of variable importance with weighted distribution (hemostasis, 0.275; sealing, 0.275; cutting, 0.2; dissection, 0.15; and tissue manipulation, 0.1) was used to calculate the versatility score. Analysis of variance and Tukey's test for multiple comparisons were performed using JMP version 9.0 software (Cornell University, Ithaca, NY).
Results
All surgeries were performed with the animal under general anesthesia and according to the experimental plan. Detailed results are listed in Table 3. Animals were maintained at a constant blood pressure (80–120 mm Hg) throughout the experiment.
Data are mean±standard deviation values.
By one-way analysis of variance. A value of P<.05 was considered significant.
Evaluation at surgery.
EnS, EnSeal; HA, Harmonic ACE; LIG, LigaSure; TB, THUNDERBEAT.
Versatility
Sealing and histology
Histological evaluation of the samples did not show any difference in sealing ability between TB and the other three instruments (Table 3). However, EnSeal was found to be superior to HA in sealing (P=.0131) using Tukey's test for multiple comparisons. Histological examples of the coagulation are presented in Figures 3 and 4. All histologic samples had complete thermal effect, but not all of them had complete histologic seal. Overall, nine of 206 (4.4%) of all the samples had incomplete histologic seal, of which eight of these nine were from the large vessel group (eight of 79 samples, 10% of large vessels).
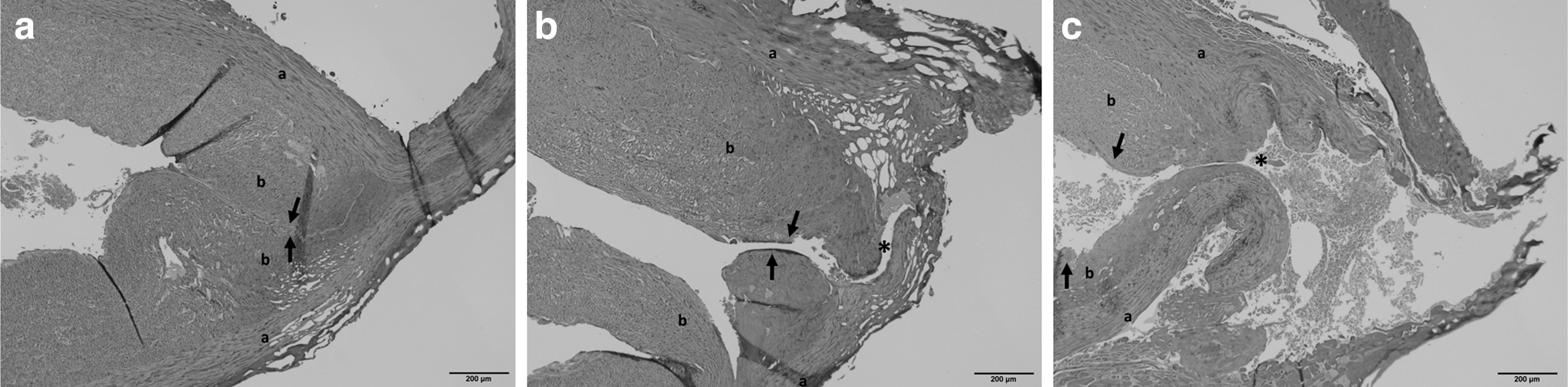
Examples of histologic sealing and thermal effect (hematoxylin–eosin stain) as defined in Table 1.
