
Abstract
Abstract
Background:
The treatment of cholecystocholedochal lithiasis (CCL) requires cholecystectomy and common bile duct (CBD) clearance, which can be achieved surgically or with a combination of surgery and endoscopy. The latter includes a two-stage-approach—preoperative retrograde cholangiography (ERC) and sphincterotomy (ST) followed by delayed laparoscopic cholecystectomy (LC), or vice versa—or a one-stage-approach—the rendezvous technique (RVT), where ERC, ST, and LC are performed during the same procedure. No data on the use of RVT in octogenarians have been reported in the literature so far. The study aims to show whether the RVT is as effective in elderly as in younger patients. Moreover, results of RVT are compared with those of a two-stage sequential treatment (TSST) in octogenarians, to identify the best approach to such a population.
Subjects and Methods:
Prospectively collected data of 131 consecutive patients undergoing RVT for biliary tract stone disease were retrospectively analyzed. Two analyses were performed: (1) results of RVT (operative time, conversion rate, CBD clearance, morbidity/mortality, hospital stay, costs, and need for further endoscopy) were compared between octogenarians and younger patients, and (2) results of RVT in the elderly were compared with those of 27 octogenarians undergoing TSST for CCL.
Results:
Octogenarians undergoing RVT were in poorer general condition (P<.0001) and had a higher conversion rate (P<.0001) and a longer hospital stay (P<.007) than younger patients. No differences in the rates of CBD clearance, surgery-related morbidity, mortality, and costs were recorded. Although octogenarians undergoing RVT were in poorer general condition than those undergoing TSST, the results of the two approaches were similar.
Conclusions:
RVT in the elderly seems to be as cost-effective as in younger patients; nevertheless, it may lead to a higher conversion rate and longer hospital stay. In octogenarians, RVT is not inferior to TSST in the treatment of CCL even for patients in poor condition.
Introduction
T
Since the 1980s, the two-stage sequential treatment (TSST) has gained widespread usage because of the lower morbidity rate12,13 compared with open surgery, although the latter was reported to achieve higher rates of CBD clearance. 14 We have proven that TSST is safe and effective not only in young patients but also in octogenarians. 15 By the 1990s, the totally laparoscopic treatment of both CBD stones (CBDS) and gallbladder stones was shown to be superior to TSST in terms of morbidity, mortality, CBD clearance, and costs,16–19 although it is technically a more demanding procedure, requiring specific training and costly, dedicated instruments. More recently, RVT was introduced and has gained popularity as it is reported to be safe and effective in the general population.8,9,20 Unfortunately, the literature is lacking regarding the use of RVT in the very elderly.
In the present study we compared early and late results of RVT between patients younger and older than 80 years of age. Moreover, in order to identify the best approach to the very old patients, the outcome of the elderly group was compared with that achieved with TSST, in a similar population of octogenarians.
Subjects and Methods
From April 2005 until December 2008, 136 consecutive patients with biliary tract stone disease underwent RVT at the Department of Surgery of the Hospital of Guastalla, Guastalla, Italy. Upon admission all patients underwent clinical examination and laboratory tests, including liver function tests (LFTs) and abdominal ultrasound (US). Those with clinical signs and symptoms of biliary colic or acute cholecystitis, abnormal LFTs, and proven gallstones at US were scheduled for an LC and intraoperative cholangiogram (IOC). The same procedure was used for those with proven CBDS at US. Conversely, patients admitted with clinical/laboratory signs of obstructive jaundice or with dilated intrahepatic bile ducts at US underwent instead an abdominal computed tomography (CT) scan to rule out other hepatobiliopancreatic diseases. Finally, all cases of new onset of acute pancreatitis (AP) had also a CT scan, and patients diagnosed with mild biliary AP were scheduled for RVT (Fig. 1). Magnetic resonance imaging (MRI) was done instead when US was negative despite the persistent clinical/laboratory suspicion of CBDS. In 1 case where MRI was inconclusive, we used endoscopic US to detect CBDS.
