
Abstract
Abstract
Introduction:
Gastrojejunostomy (GJ) tubes are an option for durable enteral access for critically ill infants with congenital cardiac disease who struggle with obtaining adequate nutrition.
Materials and Methods:
Infants weighing less than 10 kg with cardiac disease who received placement of a laparoscopic GJ tube from November 2011 to January 2015 were reviewed. The operative technique used an umbilical port for the camera and a single stab incision for the gastric access site. After insufflation to 5–8 mm Hg, the stomach was suspended to the abdominal wall, after which a dilator was maneuvered into a postpyloric position using laparoscopic visualization and fluoroscopy, and a glidewire was passed into the duodenum. The GJ tube was then fluoroscopically threaded over the glidewire; final position was confirmed by contrast injection.
Results:
There were 32 laparoscopic GJ tube placement operations performed; 7 (21.9%) of these tubes were standard single-unit GJ tubes, and 25 (78.1%) were low-profile gastrostomy tubes modified with a nasojejunal feeding tube threaded through the feeding port. Median patient age was 3.5 months (range, 0.75–11 months), with a median weight of 4.2 kg (range, 2.4–7.4 kg). Congenital defects were varied, including hypoplastic left heart syndrome and pulmonary vein stenosis. Median operative time was 62 minutes for isolated GJ placement (range, 35–114 minutes). There were three postoperative complications, resulting in a 30-day complication rate of 9.4%. Thirty-day mortality was 9.4% with no mortality related to the operation.
Conclusions:
Laparoscopic GJ tube placement may be performed safely in infants with cardiac disease and allows these patients to receive adequate nutrition despite intolerance of gastric feeding.
Introduction
I
Intolerance of gastric feeds combined with gastroesophageal reflux can be a common problem for infants with complex cardiac lesions. 3 Additional comorbid conditions that can complicate the infant's ability to tolerate gastric feedings include aspiration related to vocal cord dysfunction or neurologic injury, as well as lung disease related to either prematurity or the underlying cardiac defect.4,5 The primary options for these patients unable to tolerate gastric feedings are fundoplication or postpyloric feeding. At our institution, we have increasingly relied on gastrojejunostomy (GJ) feeding tubes to meet the nutritional needs in this population and have sought to develop a safe surgical method for GJ tube placement. This study describes our method of laparoscopic GJ tube placement and reviews our experience with performing this operation in infants with congenital cardiac disease.
Materials and Methods
Patient selection
Institutional Review Board approval was obtained to review operative records for all placements of GJ tubes between November 2011 and January 2015. We identified patients weighing less than 10 kg with congenital cardiac abnormalities who received primary placement of a laparoscopic GJ tube at our institution. Patients who had a prior gastrostomy tube placement that was being exchanged for a GJ tube were excluded.
Clinical variables
Hospital records were reviewed to extract patient age, gestational age, weight, comorbidities, and the indication for tube placement. Outcome measures included operative time, anesthetic and surgical complications within 30 days, postoperative length of stay, and 30-day mortality. Operative time was defined as incision time to surgery end. In instances where the GJ placement occurred with the patient under the same anesthetic as for another procedure/operation, total time was listed. There were a few cases in which the time for each separate operation was specified; in these instances, the time documented for the GJ tube placement was used.