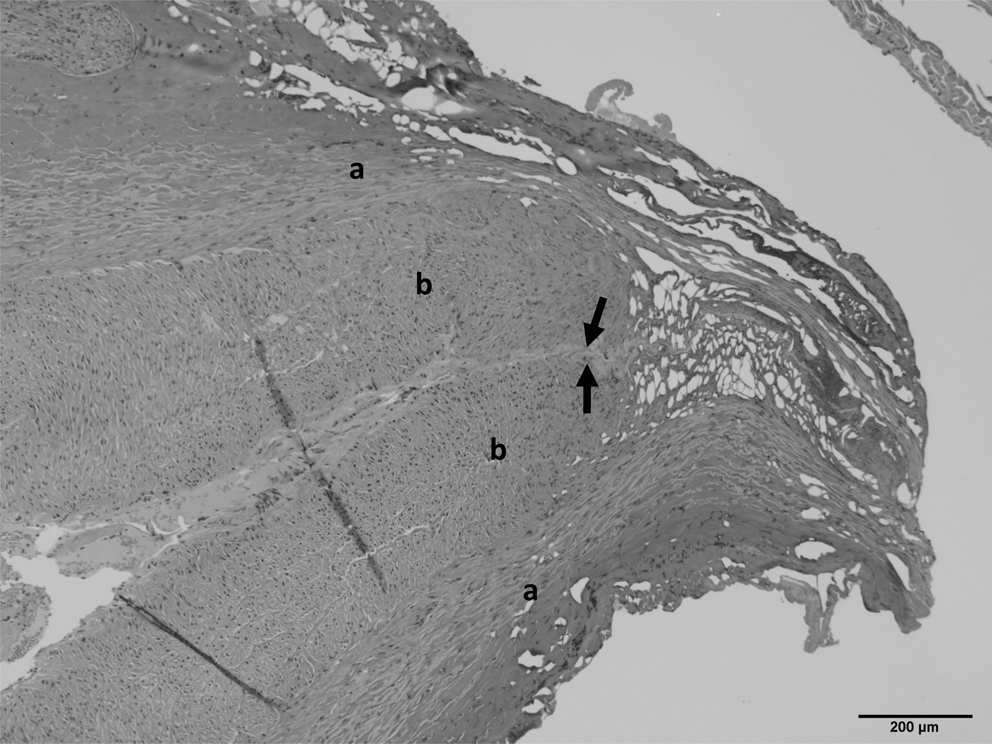
Complete histologic seal, complete thermal effect with the THUNDERBEAT. The arrows point at the sealed part. a, adventitia; b, intima.
Hemostasis during surgery
No overall difference (all blood vessel sizes) was noted in terms of hemostasis (P=.230) among the four surgical devices. The large-size vessels in general had significantly higher rates of bleeding (P<.0001), with a total of 15 of 80 (18.7%) requiring secondary action to achieve adequate hemostasis. No difference, however, was detected among the instruments on hemostasis within the large vessel group (P=.1496) (Table 3). The hemostasis failures were as follows: 5% (four of 80) failed to achieve hemostasis after two attempts with the instrument (score of 1), 6.2% (five of 80) of the large vessel samples developed heavy bleeding requiring immediate further intervention (score of 2), and 7.5% (six of 80) of the large vessels required placement of a vascular suture (score of 3).
Cutting, dissection, and tissue manipulation scoring during surgery
Cutting, dissection, and tissue manipulation scores were significantly different among the instruments with P<.0001 in the three parameters. The TB cutting score (mean±SD) of 4.9±0.1 was significantly higher compared with LIG (4.5±0.7) (P<.0001). The dissection score of TB (mean±SD) (5.0±0) was higher compared with the EnSeal (4.5±0.6) and LIG (4.7±0.5) devices (P<.0001 and P<.0028, respectively). No difference in the dissection score between TB score (5.0±0) and HA score (4.8±0.3) (P=0.3945) was noted. The tissue manipulation score was higher for TB over EnSeal and LIG (P<.0001 and P=.0024, respectively). No difference was noted regarding tissue manipulation score between TB and HA (P=.6284).
After calculation of the versatility score using the coefficient of variable importance with weighted distribution as described above, all instruments demonstrated high versatility (>3.5). However, TB had significantly higher versatility than LIG, EnSeal, and HA (P=.0042, P=.0450, and P=.0120, respectively).
Bursting pressure
Bursting pressure was similar among TB and the other three instruments (P=.2090). It is interesting that the bursting pressure was different among the vessel groups. The medium-size vessels (4–5 mm) had the highest bursting pressure (mean/SD, 900.5±537.3 mm Hg; P=.0249) compared with the small- (712.9±587.8 mm Hg) and large-size (683.9±483.7 mm Hg) vessels (Table 3 and Fig. 5).