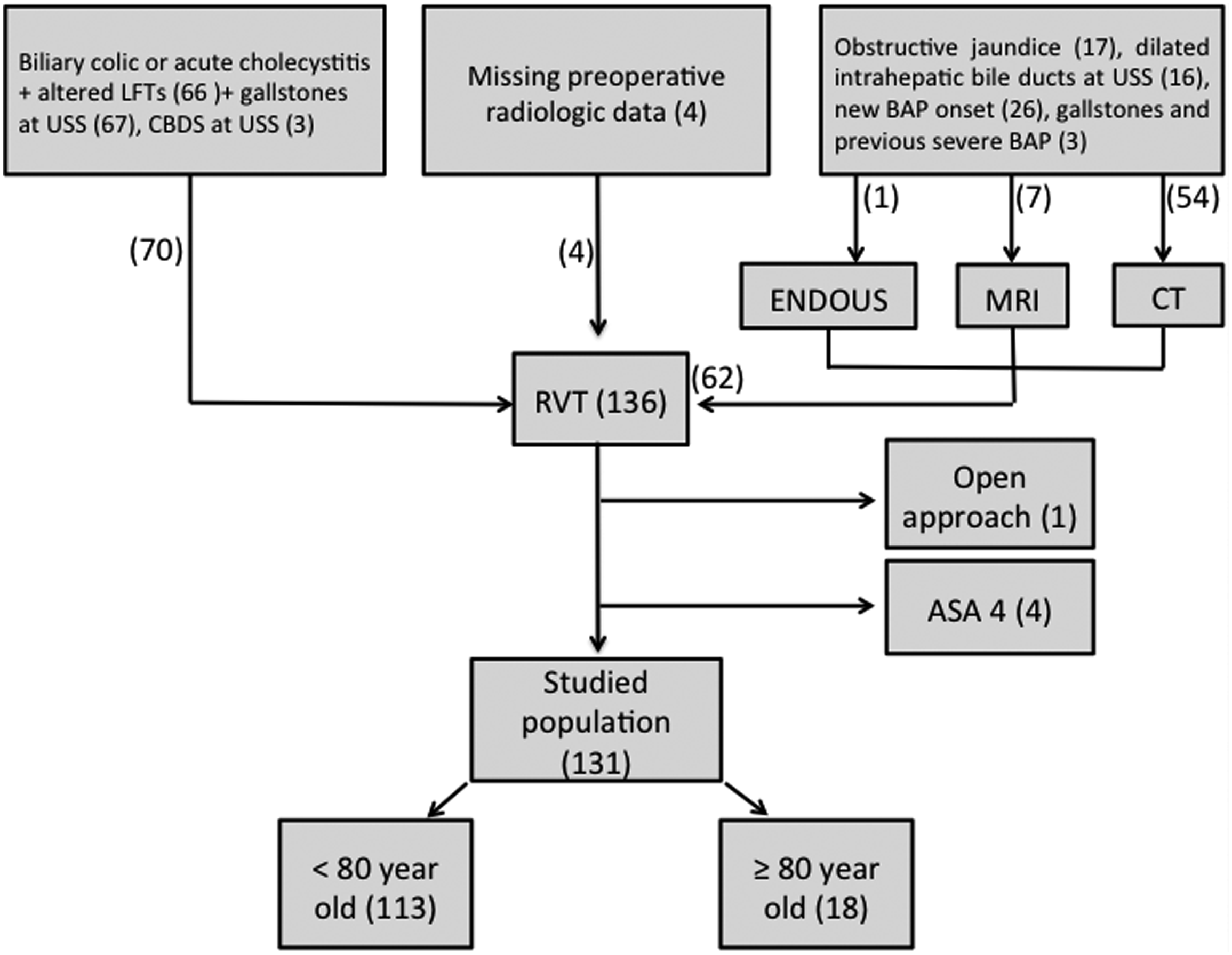
Patient selection (patients undergoing the rendezvous technique [RVT]). ASA, American Society of Anesthesiologists; BAP, biliary acute pancreatitis; CBDS, common bile duct stones; CT, computed tomography; ENDOUS, endoscopic ultrasound; LFTs, liver function tests; MRI, magnetic resonance imaging. USS, ultrasound scan.
Exclusion criteria from the study were an American Society of Anesthesiologists (ASA) class of 4 and/or planned open surgery. Finally, 131 patients were included (Fig. 1).