Operative description
The operative technique used an umbilical port for the camera and a single stab incision for the gastric access site. After insufflation to 5–8 mm Hg, the stomach was suspended by two sutures placed with tiny skin openings that allowed the knots to be tied in the subcutaneous space. Stomach access and dilation occurred by the Seldinger technique. Once the stomach was secured to the abdominal wall, the dilator was maneuvered into a postpyloric position using laparoscopic visualization and fluoroscopic confirmation, and a 0.035 inch stiff glidewire was passed into the duodenum. The GJ tube was then threaded over the glidewire under fluoroscopy. Its final position was confirmed by contrast injection (Fig. 1; video [http://online.liebertpub.com/doi/full/10.1089/vor.2015.0277]>). GJ tubes placed were either standard single-unit GJ tubes (MIC* gastric jejunal feeding tube [Halyard Health, Alpharetta, GA] or G-JET® gastric-jejunal tube [Applied Medical Technology, Inc., Brecksville, OH]) or low-profile gastrostomy tubes (MIC-KEY*; Halyard Health) modified with a CORFLO® nasojejunal feeding tube (CORPAK MedSystems, Buffalo Grove, IL) threaded through the feeding port (Fig. 2). The latter type is referred to as a transgastric GJ tube. For transgastric GJ tubes, the nasojejunal tube is threaded through the GT feeding port prior to advancing the tubes over the glidewire as a single unit. After confirmation of placement, the gastrostomy balloon is inflated with sterile water, and the phlange is secured to the abdominal wall.
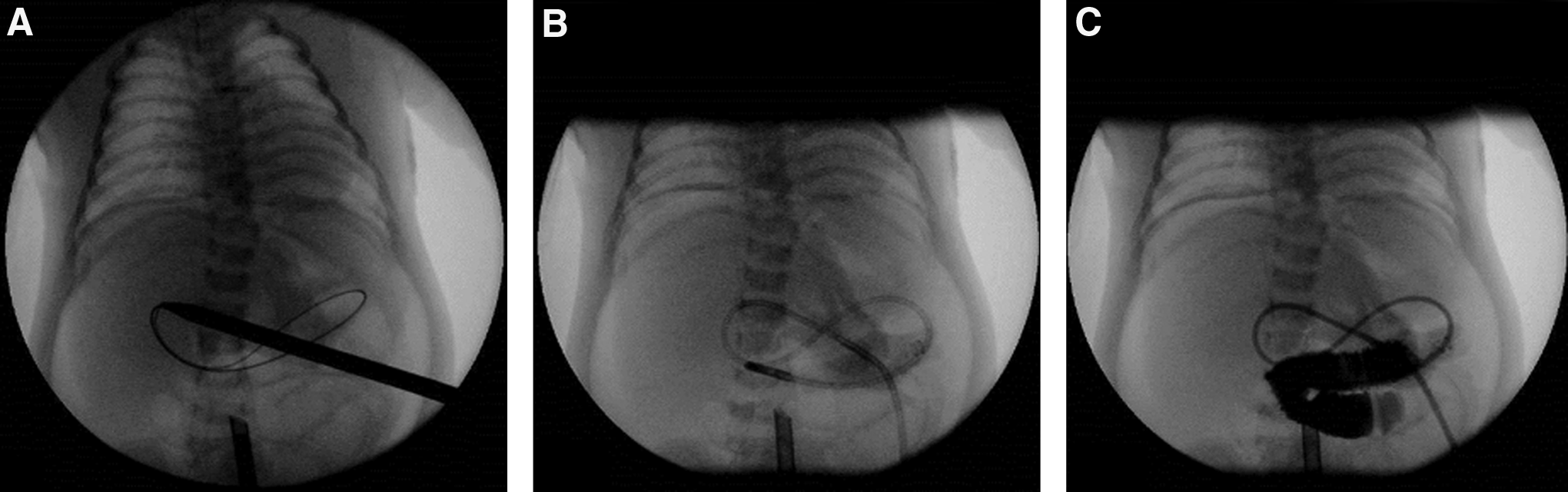
Transgastric gastrojejunostomy placement under fluoroscopic guidance.