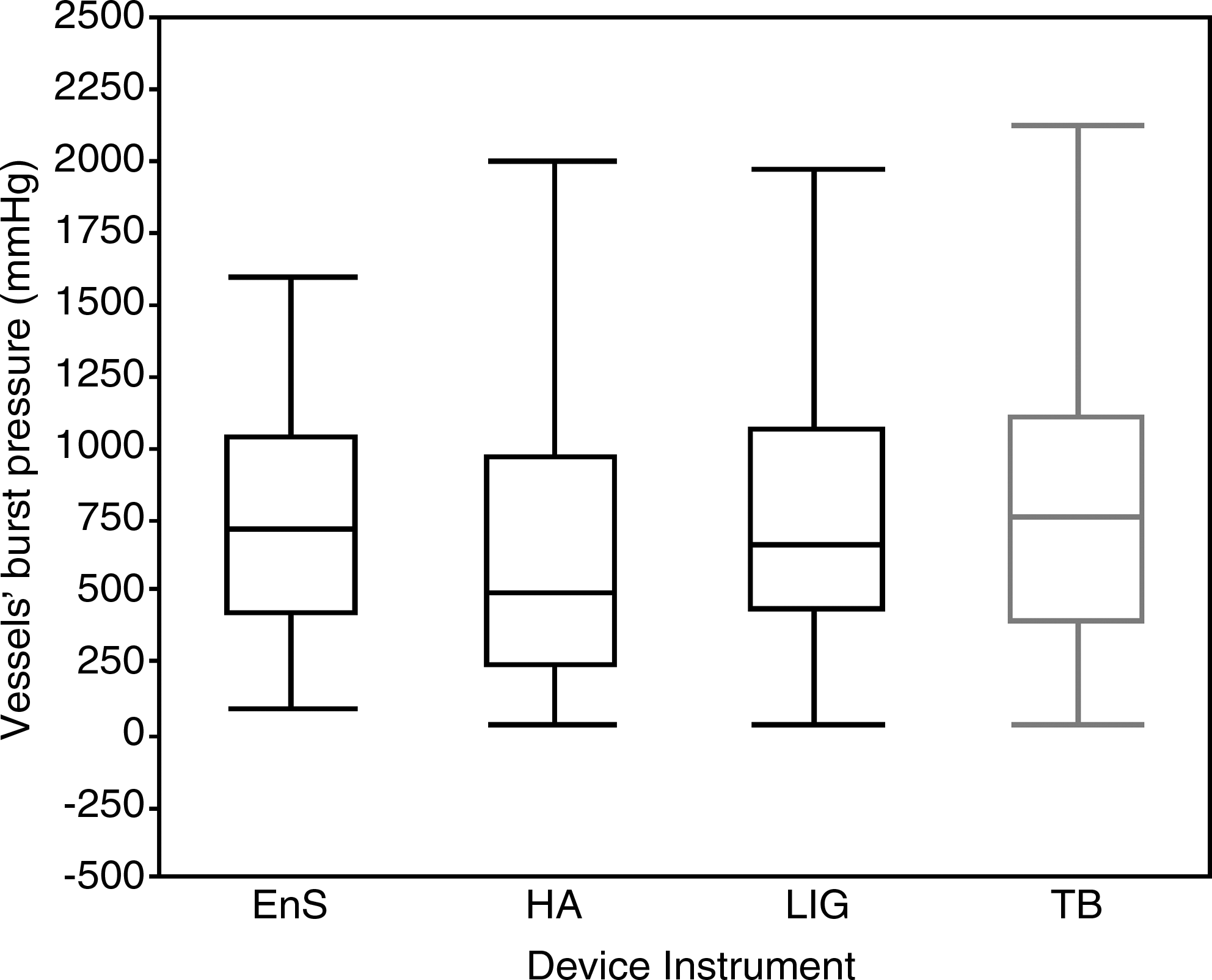
Comparison of bursting pressure among the instruments: EnSeal (EnS), Harmonic ACE (HA), LigaSure (LIG), and THUNDERBEAT (TB).
Dissection time
Dissection time was lower with TB (mean±SD, 31.1±3.2 seconds) compared with the other three devices (P<.0001) (Table 3).
Thermal spread
Thermal spread measured at the time of surgery was different among the instruments (P=.0369); however, it was similar between TB and HA, TB and EnSeal, and TB and LIG (P=0.4167, P=.6817, and P=0.8154, respectively). A difference in thermal spread was also noted among vessel groups: The large-diameter vessels (6–7 mm) had significantly higher thermal spread compared with small- (2–3 mm) and medium-diameter (4–5 mm) vessels with corresponding P values of P=.0002 and P=.0237 (Table 4).
Data are mean±standard deviation values.
By one-way analysis of variance. A value of P<.05 was considered significant.