All the RVT procedures were done by two surgeons with experience in both laparoscopic surgery and digestive endoscopy. The technique consists of a laparoscopic access first, including the dissection and the opening of the cystic duct, through which a guidewire is passed to the duodenum. Before endoscopy, a soft laparoscopic clamp is used to close the lumen of the first jejunal loop, in order to avoid massive small bowel air insufflation during endoscopy, which may hamper further laparoscopic view. Then a flexible endoscope is advanced to the duodenum, where the guidewire is encountered and caught in order to allow the correct endoscopic cannulation of the papilla major for further contrast dye injection, IOC, and placement of the papillotome for ST. After the endoscopic instruments and the guidewire are withdrawn, a formal LC is performed.
At our institution the policy to perform the ST after IOC is as follows: if the IOC shows no stones, the contrast dye flows smoothly to the duodenum, and preoperative LFTs are improved, no further ST is performed. In the case of actual or previous biliary AP, the ST is instead done even if the IOC findings are normal. If IOC shows no CBDS but there is dye contrast filling of the pancreatic duct, suboptimal duodenography, or persistently altered LFTs, the ST is then performed.
According to our policy, if we fail in obtaining clearance of the CBD through the retrograde approach, we proceed to laparoscopic CBD clearance with a choledochoscope and stone retrieval by a Dormia basket through a 12-mm disposable trocar. If choledochoscopy fails, the procedure is converted, and a classic open CBD exploration is performed through a longitudinal choledochotomy. After CBD clearance by (laparoscopic or open) exploration is achieved, the CBD is closed with interrupted sutures, and a pericholedochal drain is routinely placed.
In 4 patients, RVT was performed together with another procedure: laparoscopic splenectomy for a hematologic disease (n=1), laparoscopic ventral hernia mesh repair (n=1), open groin hernia mesh repair (n=1), and open umbilical hernia mesh repair (n=1). All patients were younger than 80 years of age.
Analysis of RVT for patients <80 years old (Group 1) versus ≥80 years old (Group 2)
Patients were divided in two age-based groups as follows: <80 years old (Group 1) and ≥80 years old (Group 2). Data concerning comorbidities and general health conditions, preoperative number of CBDS, rate of CBDS finding at IOC, operative time, rate of conversion to open surgery, rate of CBD clearance, length of hospital stay, surgery-related morbidity and mortality, costs, and need for further ERC were retrospectively compared between the two groups.
Perioperative morbidity and mortality were considered to occur up to 30 days after surgery. Therefore late mortality and complications were defined as occurring beyond this time frame.
The cost analysis between Groups 1 and 2 included costs of laparoscopic and endoscopic tools, the utilization of the operating theater, and hospitalization.
All patients underwent clinical evaluation 1 month after surgery, and by the end of 2011, they (or their relatives or their family physicians) were contacted by telephone. Death events were censored at last follow-up.
Analysis of octagenarians (≥80 years old) for results of RVT (Group 2) versus TSST (Group 3)
Results of RVT in the elderly group (Group 2) were retrospectively compared with those of 27 consecutive octogenarians who received TSST for CBDS (Group 3) between January 1991 and December 1997 at the Department of Surgery of the Hospital of Parma, Parma, Italy. The latter series belong to an already published study comparing the results of TSST versus those of ERC and ST without LC in octogenarians with CBDS. 15
At Parma Hospital, the diagnostic algorithm of biliary tract stone disease was the same of that followed at Guastalla Hospital, including the routine use of MRI when CBDS were suspected but not confirmed at US and/or laboratory tests.
Group 3 patients underwent preoperative ERC and endoscopic ST, followed by LC as soon as possible according to the operating schedule. All of the patients were admitted to the hospital after ERC/ST; therefore the “total” hospital stay after TSST included that following endoscopy and surgery and the delay between them.
Statistical analysis
For statistical analysis, differences in frequencies were evaluated by the chi-squared and Fisher's exact tests, whereas differences in the means between two groups were assessed by Student's t test. Two-tailed P values were used, and values of <.05 were defined as indicating significant differences. Data were analyzed with SPSS® version 20 software (IBM, Armonk, NY).
Results
RVT in Group 1 (<80 years old) versus Group 2 (≥80 years old)
Comparison, including preoperative, operative, and outcome data, of groups is reported in Table 1. Follow-up was completed in 108 cases (82.4%), and its mean length was 52 months (range, 1–81 months).
By chi-squared test except as indicated.
Significant difference.
Preoperative data for 4 patients are missing.
By Student's t test.
By Fisher's exact test.
ASA, American Society of Anesthesiologists; CBDS, common bile duct stones; M:F, males:females.
