
Abstract
Abstract
Objective:
This study evaluated the impact of obesity on learning to perform laparoscopic surgery for colon cancer.
Subjects and Methods:
We compared the outcomes for 72 patients with colon cancer treated by a single surgeon between June 2005 and July 2008. The first 36 patients who underwent surgery were considered to be during the “early period,” and the other 36 patients who underwent surgery as the “late period,” and the patients with a body mass index (BMI) ≥25 kg/m2 were defined as being obese.
Results:
During the early period, the tumor stages of obese patients were less advanced than those of nonobese patients, whereas the length of the operation, surgical blood loss, and wound diameter of obese patients were worse than those of nonobese patients. Furthermore, the tumor stages in the obese patients during the late period were more advanced than those in obese patients during the early period, whereas the length of the operation and number of dissected lymph nodes in the obese patients during the late period were better than those in obese patients during the early period.
Conclusions:
We demonstrated that the differences of the surgical outcomes between obese and nonobese patients undergoing laparoscopic colon resection decreased as the surgeon's experience increased.
Introduction
In several previous studies, obese patients had longer surgeries, higher conversion rates to open surgery, and higher morbidity and mortality rates than nonobese patients.12–14 However, other studies reported that obesity did not have an adverse impact on either the technical procedures or the postoperative outcomes of laparoscopic colon resection.5,15–19 Furthermore, it has been reported that the body mass index (BMI) was considered to be one of the independent predictors of conversion to open surgery in laparoscopic colorectal surgery. 5 However, there have been no reports about the relationship between obesity and the learning curve for laparoscopic colon resection.
In this study, we tried to clarify the impact of BMI related-obesity on a single surgeon's learning laparoscopic surgery for colon cancer.
Subjects and Methods
Patients
Seventy-two patients with colon cancer, including 10 cecums, 20 ascending colons, 5 descending colons, 20 sigmoid colons, and 17 rectosigmoid colons, who underwent surgery by a single surgeon between June 2005 and July 2008 at Wakayama Medical University Hospital (Wakayama, Japan) were enrolled in this study. This surgeon had served as the assistant for 20 laparoscopic colectomies for 1 year and as the surgeon for open gastrointestinal surgeries during 16 years before this study.
First, we selected the period during which a single surgeon first performed consecutive surgeries as the primary surgeon, because this surgeon has performed the laparoscopic colectomies partially as the instructor for the junior class surgeon after this consecutive surgery period.
Next, we tried to divide this selected period to two equal periods and compare the data between early and late periods. When the time period was divided into two equal parts, 36 patients were distributed in each part by chance. We defined the period of the first 36 patients who underwent surgery as the “early period,” whereas we defined the later 36 patients who underwent surgery as being treated in the “late period.”
We considered it adequate to divide the patients into two groups of 36 patients, because it has been reported that the learning curve for laparoscopic colon resection stabilizes after 30–70 cases5–11 including 36 patients.
The obese patients were defined as those with a BMI of ≥25 kg/m2, and those patients with a BMI of <25 kg/m2 were nonobese according to the criteria of the Japan Society for the Study of Obesity. 20 We divided all patients into four groups as follows: nonobese patients who underwent surgery in the early period (early nonobese group); obese patients who underwent surgery in the early period (early obese group); nonobese patients who underwent surgery in the late period (late nonobese group); and obese patients who underwent surgery in the late period (late obese group).
The surgical procedures consisted of 10 ileocecal resections, 20 right hemicolectomies, 5 left hemicolectomies, 20 sigmoidectomies, and 17 high anterior resections. The patients were placed in the lithotomy position with head-down and right-side-down tilting for sigmoidectomy and high anterior resection, whereas they were placed in the supine position with opened legs for ileocecal resection, right hemicolectomy, and left hemicolectomy. Five-port trocars including a blunt port, two 5-mm ports, and two 12-mm ports were introduced for sigmoidectomy and high anterior resection, whereas five-port trocars including a blunt port, three 5-mm ports, and one 12-mm port were introduced for ileocecal resection, right hemicolectomy, and left hemicolectomy. With the patient under pneumoperitoneum with CO2 gas to a maximum of 10 mm Hg, laparoscopic exploration was performed. Transection and anastomosis of the bowel were performed extracorporeally through a small incision that was covered with an impermeable protector for ileocecal resection, right hemicolectomy, and left hemicolectomy. For sigmoidectomy and a high anterior resection without stapling anastomosis, the transection and anastomosis of the bowel were performed extracorporeally through a small incision, whereas for those with stapling anastomosis, the transection of the distal bowel was performed intracorporeally, and that of the proximal bowel was performed extracorporeally through a small incision.
