
Abstract
Introduction:
Insecure gastropexy, gastric mucosa overgrowth, granulation tissue formation, and a nonhealing gastrostomy are unwanted consequences encountered in the current minimally invasive gastrostomy tube (GT) placement techniques. Aiming to overcome these problems we have developed a simplified laparoscopic-assisted GT insertion (LAG) procedure using guided transabdominal U-stitches (GTU) gastropexy.
Materials and Methods:
We retrospectively reviewed all LAG cases performed in our institute using the GTU technique. In brief, a curved clamp is inserted intragastrically through the laparoscopic port and guides a needle across the abdominal and gastric walls to exit, then re-enter back, through the port in an out-in-out fashion creating multiple spaced transabdominal U-stitches that are tied over pledgets.
Results:
Between March 2008 and January 2015, 31 cases had LAG attempted using GTU. Two cases were converted to open procedures for non–LAG-related reasons. The median age of the remaining 29 cases was 37 (range, 0.3–154.9) months. Of those patients, 20 had fundoplication (LAG-Fundo), whereas the remaining 9 had LAG-only. The mean operative times for LAG-Fundo and LAG-only were 148 ± 57.5 minutes and 41 ± 12.4 minutes, respectively. During a median follow-up of 21 (range, 4–81) months we did not encounter any procedure-related mortality, intraabdominal leaks, or bowel injuries. One patient required redo gastropexy due to unplanned early U-stitch removal, and 7 cases had transient external GT leak, granuloma formation, and/or skin infection.
Conclusions:
GTU can achieve a simple and secure LAG, avoiding the catastrophic complications of intraabdominal leak without the need of special instruments or enlarging the port's wound. Using a smaller wound and intraabdominally placed mucosa helps in minimizing the risk of wound infection and external leak. Transient complications are expected during the earlier phase of the learning curve.
Introduction
The original gastrostomy tube (GT) insertion described by Stamm1 has been widely replaced by minimally invasive procedures such as percutaneous endoscopic gastrostomy (PEG) and laparoscopic GT insertion (LAG). PEG has gained popularity, particularly among nonsurgeons, due to its simplicity, efficiency, and minimal invasiveness.2,3 However, percutaneous transabdominal insertion does not visualize all the procedure's steps, which carries a small but a catastrophic risk of bowel injuries and intraperitoneal leak, 4 particularly in children with distorted anatomy.2,5 Alternatively, LAG is considered relatively safer6,7; this could be attributed to the better visualization it offers. However, the gastropexy technique frequently requires stretching or enlarging the port incision to place purse-string stitches and to fix the stomach to the fascia in a stoma-like fashion, a procedure termed by some authors as a mini-open technique (MOT).6,8–10
Here we describe a simplified technique for secure laparoscopic GT placement under vision using guided transabdominal U-stitches (GTU) through the laparoscopic port without expanding the port or using any special tools.
Patients and Methods
Patients' data
After obtaining the approval of our institution's review board (protocol numbre E-14-1169), we retrospectively reviewed all children who had undergone LAG in our hospital between March 2008 and January 2015. Only cases of LAG using GTU with or without fundoplication were included. Cases that were performed by alternative laparoscopic techniques or converted to open procedures for nonrelated causes were excluded. Data collected from chart review included patients' age, gender, primary diagnosis, the performed procedure, operative time, and postoperative complications. Complications were categorized as major complications (ones that required surgical intervention, including intraabdominal leak or sepsis, stomach–abdominal wall dehiscence, significant persistent paratube leak, and mucosa prolapse requiring revision) and minor complications (which included GT dislodgment, minor transient paratube leak, wound infections requiring antibiotic treatment, and granulation tissue requiring silver nitrate cauterization).
Operative technique
The laparoscopic GT was inserted either as an isolated procedure (LAG-only) or in combination with laparoscopic fundoplication (LAG-Fundo).
In the LAG-only procedure, we usually used two ports: an umbilical 5-mm scope port and a 5-mm working port, which was later used for the GT. In thinner patients who underwent the LAG-only procedure the working port was replaced by a single 5-mm incision placed 2–3 cm below the left costal margin. The anterior wall of the stomach was grasped at the most inferior part of the greater curvature away from the pylorus and exteriorized through the left subcostal wound (Fig. 1a). Clamps were placed at the opposite quadrants of the delivered stomach wall. The stomach was then inflated via a nasogastric tube to stretch the mucosa and to facilitate its puncture with a blunt cautery tip. In patients who did not have fundoplication, adequate stomach inflation here will be difficult to sustain and might require repeated inflation. Once the stomach wall was punctured, a closed clamp was introduced inside the stomach, visualized laparoscopically to confirm its intragastric position, and then cranked against the abdominal wall to facilitate needle guidance.