Demographic data
The mean age was 59.1 years (median, 65 years; range, 21–92 years). There were 73 women and 58 men (P=.907). There were 113 patients younger than 80 years of age (Group 1), and there were 18 octogenarians (Group 2). Comorbidities were detected in 69 patients (52.7%) overall. These consisted of cardiovascular diseases (n=57), hematologic disorders (n=4), chronic pulmonary obstructive disease (n=2), hypothyroidism (n=2), type 2 diabetes (n=3), and morbid obesity (n=1). There were 56 cases in Group 1 and 13 in Group 2. Thirty-six patients were ASA 3 (27.4%): 22 in Group 1 and 14 in Group 2 (P<.0001).
Number of CBDS at preoperative radiology
Preoperative radiology data were missing for 4 patients from Group 1. Overall preoperative radiology showed CBDS in 21 of the remaining 127 (16.5%) cases: 16 in Group 1 and 5 in Group 2 (P=.712). CBDS were detected by abdominal US (n=3), CT (n=16), MRI (n=1), and endoscopic US (n=1). A single stone in the CBD occurred in 3 cases, sludge in 2 other cases, and multiple stones in 16 cases. Microlithiasis (stone diameter, <3 mm) was detected only in an 81-year-old patient. A dilated biliary tree without CBDS was found in 17 other patients (13.4%).
Operative time and conversion to open surgery
Median operative time was 135 minutes (range, 58–405 minutes) overall: 135 and 125 minutes in Groups 1 and 2, respectively (P=.602). Conversion to laparotomy was necessary in 5 patients (3.8%): 3 patients from Group 1 (iatrogenic CBD injury in 1 case, intense Calot's triangle inflammation in 1 case, and adhesions in another) and 2 patients from Group 2 (intense Calot's triangle inflammation in 1 patient and adhesions in the other) (95% confidence interval –89.9 to 214.2; P=.139).
CBD clearance
IOC findings were abnormal in 127 of the 131 patients (96.9%). CBDS were detected in 103 cases (81.1%): 89 in Group 1 and 14 in Group 2 (P=1.000). In the remainder findings were of dilatation of the CBD in 3 patients, stenosis of the CBD in 15 patients, and dye contrast filling of the pancreatic duct in 6 patients. In 4 patients in Group 1 the IOC was normal: 3 had a new onset of biliary AP, and 1 had acute cholecystitis and persistently raised LFTs.
All the 131 patients underwent ST. Clearance of stones or sludge from the CBD was successful in all but 1 patient (P=.136). In an 85-year-old patient (ASA 3) with obstructive jaundice, RVT failed. In that case the procedure was converted to laparotomy because of technical difficulty (intense Calot's triangle inflammation); open RVT was attempted, but the CBD was not completely cleared, and the subsequent open choledochoscopy through the cystic duct failed as well. Because there were anesthetic concerns, a formal CBD exploration through a choledochotomy was avoided, and a transcystic duct drain was placed. On postoperative Day 13 ERC was repeated in this patient, and the procedure showed several stones in the distal CBD with a normal opacification of the duodenum. The transcystic duct drain was removed soon after the second ERC, and because the following postoperative course was uneventful and jaundice subsided completely, no other invasive procedure was attempted. At follow-up, the patient did not show any further signs or symptoms related to choledochal lithiasis.
Mortality
At last follow-up, 9 of 108 (8.3%) patients have died overall: 2 in Group 1 and 7 in Group 2. No perioperative mortality has occurred in Group 1, although a 80-year-old female patient (ASA 2) undergoing RVT died 1 week after surgery because of hemorrhagic stroke (P=.137). She was admitted with AP and cholangitis and had a medical history of dementia on a vascular basis. There were no intraoperative difficulties, and the operative time was 195 minutes. Postoperatively serum laboratory tests showed only persistently raised amylase levels (on Days 3 and 5), whereas clinical findings were unremarkable. Because the patient recovered well from surgery, on postoperative Day 6 she was transferred to a medical rehabilitation ward, where she suddenly died following a hemorrhagic stroke the day after.
There were no late endoscopy/surgery-related deaths in either group. Causes of (RVT-unrelated) late mortality were acute myocardial infarction (n=1) and gastric cancer (n=1) in Group 1 and senectus (n=4), heart failure (n=1), and end-stage renal failure (n=1) in Group 2.
