
Abstract
Abstract
Background:
An infected urachal remnant is an uncommon benign condition that usually recurs and has the potential to become malignant. This study aimed to review our experience in laparoscopic excision of urachal remnants and report the efficacy and outcomes of the procedure in children.
Patients and Methods:
Between January 2010 and January 2012, five children with a median age of 35 months presented with urachal remnants at our institute. The data and treatment outcomes of all the patients were retrospectively reviewed. Laparoscopic surgery was performed using three ports, including the umbilical port. In all five children, the urachal remnant was excised from the umbilicus to the bladder dome by electrocauterization, and the stump on the bladder was ligated with endoloop sutures and some absorbable sutures.
Results:
All the five procedures were completed successfully. The median pneumoperitoneum time was 75 minutes. The boundary between the normal bladder wall and the urachal remnant was clearly identified using a laparoscope, allowing excision of the remnant and muscle layer of the bladder wall. No intraoperative or postoperative complications were reported at a median follow-up of 16 months. Complete resection of the urachal remnant was confirmed by pathological evaluation. No symptom recurrences were encountered. Laparoscopic resection had good cosmetic outcomes.
Conclusions:
Laparoscopic resection of urachal remnants in children allows for better anatomical visualization and may be considered as a safer, more effective, and more cosmetically beneficial alternative to open surgery.
Introduction
A
Patients and Methods
Between January 2010 and January 2012, one girl and four boys with a median age of 35 months underwent laparoscopic excision of urachal remnants (Table 1). Of the 5 patients, 3 had omphalitis symptoms, 1 had hematuria, and 1 did not have any symptoms. The 4 patients with symptoms were fully examined by abdominal ultrasonography (US). For the patient with no symptoms, a screening abdominal US and subsequently diagnostic magnetic resonance imaging (MRI) were performed to detect the congenital abnormalities due to Cornelia de Lange syndrome. The 3 patients with omphalitis symptoms were preoperatively treated with drainage of the infected umbilical wound and oral antibiotics.
F, female; M, male; MRI, magnetic resonance imaging; US, ultrasonography; VCUG, voiding cystourethrography.
Surgical technique
Under general anesthesia and in the supine position, each patient underwent bladder catheter insertion and insertion of three trocars into the peritoneal cavity. In the present study, the trocar site for the laparoscope was modified to improve operability. In the cases of apparent umbilical urachal remnants, the periumbilical urachal remnant was initially dissected through a semicircular infraumbilical incision, free from abdominal fascia, and then a 5-mm trocar was inserted through the