Histological evaluation of the samples revealed two distinguishing areas: (1) Area A (Fig. 1b, A) of complete transmural necrosis with thermal change at the extremity of the vessels, which was characterized by intense hypereosinophilia of the tissue with loss of cellular details, and variable formation of clear clefts; and (2) area B (Fig. 1b, B) with intimal thermal changes characterized by hyalinization and basophilic staining of the collagenous matrix with viability of the cell preserved. The extent of the thermal changes in area A was similar between TB and HA (P=.9469) and between LIG and EnSeal (P=.7731). When we compared the extent of the thermal changes in the adventitia (area B, Fig. 1b, B) among the different vessel size groups, there were no differences noted between the instruments in the medium-size (4–5 mm) vessel group (P=.1650). In the large-size vessel group there were no differences in the extent of the changes between TB and EnSeal (P=.1330) and TB and LIG (P=.1502). HA demonstrated shorter length of thermal changes compared with TB (P=.0032) (Table 5).
Data are mean±standard deviation values (n).
By one-way analysis of variance. A value of P<.05 was considered significant.
Sticking level
No difference was shown in comparing sticking level between TB and HA (P=.9354) and TB and EnSeal (P=.0795). However, TB had significantly less sticking compared with LIG (P<.0001).
Charring
TB had a lower charring level compared with EnSeal (P=.0320). There was no difference in the charring level between TB and HA (P=.8866) and TB and LIG (P=.1255). Ligation attempts were similar among all instruments.
Discussion
Laparoscopic surgery has stimulated the use of advanced technologies in the operating room and development of new surgical devices in abdominal surgery. In particular, devices with thin 5-mm-diameter shafts have proven useful in both laparoscopic and open surgery. Many of the new technologies have easily been adapted to these long thin instrument designs, which are of great usefulness even in open surgery, particularly in the upper abdomen and in the pelvis. Until now, however, use of a combined energy device using both ultrasonic and bipolar energy together has not been available clinically. The use of ultrasound frictional energy (fast tissue dissection, even on thin peritoneal tissue) combined with bipolar electrical energy (reliable sealing of even large blood vessels) is appealing, in that it may equip the surgeon with one instrument capable of cutting through nearly any tissue that may be encountered in the abdomen, and do so efficiently.
In order to test the clinical usefulness of this new combined energy device (TB) with the commercially available HA, LIG, and EnSeal devices, we designed an experiment that would test the “versatility score” based on five factors that were weighted according to arbitrary clinical values adding up to 1 (hemostasis, 0.275; sealing, 0.275; cutting, 0.2; dissection, 0.15; and tissue manipulation, 0.1). We believed that the most important factors in the versatility were the hemostasis and sealing capabilities, followed by cutting, and thus weighted the “values” accordingly. We additionally measured the parameters of bursting pressure and thermal spread, which have previously been used for comparisons between energy devices and other surgical sealing methods (clips and sutures).7–9 All of the sealing and hemostasis evaluations in this study were done in vivo, with live animals that were normotensive throughout the testing. Many of the other studies comparing different energy devices were done ex vivo or in preserved tissues, which may not be as representative of actual clinical situations as our model.7–9
Regarding hemostasis and vessel sealing, we did experience hemostasis failure of 5%, heavy bleeding of 6.2%, and sealing failure at histology in 4.5% of vessels (mostly large but one medium), without differences among instruments. Newcomb et al. 8 previously reported that large-size vessels have the longest seal time and the highest rate of failure to seal. In our study, we approached the ligation and sealing of large vessels (iliac and renal arteries) with extreme caution but attempted to ligate these vessels with a single seal in order to test each instrument using the same technique throughout the experiment. The bleeding came from the proximal end after cutting. In clinical situations where a large vessel may be ligated, we would consider repeated application of sealing before cutting in the middle of multiple seals. In addition, ligation of an iliac artery in the animal model may not be analogous to the clinical situation of ligating a major mesenteric vessel, in that these animal iliac vessels may be thicker and more difficult to ligate with electrical energy.
Concerning tissue manipulation scores, TB had the highest score (4.9) among the groups, but all of the devices had good scores, ranging from 3 to 5 with average in all above 4.4. The TB's jaw design likely played a role in this, in that rapid and clean dissection was the rule in using this device.