Morbidity
Perioperative complications occurred in 20 (15.3%) patients (Tables 1 and 2). There were 16 cases in Group 1 and 4 in Group 2 (P=.941). One patient in Group 1 presented persistent obstructive jaundice for 13 days after surgery. Postoperative MRI on Day 10 showed a CBD stricture, which was treated by endoscopic biliary stenting. A biliary leak developed in 4 cases (2 in Group 1 and 2 in Group 2) as the result of an iatrogenic perforation of the distal CBD during the use of the Dormia basket to retrieve CBDS. In 1 case the lesion was discovered intraoperatively and managed by conversion to open surgery (see above) and Kehr tube positioning; the other 3 cases were treated conservatively (drainage).
The patient died 7 days postoperatively.
Four patients in Group 1 developed late surgery-related complications, whereas none did so in Group 2 (P=1.000). Two patients suffered from chronic pain in the right upper abdominal quadrant, which required referral to the Pain Service, and 2 had an incisional hernia at the umbilical port site, which was treated surgically 7 and 12 months after surgery, respectively.
Hospital stay and costs
The median hospital stay was 4 days (range, 2–75 days), and it was longer in Group 2 (P<.007). Table 3 shows the cost of both laparoscopic and endoscopic tools used to perform the RVT. As shown in Table 4, cost analysis between Groups 1 and 2 did not show any difference (P=.712).
Reusable instrument. The cost is calculated on a basis of 100 operations done plus 15% (rough cost estimate of instrument servicing, repair, sterilization, storage).
Disposable instrument.
The cost is calculated on a basis of 150 procedures done.
The cost is calculated on a basis of 3000 procedures/year×5-year usage.
The cost is calculated on a basis of 300 procedures/year×5-year usage.
By Student's t test.
Costs include those of personnel, furniture, anesthetic instruments, surgical instruments, sterilization, cleaning, and utilities.
Cost per minute.
Median operating time (minutes).
Daily hospital stay cost.
Median hospital stay (days).
Further endoscopic procedures
Further endoscopic procedures were needed in 1 case in each group (P=.257). As discussed above, the reasons of those were persistent jaundice due to common hepatic duct stricture and failed CBD clearance, respectively.
Octogenarians: RVT (Group 2) versus TSST (Group 3)
Preoperative, operative, and outcome data are reported in Table 5. Mean follow-up of Group 3 patients was 126 months (range, 89–158 months).
By chi-squared test, except as indicated.
Significant difference.
By Student's t test.
By Fisher's exact test.
ASA, American Society of Anesthesiologists; DNA, does not apply; ERC, endoscopic retrograde cholangiography; LC, laparoscopic cholecystectomy; M:F, males:females; NS, not significant; RVT, rendezvous technique; ST, sphincterotomy.
Demographic data
Demographic data were similar between the two groups except for ASA score: 14 patients in Group 2 and 7 in Group 3 were ASA class 3 (P=.0431). None of the patients from Group 3 was admitted with biliary AP.
Delay of surgery (Group 3)
For patients undergoing TSST median delay of surgery was 5 days (range, 1–31 days). The majority of them (n=25) stayed in the hospital between endoscopy and surgery. Twenty-one (77.8%) underwent LC 5–10 days after ERC. That delay was mainly due to the synchronization of endoscopic and surgical schedules and the lack of surgical beds to accommodate patients after LC. Longer delays between surgery and endoscopy were attributable to the evaluation of high surgical risk (ASA 3), unclear biliary features at ERC pancreatography, or abnormal LFTs needing further preoperative evaluation.
Operative time and conversion to open surgery
Median total operative time (including the duration of both preoperative ERC/ST and LC in the TSST group) was 125 minutes (range, 58–275 minutes) in Group 2 and 137 minutes (range, 67–259 minutes) in Group 3 (P=.4563). Two patients from Group 2 and 4 patients from Group 3 underwent conversion to open surgery (P=.9980).
CBD clearance
As reported above, intraoperative ERC failed in obtaining CBD clearance in 1 patient from Group 2, whereas preoperative ERC was successful in all the cases from Group 3 (P=.4000).
Mortality
At last follow-up, 7 patients in Group 2 (38.9%) and 15 in Group 3 (55%) have died. One patient from Group 2 died 1 week after surgery because of a hemorrhagic stroke, as reported above. No perioperative mortality has occurred in Group 3 (P=.4000). No late surgery- and endoscopy-related mortality occurred in either group.