same incision. In the cases with no pathological umbilical lesion, an initial port was inserted through a longitudinal umbilical incision. A 5-mm port was placed in the right midclavicular line above the level of the umbilicus, and another 5-mm port was placed at the right anterior axillary line blow the umbilical level. A 30° telescope was inserted from the upper lateral or umbilical port. The dissection was completed with electrocautery. After the bladder dome was delineated by distending it with normal saline, the urachal remnant was meticulously dissected from the muscle layer of the bladder. The root of the urachal remnant was amputated, and the mucosal part of the dissected bladder was ligated twice with a polydioxanone endoloop. The muscle layer of the bladder dome was closed using some absorbable sutures. Once the bladder reconstruction was completed, the bladder was filled with normal saline to identify points of leakage, if any. The specimen was exteriorized via the umbilicus in all the cases. A urethral catheter was left indwelling for 1–3 days postoperatively to keep the bladder decompressed.
Results
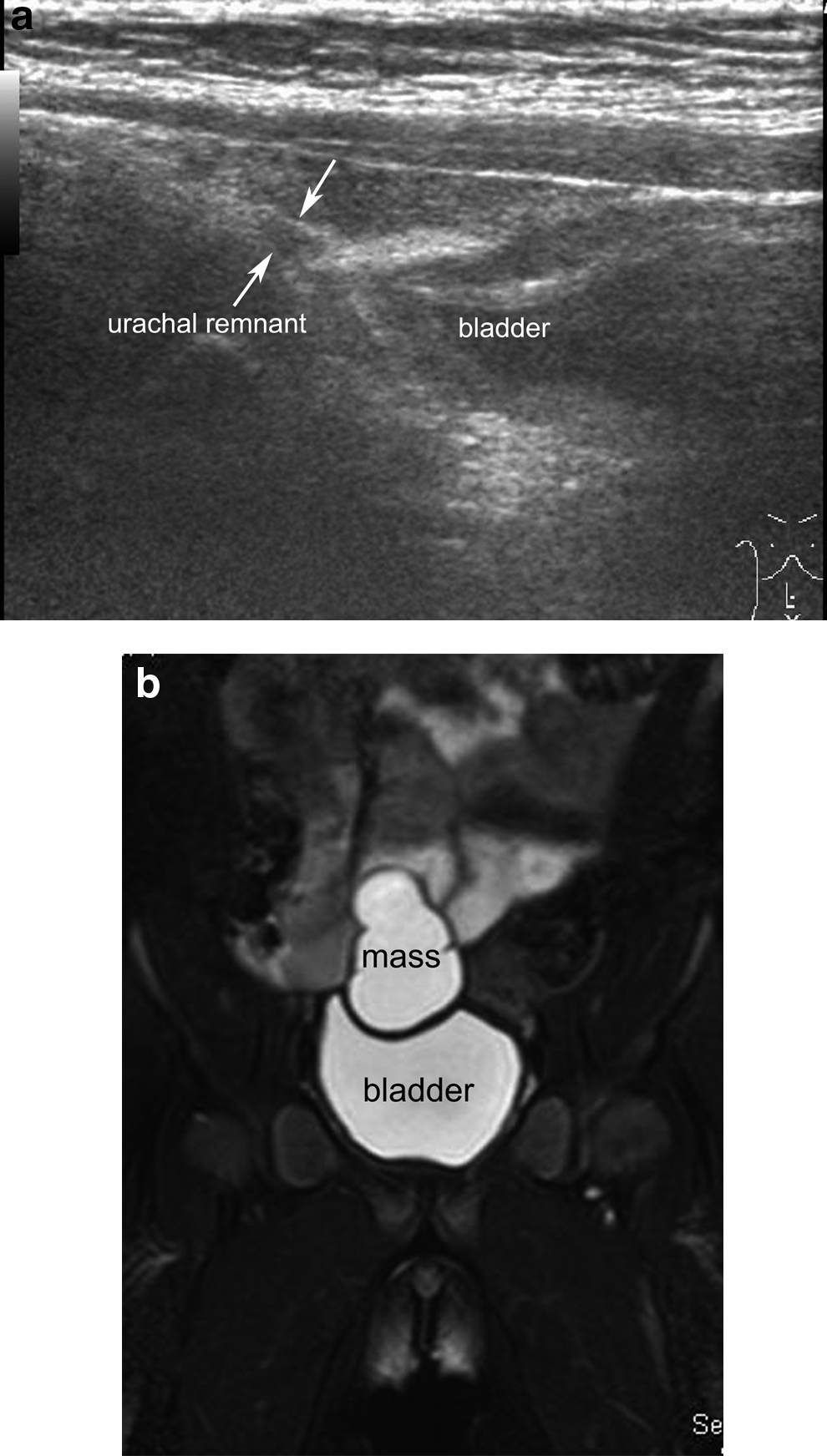
Preoperative US was useful for the diagnosis of the urachal remnants in 4 patients, of whom 3 had a hypoechogenic mass under the periumbilical region and on the bladder dome (Fig. 1a), which are connected with the urachal remnant. Patient 4, who had hematuria, had the hypoechogenic mass on the bladder dome only. Urachal remnants were precisely preoperatively diagnosed in these 4 patients. Case 5 was suspected as having right salpinx cysts on US and MRI (Fig. 1b). She was diagnosed as having large urachal cysts in the bladder dome in the process of the laparoscopic operation.
All five operations were successfully completed. The operative time ranged from 112 to 180 minutes (median, 125 minutes), and the pneumoperitoneum time ranged from 63 to 156 minutes (median, 75 minutes). Patient 5, who had large urachal cysts, required partial bladder resection (Fig. 2a and b) because the cysts were too large for identification of the boundaries between the cysts and the muscle layer. The bladder was reconstructed using single-layer suturing with an additional port. In the other 4 cases, the boundaries between the normal muscle layer of the bladder wall and the urachal remnants were clearly identified using a laparoscope, and complete excision of the remnants could be performed without opening the inner bladder cavity (Fig. 2c). No intraoperative or postoperative complications were reported during the follow-up period ranging from 11 to 35 months (median, 16 months). No patient had urinary leakage. Complete resection of the urachal remnant was confirmed by pathological evaluation. No dysplastic tissue was identified in the pathological specimens. All the patients are currently asymptomatic, without any local signs of recurrence. Laparoscopic resection had good cosmetic outcomes.