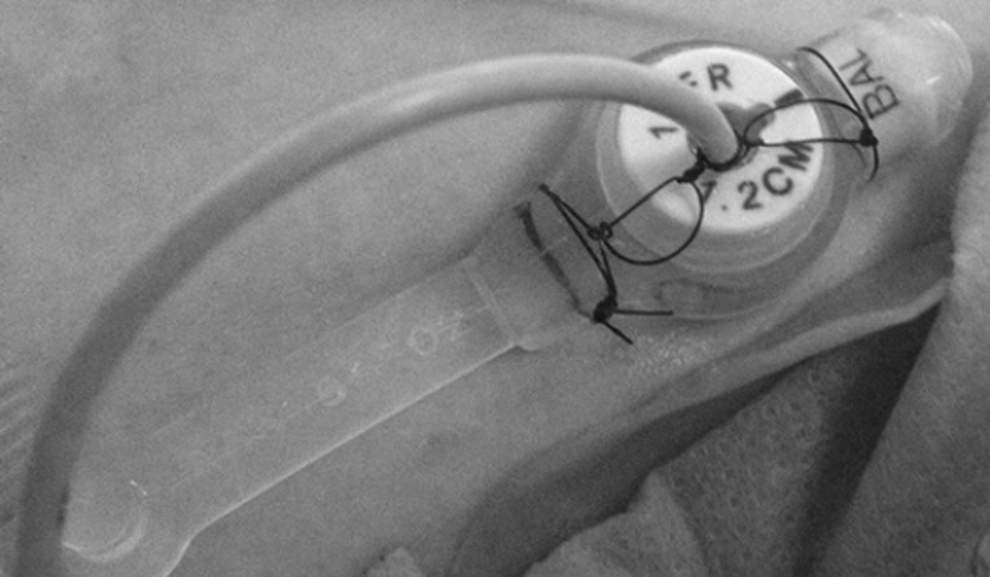
Transgastric gastrojejunostomy. The nasojejunal feeding tube is placed through the feeding port of the gastrostomy button and secured externally at the proper depth with Prolene suture.
Results
There were 32 primary laparoscopic GJ tube placed in infants with cardiac disease between November 2011 and January 2015; 7 (21.9%) of these tubes were standard single-unit GJ tubes, and 25 (78.1%) were transgastric GJ tubes (Table 1). Median patient age was 3.5 (range, 0.75–11) months, with a gestational age at birth of 38 (range, 24–40) weeks. Male patients made up 59.4% of the population, and median weight was 4.2 (range, 2.7–7.4) kg. Two groups with 7 (21.9%) patients each had either multiple congenital anomalies or isolated hypoplastic left heart syndrome; these were the most common groups in this population. Other anomalies included coarctation of the aorta, anomalous pulmonary venous return, and double-outlet right ventricle (Table 2). The most common indications for GJ placement were gastric feeding intolerance/gastroesophageal reflux (n = 29; 90.6%) and/or aspiration (n = 10; 31.2%) (Table 1).
Data are median (range) values unless indicated otherwise.
GERD, gastroesophageal reflux disease; GJ, gastrojejunostomy.
Median operative time was 68.5 minutes (range, 35–361 minutes) (Table 1). Forty percent of GJ placements were done concurrently with other operations; longer median operative times (62 versus 170 minutes) occurred in patients undergoing multiple concurrent operations. The most common procedure performed with the patient under the same anesthetic was tracheostomy placement (6%). All of the longer cases (>180 minutes) involved at least three procedures. When the GJ placement was the only operation, operative time ranged from 35 to 114 minutes. The operations were carried out by four surgeons, with 90% being performed by a single surgeon (as either the primary or secondary surgeon).
Three patients experienced postoperative complications, resulting in a 30-day complication rate of 9.4%. One patient developed postextubation stridor and a pneumothorax, whereas 2 patients had GJ tube complications related to tube malfunction or migration. Thirty-day mortality was 9.4% (3 patients) with no mortality being related to the GJ tube operation itself (Table 3). Total hospital length of stay was dependent on underlying comorbidities; median postoperative length of stay was 10 days, with 1 patient still remaining hospitalized at the time of this review.
DORV, double-outlet right ventricle; GJ, gastrojejunostomy; POD, postoperative day; PVS, pulmonary vein stenosis.