Morbidity
As shown in Table 2, perioperative complications occurred in 4 patients from Group 2 (see above) and 4 patients from Group 3 (P=.9820). Late surgery- and endoscopic-related complications occurred in 1 patient from Group 3 (P=.6000), who developed an incisional hernia that was treated laparoscopically.
Hospital stay and costs
Median total hospital stay was 6 days in both Group 2 and Group 3 (P=.9336). As shown in Table 6, cost analysis did not show any significant difference between RVT and TSST in octogenarians (P=.9301).
By Student's t test.
Costs (euros) include those of personnel, furniture, anesthetic instruments, surgical instruments, sterilization, cleaning, and utilities.
Cost (euros) per minute.
Median operating/endoscopy time (minutes).
Costs include those of personnel, furniture, anesthetic instruments, sterilization, cleaning, and utilities.
Daily hospital stay cost (euros) in the gastroenterology ward.
Median delay of surgery (days) after endoscopic retrograde cholangiography.
Daily hospital stay cost (euros) in the surgical ward.
Median hospital stay (days) after laparoscopic cholecystectomy.
DNA, does not apply.
Further endoscopic procedures
As noted above, 1 patient from Group 2 underwent further ERC 13 days after surgery because of failed CBD clearance. One patient from Group 3 needed also further ERC and biliary stenting 35 months after surgery (P=.645). This 84-year-old man developed jaundice related to a cephalopancreatic cancer and died 8 months after endoscopy.
Discussion
Choledochal lithiasis represents a relatively common clinical finding in patients with gallbladder lithiasis and requires both CBD clearance and cholecystectomy. 1 Recent progress in laparoscopic surgery and endoscopic techniques has rekindled the debate concerning the most appropriate management of this condition.12,14,16–25
The combined TSST approach is still widely used because of its advantages as a mini-invasive approach without the need of specific laparoscopic skills and dedicated instruments.3–6,26,27 Nevertheless, this technique has showed morbidity, mortality, and costs higher than a totally laparoscopic approach.16–19 Moreover, it implies two hospital stays or, if a single hospitalization is considered, an optimal integration of endoscopy and surgery schedules.
A totally surgical approach has the main advantage of a single hospital admittance, procedure, and general anesthesia.14,25,28 A totally laparoscopic management of CCL has proven to be as effective as open surgery with fewer postoperative complications,22,24,25,29,30 but, owing to the need of advanced technical skills and dedicated equipment, it has had limited usage up to now.
The RVT, first described by Cavina et al., 8 is a single-stage surgical/endoscopic approach to manage CCL that has been reported to be more effective than TSST because it is associated with higher CBD clearance rate, lower morbidity, shorter hospital stay,9,20 and reduced hospital costs. 20 Such good results may be explained by the specific technique itself because RVT implies the anterograde passage of a guidewire through the cystic duct to the duodenum before the ERC and the ST are performed. This maneuver allows a safer endoscopic cannulation of the papilla major, thus possibly reducing the rate of iatrogenic acute pancreatitis. 10 Indeed, the downside of the RVT is that it requires specific equipment and dedicated personnel. Because both endoscopy and laparoscopy are performed synchronously, a second operator (endoscopist or endoscopy-trained surgeon) and adequately trained personnel, as well as an appropriately prepared theater (endoscopic and laparoscopic instruments, etc.), are needed at the same time.
Although several authors have reported encouraging results of RVT in the general population,10,12,14 unfortunately, the literature on RVT in the elderly is lacking. In our experience, RVT in octogenarians was as safe and effective as in younger populations. In the present study, octogenarians showed a higher rate of conversion to laparotomy. Although, theoretically, it may be hypothesized that an older patient may have a more long-lasting CCL, which may somehow increase the difficulty of the procedure (for example, by worsening tissue inflammation/scarring at Calot's triangle, etc.), and age and poorer condition of the patients may also lead the operating surgeon not to postpone conversion, we are instead inclined to believe that a numerical bias (the small size of Group 2) may be responsible for such values.
It is significant that the only failure of RVT in obtaining a complete CBD clearance was recorded in Group 2, where the poor general condition of the patients prevented us from performing a further CBD exploration through a choledochotomy.
Perioperative mortality occurred in an 80-year-old patient as the result of an acute cardiovascular event. Nevertheless, a similar rate of perioperative complications in Group 1 and Group 2 seems to confirm the safety of RVT in octogenarians.