The patient and tumor characteristics were compared for the following three clinical variables: clinicopathological features, intraoperative factors, and postoperative factors. The clinicopathological features consisted of age, gender, prior abdominal surgery, primary lesion, maximum tumor size, the extent of the tumor located in the cross-sectional circumference of the bowel, histopathological type, depth of invasion, lymph node metastasis, liver metastasis, lung metastasis, peritoneal invasion, lymphatic invasion, venous invasion, TNM stage, serum carcinoembryonic antigen (CEA), and serum carbohydrate antigen 19-9. The intraoperative factors consisted of the surgical procedure, stapling anastomosis, length of the operation, surgical blood loss, transfusion, wound diameter, length of the resected colon, number of dissected lymph nodes, number of metastatic lymph nodes, and intraoperative complications. The postoperative factors consisted of the start of oral water intake, start of oral food intake, postoperative complications, and the postoperative hospital stay.
A primary lesion was defined as follows: right-sided primary lesion, tumor proximal to the splenic flexure; and left-sided primary lesion, tumor distal to the splenic flexure. The depth of invasion was defined as follows: Tis, intraepithelial or invasion of the lamina propria; T1, tumor invades the submucosa; T2, tumor invades the muscularis propria; T3, tumor invades through the muscularis propria into the subserosa or into nonperitonealized pericolic or perirectal tissues; and T4, tumor directly invades other organs or structures and/or perforates the visceral peritoneum. The TNM clinical stage was described according to the International Union Against Cancer classification of malignant tumors. 21
No preoperative chemotherapy or radiotherapy was performed in this study.
Statistical analyses
The statistical analyses were performed with the Stat View-J version 5.0 software program using the Windows XP operating system. Significant differences in clinicopathological features, intraoperative factors, and postoperative factors were determined by Student's t test and either the chi-squared test or Fisher's exact test.
A value of P<.05 was considered to be statistically significant.
Results
Clinicopathological features
Table 1 shows the comparative analyses of the clinicopathological features among the four groups. The maximum tumor sizes of the early nonobese and late obese groups were significantly higher than those of the early obese group (P=.025 and P=.019, respectively). The extent of the tumor located in the cross-sectional circumference of the bowels of the early nonobese and late obese groups was significantly higher than that of the early obese group (P=.030 and P=.008, respectively). The histopathological type of the late obese group consisted of fewer tumors of the well-differentiated type than in the early obese group (P=.033). The depth of invasion of the early nonobese and late obese groups consisted of more T3 and 4 cancers than the early obese group (P=.011 and P<.001, respectively). The incidence of lymph node metastasis in the early nonobese and late obese groups was significantly higher than that in the early obese group (P=.005 and P=.006, respectively). Venous invasion was significantly more common in the late obese group than in the early obese group (P<.001). The early nonobese and the late obese groups consisted of more patients with TNM stage 3 and 4 disease than the early obese group (P=.005 and P=.002, respectively). The serum CEA level of the late obese group was significantly higher than that of the early obese group (P=.005).
Data are mean±SD values or numbers of patients (%).
(+), obese; (−), nonobese; CA, carbohydrate antigen; CEA, carcinoembryonic antigen; E, early period, the period when the first 36 patients underwent surgery; L, late period, the period when the other 36 patients underwent surgery; left-sided primary lesion, tumor distal to the splenic flexure; right-sided primary lesion, tumor proximal to the splenic flexure; Tis, intraepithelial or invasion of the lamina propria; T1, tumor invades the submucosa; T2, tumor invades the muscularis propria; T3, tumor invades through the muscularis propria into the subserosa or into nonperitonealized pericolic or perirectal tissues; T4, tumor directly invades other organs or structures and/or perforates the visceral peritoneum.
Intraoperative factors
Table 2 shows the comparative analyses of the intraoperative factors among the four groups. The lengths of the operation for the early nonobese and late obese groups were significantly shorter than that of the early obese group (P=.026 and P=.008, respectively). The surgical blood loss of the early obese group was significantly greater than that of the early nonobese group (P=.038). The wound diameter of the early obese group was significantly larger than that of the early nonobese group (P=.010). The length of the resected colon of the late nonobese group was significantly longer than that of the early nonobese group (P=.002). The numbers of dissected lymph nodes in the early nonobese and the late obese groups were significantly higher than that of the early obese group (P=.005 and P=.004, respectively); moreover, that of the late nonobese group was significantly higher than that of the early nonobese group (P=.048). The numbers of metastatic lymph nodes in the early nonobese and late obese groups were significantly greater than that of the early obese group (P=.018 and P=.027, respectively). There were no significant differences in the incidence of intraoperative complications among the four groups. The intraoperative complications included one stapler misfire for the early nonobese group, two missed lesions and one stapler misfire for the late nonobese group, and one stapler misfire for the late obese group. No conversions to open surgery were performed during this study.
Data are mean±SD values or numbers of patients (%).
Figure 1 shows the changes in the length of the operation. In the early period, the length of the operation for the obese group was significantly longer than that of the nonobese group (P=.026). There was no significant difference in the length of the operation in the nonobese groups between the early and late periods, whereas the length of the operation for the obese groups in the late period was significantly faster than that in the early period (P=.008).