Because all of the comparison devices tested in our study have U.S. Food and Drug Administration approval, we expected them to seal blood vessels well. Bursting pressure has been considered an indicator for vessel sealing.8,10 The TB performed well in comparison, with supraphysiologic bursting pressures seen in all groups and all blood vessels. Even though the medium-size blood vessels had higher burst pressures, the high value (900.5±537.3 mm Hg) also indicates that there were no physiologic differences. A recent study by Sindram et al. 11 demonstrated that the collagen–elastin ratio and vessel type play a role in the level of the bursting pressure rather than the vessel diameter.
Thermal spread measured at surgery was lowest in the HA and TB devices, likely because of the rapid dissection with these instruments due to the ultrasonic technology. Less thermal spread is of some clinical significance in that adjacent structures must be protected. With the increase of the vessel size the thermal spread increased, and the large vessels demonstrated significantly higher thermal spread. However, in all vessel groups and within each instrument group the thermal spread measured at surgery time was below 2 mm. We cannot state that the differences seen in this study would be of clinical importance. Rather, the objective of improving energy or tissue sealing devices should be the achievement of less and less lateral thermal spread, so this end point is important.
The histological thermal changes in intima and adventitia were larger than the thermal spread measured at surgery. This is likely because the microscopic thermal effect on the tissue extends further than what is perceived by the naked eye. Even though many studies have reported histological thermal spread, there are no clear criteria described as to how exactly it should be measured. Most of the studies measure the thermal changes from the cut edge of the coagulated vessel.7,8,12 In order to measure the actual thermal spread and not overall histological thermal changes, the area where the vessel was grasped needs to be marked prior to the histological evaluation. Because we did not mark this area in each sample we reported the overall thermal effect changes. This is particularly important in order to avoid faulty interpretations about the histological thermal spread of different energy devices.
We also tested the dissection speed of all four instruments in an arbitrary model in a 15-cm-long segment of mesentery. This is a test that we developed in our laboratory prior to the performance of this experiment, and it appeared to be very reproducible during our preliminary studies. The low variability of times within tests of each instrument suggests that this may be a reliable measure of how quickly each instrument can cut and seal mesentery. We realize that this type of measure also depends on the surgeon performing the study, and all tests in this experiment were done by one surgeon.
TB and HA performed better in terms of charring and sticking compared with EnSeal and LIG. It is important for the surgeon to be acquainted with the properties of these devices in order to minimize injury and optimize safety during surgery. Studies comparing energy devices rarely measure these parameters and comment about their importance. Dubuc-Lissoir 13 reported in a human study that the LIG vessel sealing system performed with minimal sticking and charring, but it was not clear how the scoring was performed. In our study we found that the LIG V has a higher level of sticking and charring compared with the other instruments.
Limitations
This is a preclinical study in a porcine model, and thus it is not clear if the results will be replicated in a live human. In order to study the treatment effect on larger mesenteric vessels, iliac vessels and renal vessels were substituted in this porcine model. Furthermore, the funding for this comparative study was supplied solely by Olympus. In order to minimize bias, the study was completed in a single institution, and all surgeries were performed by one surgeon. Additionally, a separate team measured the bursting pressure in a blinded manner, and the pathologist was blinded to the instrument used.
The potential benefits of this lab are ultimately to future patients who are to undergo extensive soft tissue dissection within the abdomen and pelvis and in particular for colorectal operations such as colectomy. If one surgical device can adequately cut, coagulate, and manipulate tissues while limiting tissue damage caused by thermal spread, this could reduce the operative time as well as complication rates.
Conclusions
The TB has a higher versatility score compared with the other instruments with faster dissection speed, similar bursting pressure, and acceptable thermal spread. In this preclinical model this new energy device is an appealing, safe alternative for cutting, coagulation, and tissue dissection during surgery and should decrease time and increase versatility during surgical procedures. Its use in human surgery seems promising.
Footnotes
Acknowledgments
The authors wish to acknowledge and express sincere gratitude to Olympus for financial support of this project.
Disclosure Statement
Koiana Trencheva, Dr. Sebastien Monette, Dr. Raghava Pavoor, Dr. Parul Shukla, and Dr. Junjun Ma have no conflicts of interest or financial ties to disclose. Dr. Jeffrey W. Milsom has received course support from Olympus, Covidien, and Applied Medical and research support from Olympus. Dr. Toyooki Sonoda has received course support from Olympus, Covidien, and Applied Medical and research support from Adolor.