The hospital stay was longer among octogenarians. We could explain that as the result of several aspects. First, the octogenarians had more comorbidities; hence we adopted a more cautious attitude with regard to early discharge. Second, all of them were discharged home, and some had social issues that had to be addressed.
Further endoscopy was needed in 2 cases. In the 60 year-old patient whose jaundice persisted up to 13 days postoperatively requiring further biliary stenting—despite a good CBD clearance during the intraoperative ERC—we retrospectively argue that a preoperatively undiagnosed biliary stricture was already present at surgery rather than developed postoperatively. The second was the case of the 85-year-old whose RVT and CBD clearance failed (see above).
No late surgery/endoscopy-related deaths occurred in either group, although, interestingly, late surgery-related complications were recorded only among patients from Group 1. Possibly, a more active lifestyle of younger patients may be supposed to play a role in late morbidity (at least in the occurrence of incisional hernias), but we are instead inclined to believe that the small Group 2 population biased that value.
Cost comparison showed no difference between octogenarians and younger patients, as the only relevant cost difference between the two groups concerned the hospital stay, which was longer for the older patients.
In order to show the real safety and effectiveness of RVT in the elderly, we also compared the results of Group 2 with those of octogenarians undergoing treatment of cholecystocholedochal disease by TSST.
Small population size, retrospective analysis, and comparison of two different approaches in two different environments are definitely potential biases of this study.
Patients from Group 2 showed a significant higher percentage ASA 3 score; moreover, none of those from Group 3 had biliary AP. In the light of such a difference, it is in our opinion remarkable that the results in Groups 2 and 3 were in the end similar. In fact, conversion rates were almost the same in the two groups, as well as the success rate, and the total operative time (including that needed to perform ERC/ST in Group 3) did not differ between the two groups.
Both perioperative and late morbidity rates were also similar in the two groups; however, biliary leak occurred only in patients undergoing RVT. Clearly, our series cannot exhaustively explain why such a complication occurred in the RVT and not in the TSST group. To our knowledge, only 1 case of postoperative biliary leak after RVT has been reported in the literature and was due to a retroperitoneal perforation during ST. 9
Octogenarians undergoing RVT remained in the hospital longer than those having TSST. That result differs from other series—all including patients up to 75 years of age9,20—where RVT carried a shorter postoperative hospital stay than TSST. We may argue that the higher ASA 3 score rate and preoperative diagnosis of biliary AP in Group 2 may account for such a difference with the literature, but instead we believe that the occurrence of two long-lasting postoperative complications (biliary leak) may partially explain this vlaue in a relatively small-sized group.
It is interestingly that such a difference observed in postoperative (postsurgical) stay virtually disappeared when we consider the “total” hospital stay, including, in Group 3, the delay between ERCP/ST and LC. In fact, a median 5-day delay between ERC and LC has been recorded in Group 3. As described above, theater schedules, patients' general conditions requiring further anesthetic assessment, and need for further diagnostic tests accounted for such a long delay. Unfortunately, our hospital policy did not provide for a temporary transfer of the patients to a medical ward while waiting for surgery, where perhaps costs could have been less.
With regard to the cost analysis, in contrast with recent literature in the general population, 20 we found that in octogenarians RVT is as expensive as TSST. Both the prolonged operating time (thus increasing the cost of theater utilization) and postoperative stay did not allow the RVT protocol to reduce costs compared with the TSST.
The strength of this article is that it is the first to quantify the results of RVT in octogenarians compared with those obtained in younger patients and with those achieved in the same population by the management of CCL used most frequently nowadays in Europe, the sequential approach by ERC/ST followed by LC.
In conclusion, despite a prolonged hospital stay, our study shows RVT as being as safe and effective in octogenarians affected by CCL as in younger patients. RVT results are also comparable with those of TSST in octogenarians. However, the retrospective nature of the study, a small population size, and short follow-up do not allow for definitive conclusions. Only a prospective randomized trial might trace recommendations for the use of the RVT in the treatment of CCL in octogenarians.
Footnotes
Acknowledgments
The authors thank Dr. Antonio Ventura and Anna Maria Forestiero of the Controllo di Gestione of the University Hospital of Parma, Parma, Italy.
Disclosure Statement
No competing financial interests exist.