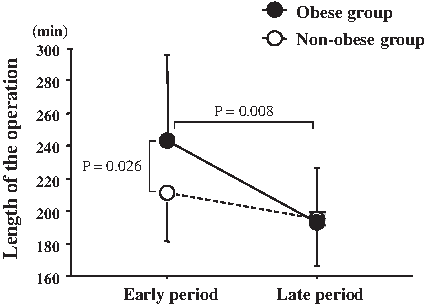
Changes in the length of the operation between the early and late periods. In the early period, the length of the operation in the obese group was significantly longer than that in the nonobese group (P=.026). There was no difference in the length of the operation in the nonobese groups between the early and late periods, whereas the length of the operation in the obese group was significantly shorter than that in the early period (P=.008).
Postoperative factors
The start of oral water intake and oral food intake in the late nonobese group was significantly earlier than that of the early nonobese group, and those values for the late obese group were significantly earlier than those for the early obese group (P<.001 versus P=.014 and P<.001 versus P=.009, respectively). Furthermore, the postoperative hospital stay of the late nonobese group was significantly shorter than that of the early nonobese group, and that of the late obese group was significantly shorter than that of the early obese group (P<.001 and P=.010, respectively). There were no significant differences in the incidence of postoperative complications among the four groups.
The observed postoperative complications were one case of peritonitis, one case of pneumonia, and one anastomotic stenosis for the early nonobese group, one case of peritonitis, one case of pneumonia, and one anastomotic stenosis for the early obese group, and one case of allergic dermatitis and one case of mild liver dysfunction in the late nonobese group (Table 3).
Data are mean±SD postoperative days or numbers of patients (%).
(+), obese; (−), nonobese; E, early period, the period when the first 36 patients underwent surgery; L, late period, the period when the other 36 patients underwent surgery.
Discussion
In Asians, a BMI of ≥25 kg/m2 is the cutoff for obesity. 12 Therefore, in this study, obese patients were defined as those with a BMI of ≥25 kg/m2, whereas those with a BMI of <25 kg/m2 were considered nonobese according to the criteria of the Japan Society for the Study of Obesity, the International Obesity Task Force, and previous studies.20,22 In some previous reports, the impact of obesity on laparoscopic surgery for the colon and rectum has been studied according to the definition of obesity as a BMI of ≥30 kg/m2, as classified by the World Health Organization.20,22 However, several studies have shown that the prevalence of individuals with a BMI of ≥30 kg/m2 is very low in the general Japanese population.20,21 Furthermore, the International Obesity Task Force has proposed a BMI cutoff of 25 kg/m2 for obesity in Asians according to the risk factors and morbidities.12,20
In the previous studies, the traditional outcomes that have been analyzed after laparoscopic colorectal resections were the length of the operation, intraoperative complications, conversion to open surgery, postoperative complications, and postoperative length of hospital stay. 6 In our study, no differences were observed in the incidence of the intra- and postoperative complications among the four groups, and there were no conversions to open surgery. The risk factors associated with conversion to open surgery have been described in the previous literature and include high BMI,5,13,23 excessive tumor bulk, adhesions, diverticular phlegmon, Crohn's masses,5,24 and the surgeon's experience.5,6 Moreover, various studies have also demonstrated that the number of intraoperative laparoscopic-related complications, conversion rate, and morbidity and mortality rates decreased with increasing experience of the surgeon.5,25,26 In this study, during the early period, in spite of the smaller tumor size, greater superficial invasion, fewer lymph node metastases, and less advanced TNM stage in the obese patients, the outcomes of the obese patients were worse than those of nonobese patients, including the length of the operation, blood loss during the operation, wound diameter, number of dissected lymph nodes, and number of metastatic lymph nodes. However, there were no differences in the variables between obese and nonobese patients during the late period. In Japan, lymph node dissection for the preoperative clinical TNM stage 0 and I cases that consisted of Tis and T1 depth invasion is usually performed within the epicolic, paracolic, and intermediate lymph nodes and is not performed for the lymph nodes around the origin of the feeding artery. The early obese patients consisted of stages 0, I, and II only in this study; therefore the numbers of lymph node dissected in the early obese patients might be smaller than that of the other groups. On the other hand, some technical problems for the obese patients might lead to the smaller number of lymph nodes in the early period. Obese patients with advanced stage in the early period had better undergo laparoscopic colectomy by the surgeon according to the instruction of the senior class surgeon. Furthermore, in spite of the larger tumor sizes, less well-differentiated type tumors, deeper invasion, more lymph node metastases, more venous invasion, more advanced TNM stage, and higher serum CEA of the obese patients in the late period, the outcomes of the obese patients in the late period were better than those of obese patients during the early period, such as the length of the operation, number of dissected lymph nodes, number of metastatic lymph nodes, start of oral water intake, start of oral food intake, and postoperative hospital stay. These results suggest that the impact of obesity on the outcome of laparoscopic colon resection may be decreased as the surgeon's experience increases.
Here we have clarified the impact of BMI-related obesity on the learning of laparoscopic surgery for colon cancer by a single surgeon.
Footnotes
Disclosure Statement
No competing financial interests exist.