
Abstract
Abstract
Background:
Multiple stapler firings during distal rectal division were associated with unduly long stapler line and anastomotic leakage after laparoscopic rectal resection. A simple and relatively easy technique to perform a safe transection of rectum is presented.
Materials and Methods:
The extracorporeal ligation of the rectum just proximal to the cut end of the rectum before applying the linear stapling stapler facilitates the procedure and requires only a few firings of the stapler during the laparoscopic rectal resections.
Results:
Ten patients with a median age of 72 years underwent rectal transection with this technique. The procedure was performed with a single 60-mm cartridge in 3 patients, and two firings of the Endo GIA™ (Covidien LLC, Mansfield, MA) with a 45-mm cartridge were necessary for cross-stapling at the level of the pelvic floor in the remaining patients. There were no intraoperative complications. Postoperative complications were seen in 2 patients.
Conclusions:
This simple technique theoretically seems safer than the conventional approach and should be considered as an additional option for rectal transection.
Introduction
Materials and Methods
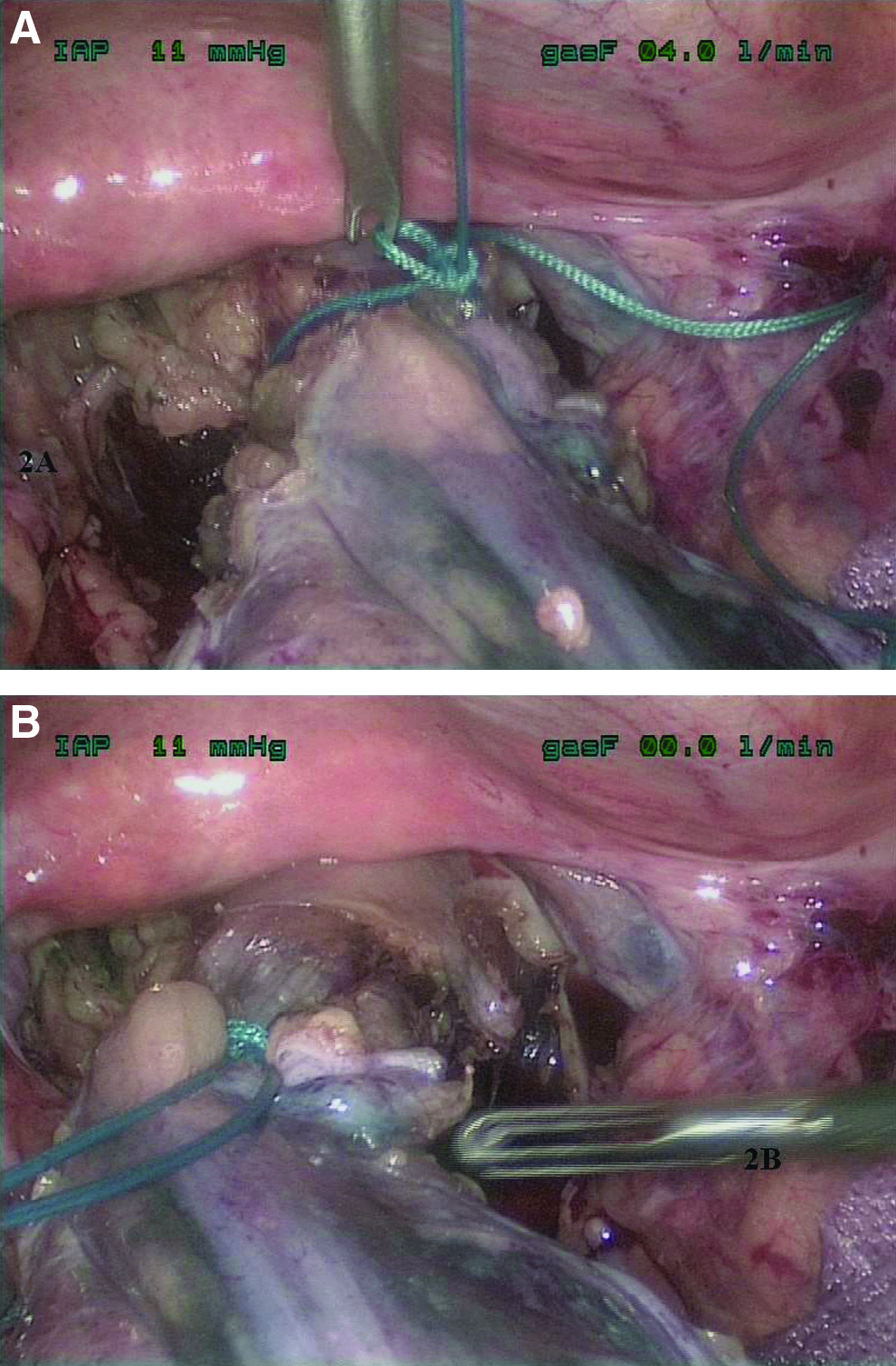
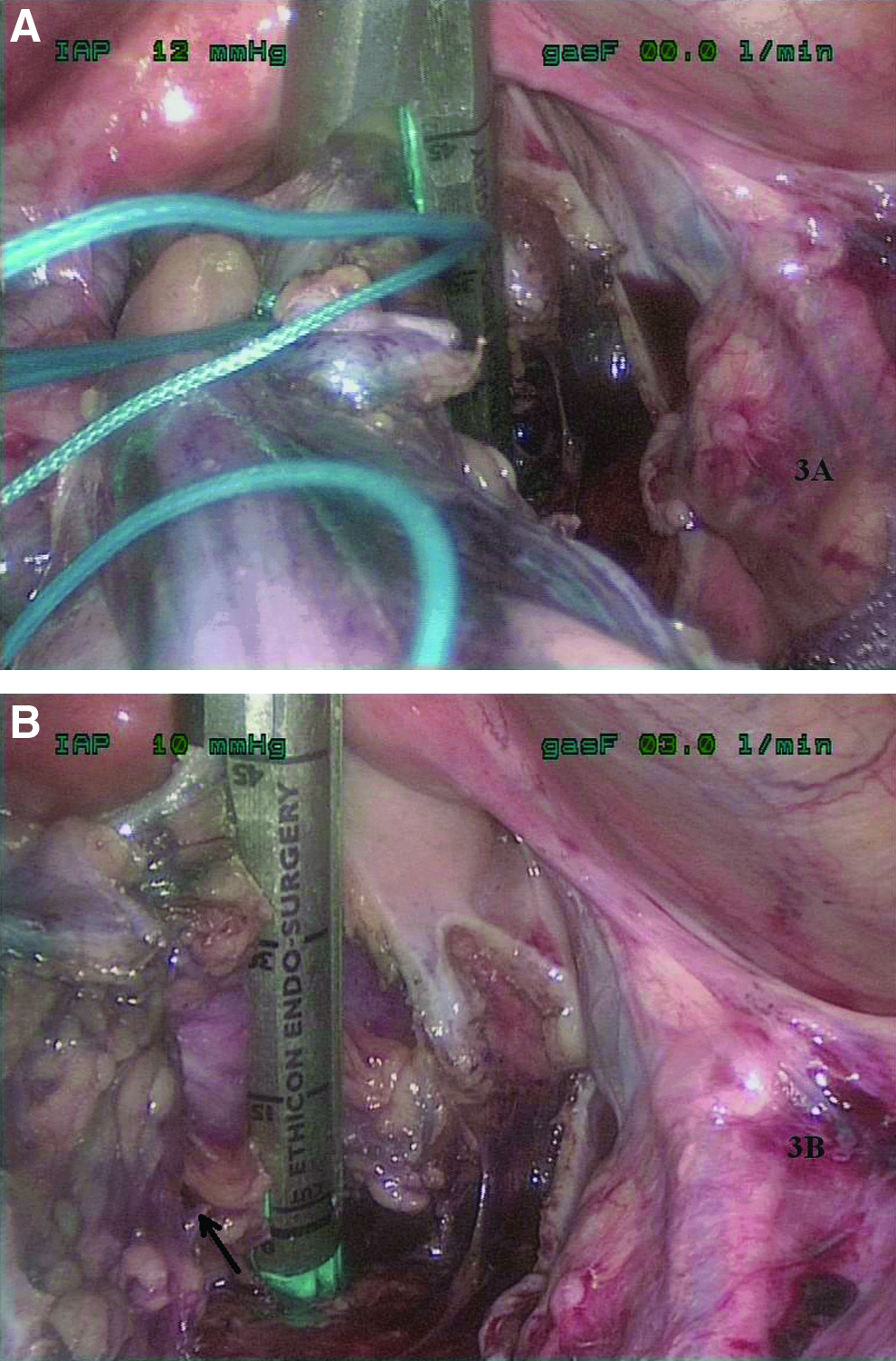
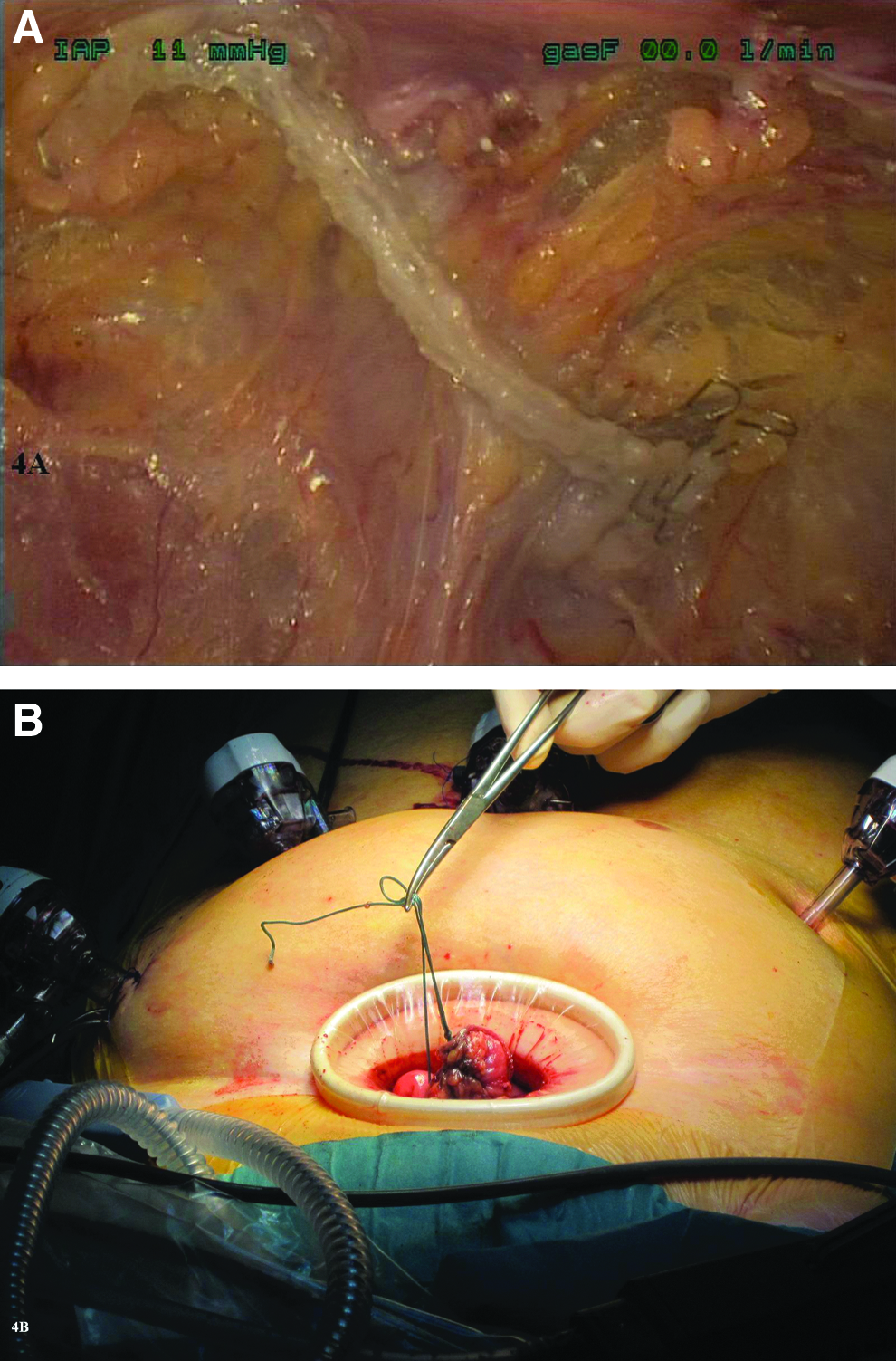
LTME was performed using five ports. The abdomen was insufflated with CO2 to a pressure of 12 mm Hg. After clipping of the inferior mesenteric vessels and pelvic dissection of the mesorectum, the rectum was dissected down to the muscle tube of the rectum below the inferior extent of the mesorectum. Then a long Ethibond Excel™ 5 suture (Ethicon, LLC, San Lorenzo, Puerto Rico) was passed to the peritoneal cavity through a 10-mm suprapubic port (Fig. 1A), making a loop all the way around the dissected rectal muscular tube just proximal for the expected cross-stapling line, and then brought back outside through the suprapubic trocar (Fig. 1B). The suture was tied around the rectal muscular tube using an extracorporeal knot technique (Fig. 2A). Then the free ends of the suture were taken out through an upper right-sided 5-mm port to facilitate the proper traction of the rectum in a correct direction for the application of the Endo GIA (Fig. 2B), and the rectum was lifted up by extracorporeal retraction on the free ends of the suture (Fig. 3A). A roticulating Endo GIA was introduced through the suprapubic port and applied to the muscular tube of the rectum just below the level of the suture ligation, and cross-stapling of the rectum was then performed using one or two cartridges (Fig. 3B), almost like in open surgery (Fig. 4A). Extraction of the transected proximal rectum could now be achieved by retracting the free ends of the suture through the suprapubic incision (Fig. 4B). The rectal resection was completed extracorporeally, and the anvil of the circular stapler was attached to the proximal colon, which was then returned to the abdominal cavity. The anastomosis was performed by use of a double-stapling technique.