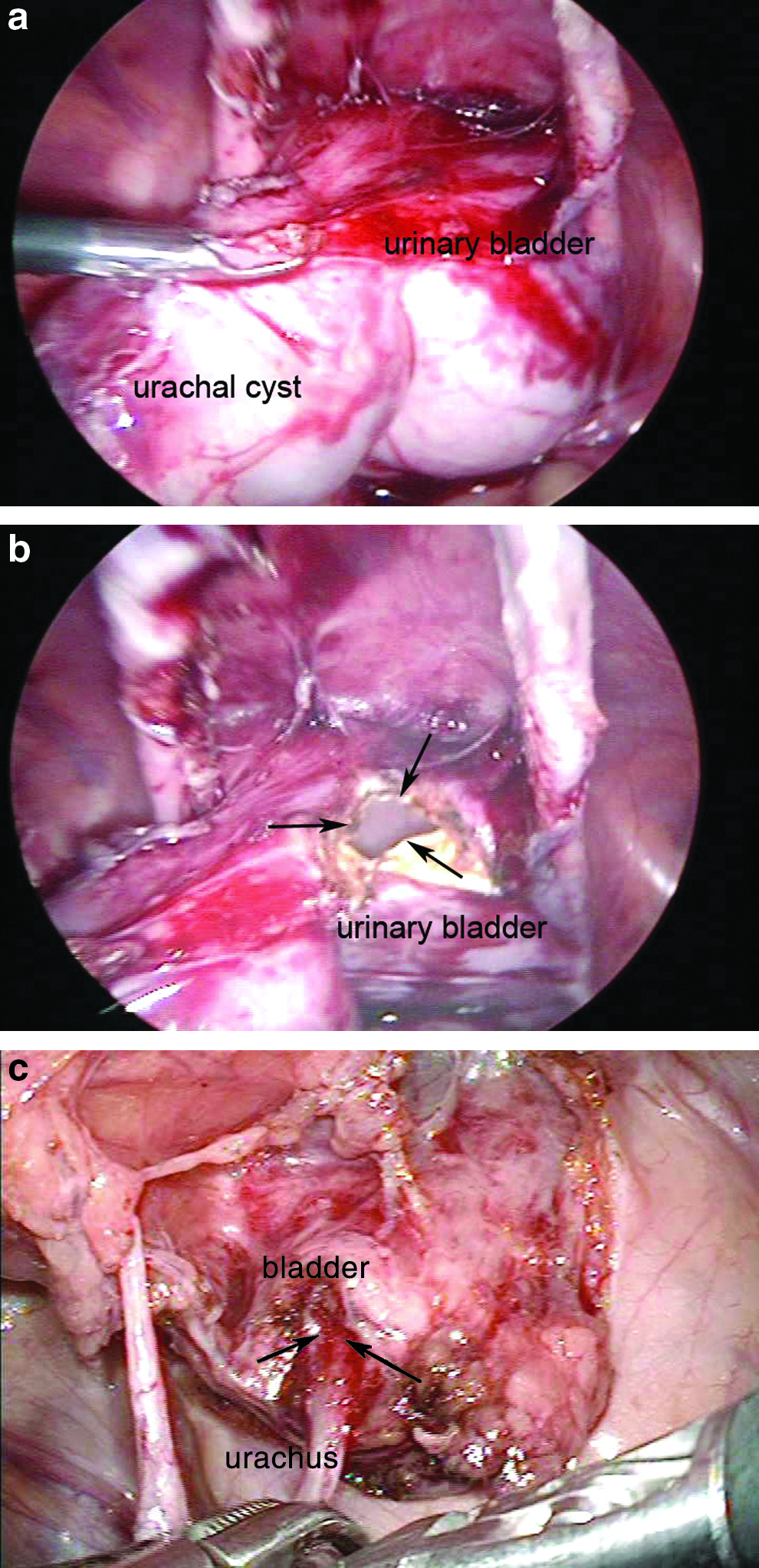
Laparoscopic images.
Discussion
The urachus is ordinarily obliterated and becomes the median umbilical ligament after birth. Failure of this regression results in urachal remnants. Seropurulent umbilical discharge or painful swelling in the lower abdominal midline must be examined by US for the existence of a patent urachus and opening in the umbilical region of an infected urachal cyst. The urachal remnants should be excised completely because of the risk of recurrent inflammation and malignant degeneration. The traditional surgical approach for dissecting an urachal remnant uses a transverse or midline incision in the lower abdomen. A large incision allows better visualization for resection; however, these anomalies are generally benign, requiring only a small incision. An incomplete resection may result because of the limited surgical view that a small incision allows. In this regard, laparoscopic observation offers an excellent panoramic view of the whole lesion, independent of the wound length, thereby enabling appropriate assessment of the extent of the urachal remnant. Some authors have suggested that resection of umbilical urachal remnants, which communicate with the urinary bladder, could benefit from the laparoscopic approach. Our presented cases strongly support the proposal that laparoscopy excision of urachal remnants in children allows for not only cosmesis but also better visualization and recognition of distal urachal remnants; with its magnification effect, complete removal is not difficult. Laparoscopic excision of urachal anomalies will minimize invasiveness and achieve more certain surgical outcome in small incisions than that in the open procedure.
In Case 5, we could not distinguish preoperatively the large urachal cysts on the bladder dome from the salpinx cysts, despite the assessment by MRI. In some cases of urachal remnants, a preoperative definitive diagnosis could not be obtained. 9 Even if the preoperative diagnosis was uncertain, the correct diagnosis and the right treatment would be performed by the laparoscopic approach with its excellent panoramatic view. The laparoscopic technique would be a better option for such cases.
Cases of trocar placement without a visible umbilical site have been reported.2–4 In our methods, the periumbilical urachal remnant was initially dissected through a semicircular infraumbilical incision, free from abdominal fascia. Next, a port was inserted from an umbilical wound. An umbilical insertion provides better postoperative cosmesis without interference with the operative procedure. No postoperative complications were encountered.
The laparoscopic approach appears to be a safe, effective, and cosmetically beneficial alternative to usual open surgery for urachal remnants that require dissection from the bladder dome. Given that most urachal anomalies in young patients are benign, the cosmetic outcome is important to these patients and their parents. 6 Laparoscopic resection is minimally invasive, allowing for complete excision of urachal remnants without difficulty.
Footnotes
Disclosure Statement
No competing financial interests exist.