Discussion
The prioritization of nutritional support for infants with congenital cardiac defects has become paramount in recent years, especially in patients with more complex cardiac lesions such as those with single-ventricle physiology or pulmonary vein stenosis.2,6 Unfortunately, these are the very same patients for whom gastroesophageal reflux and intolerance of gastric feeding methods are quite common; often these same patients also have higher risk factors for aspiration and low tolerance for additional lung insults. Although fundoplication operations, open or laparoscopic, have been used successfully in infants with even the most complex cardiac defects, 7 many cardiac teams are interested in enteral access procedures that would potentially pose the least additional risk possible in terms of operative time and recovery. Nasojejunal feeding tubes can be (and often are) used in these patients, but nasojejunal tubes are best used for short-term enteral access due to risk of dislodgement and the need for frequent replacement. For this purpose, our institution has investigated the use of GJ tubes for postpyloric feeding.
Several options for primary GJ tube placement exist: percutaneous placement via endoscopic and/or fluoroscopic guidance, as well as surgical placement.8,9 For patients with existing gastrostomy tubes, exchange to GJ tubes is a very straightforward fluoroscopic procedure that both is quick and requires minimal if any sedation or anesthesia. For patients without gastric access in place, for whom the need for postpyloric feeding is present from the beginning, the option of primary GJ tube placement is attractive. In this study, we sought to describe our method of primary laparoscopic GJ tube placement, which is a simple modification of standard laparoscopic gastrostomy tube placement. 10 We have found that this procedure can be performed with low laparoscopic insufflation pressures, with acceptable operative times, and without procedure-related mortality, even in a group of very complex cardiac patients. This procedure is based on stable gastrostomy fixation that gives flexibility for primary GJ tube placement, as well as safe GJ tube exchange when needed.
Castle et al. 11 have described a similar method for primary GJ placement using a combination of laparoscopy and endoscopy with good results in their case series. However, here we emphasize the modification of the operation for infants too small for standard single-unit GJ tubes. For patients weighing less than 10 kg, and especially for infants under 5 kg, single-unit GJ tubes can pose additional risks related to the large size of standard GJ tubes—either 14 or 16 French diameter. These large tubes in small infants can cause duodenal or jejunal perforation or can stent open the pylorus to a degree that reflux of postpyloric feeds into the stomach is a common problem. We used a modified transgastric jejunal tube in these cases and have preferred this approach increasingly for infants under 5–6 kg. The 6 French feeding tube inserted through a standard gastrostomy button can be used for infants even under 3 kg, and we have not yet seen any cases of jejunal injury related to these tubes. Additionally, the smaller tube affords placement of longer jejunal tubes that can be positioned past the ligament of Treitz to minimize reflux of feeds back into the stomach (and esophagus). We have also found that clogging of the standard 6 French feeding tube can be easily addressed by water flushing when the side port is clamped to allow power forward flushing with just a few milliliters of water.
Three (9%) patients died within 30 days of their primary GJ tube placement due to their underlying cardiac conditions, which is troublesome. Nevertheless, none of these patients had perioperative instability attributable to either laparoscopic insufflation or enteral tube placement. This mortality certainly underscores the underlying complexity of these patients and the need for close coordination and planning with the cardiac and anesthetic teams. It is our policy to not consider cardiac patients for enteral tube placement until they have medically stabilized to the point that potential discharge home from the hospital is being considered.
Conclusions
This study describes a novel method of primary laparoscopic GJ tube placement that is safe and effective in small infants with complex congenital cardiac disease. These initial results indicate that patient selection and close teamwork with the cardiac and anesthesia groups are critical. Further studies are underway to delineate the long-term outcomes following GJ tube placement and to determine which patients can be successfully transitioned to gastric and/or oral feeds versus those patients who would benefit from fundoplication.
Footnotes
Disclosure Statement
No competing financial interests exist.