Results
Our experience to date includes 10 patients with a median age of 72 years. Most of the patients were male (70%) (Table 1). In 3 patients with high rectum cancers, the procedure was performed with a single 60-mm cartridge. Two firings of the Endo-GIA with a 45-mm cartridge were necessary for cross-stapling at the level of the pelvic floor in the remaining patients. There were no intraoperative complications. Postoperative complications were seen in 2 patients, both with an American Society of Anesthesiologists score 3 classification; one was an anastomotic leakage treated with transanal drainage, and the other was seen in a patient who developed a pelvic fluid collection requiring ultrasound-guided drainage.
ASA, American Society of Anesthesiologists; AV, anal verge; HO, Hartmann's operation; LAR, low anterior resection; LAR-l, low anterior resection with protective ileostomy.
Discussion
Cross-stapling of the rectum following LTME using linear stapling devices can be challenging, especially in men with a narrow pelvis and a bulky mesentery. The space available in the pelvis varies between the sexes and also depends on the relation between the pelvic and tumor dimensions. It is not often possible to transect the rectum with a single cartridge at the level of the pelvic floor because of anatomical confinement of the pelvis. Multiple firings of the roticulating linear stapler result in an insecure zig-zag staple line, which interferes with an adequate circular stapling. 4 Yamamoto et al. 5 found that the most common intraoperative complication leading to conversion was a difficult rectal transection. Hand-assisted hybrid approaches, including vertical rectal division,6,7 have been used to overcome these difficulties, and recently some alternative techniques were reported, such as the use of an endo-Satinsky clamp, 8 the intestinal bulldog clamp, 9 and the instruments for stapled hemorrhoidopexy. 10 We have attempted to manage this problem by adopting the cotton tape tie technique described by Chung et al. 3 in 1997. Although the present report involves a limited number of patients, we only needed one cartridge in 3 patients and two cartridges in the 7 other cases. There were two minor complications, which were both controlled with drainage, in our series of 10 patients.
We found that it can be difficult to manipulate the distal rectum for applying an Endo GIA when the endo-Satinsky clamp is used. In addition, the number of cartridges required for cross-stapling of the rectum in this series was almost similar compared with the other reported series.7–9 The retraction and manipulation of the bowel were much easier with our technique. A correct placement of the rectal ligation may also serve as a marker to ensure that a clear distal margin is secured, even in the cases with small rectal tumors. Unfortunately, we have no experience with the use of instruments for stapled hemorrhoidectomy in laparoscopic rectal surgery. 10 However, this approach can only be used for low rectal tumors and needs more experience.
In conclusion, our patient series is too small to draw solid conclusions, but we believe that the use of an extracorporeal ligation of the rectum may reduce the number of stapler firings for rectal transection. Therefore, we hypothesize that this technique seems theoretically safer than the conventional approach and should be considered as an additional option for rectal transection during LTME. Furthermore, it may allow effective rectal lavage, when appropriate.
Footnotes
Acknowledgments
The author is indebted to Per Jess, MD, Dr Med Sci, and Ian N. Mitchell, RN, for his review of this manuscript.
Disclosure Statement
No competing financial interests exist.