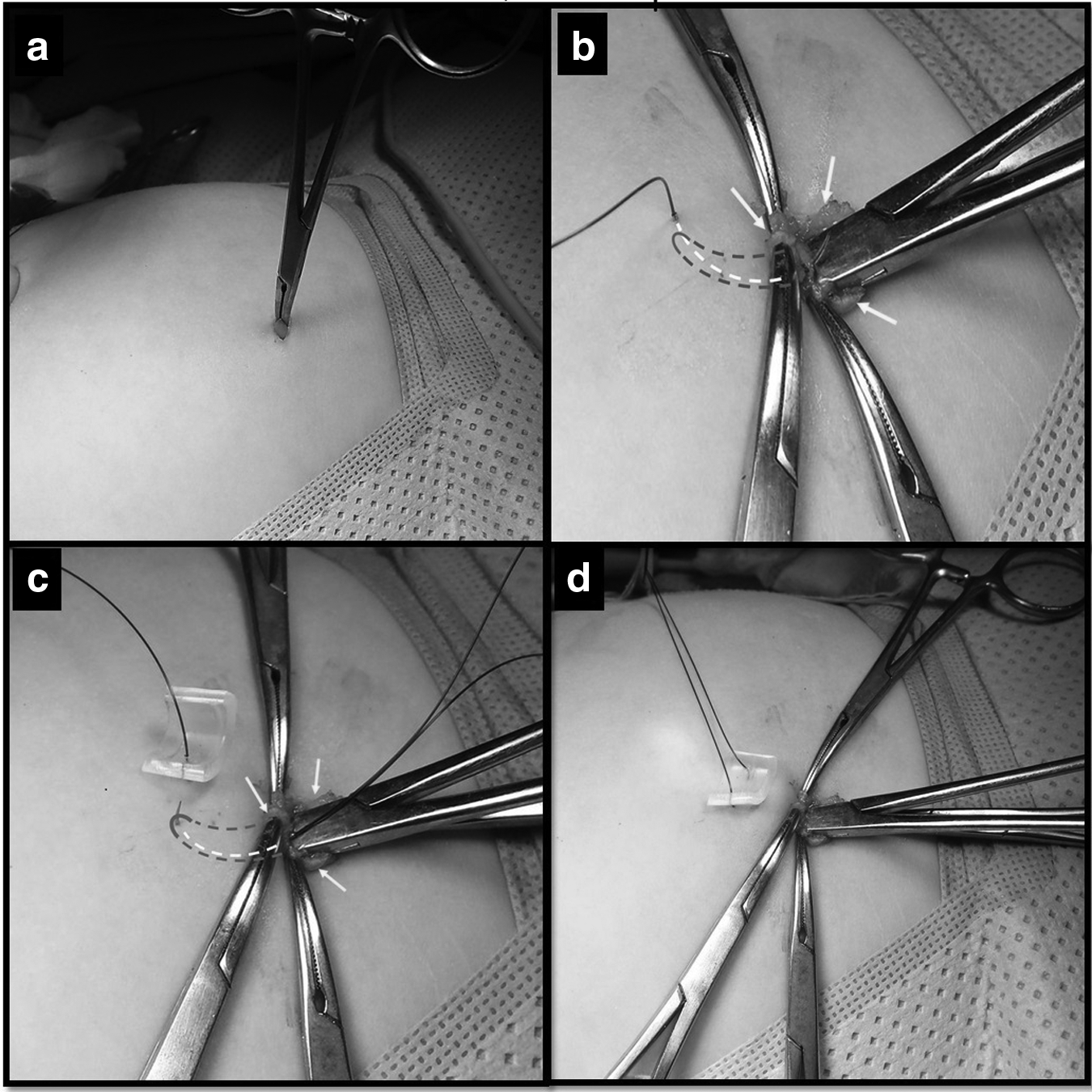
Based on the size of the child, pledget-reinforced 3-0, 2-0, or 0 polydioxanone (PDS®; Ethicon Inc., Somerville, NJ) stitches were used for the transabdominal stitches. Pledgets were cut from silicon Foley catheters. The suture was passed vertically and transabdominally, 1–2 cm from the port hole, until it touched the tip of the intragastric clamp. It was then slid along its curve to exit through the gastrostomy wound (Fig. 1b). Then the needle was flipped, and the suture was passed back into the hole, sliding it back over the clamp to exit to the side of its entry point, leaving a 1–2-cm abdominal wall bridge (Fig. 1c). Finally, it was passed back through the same pledget (Fig. 1d). We often placed three or four U-stitches depending on the size of the patient and the expected tension on the GT.
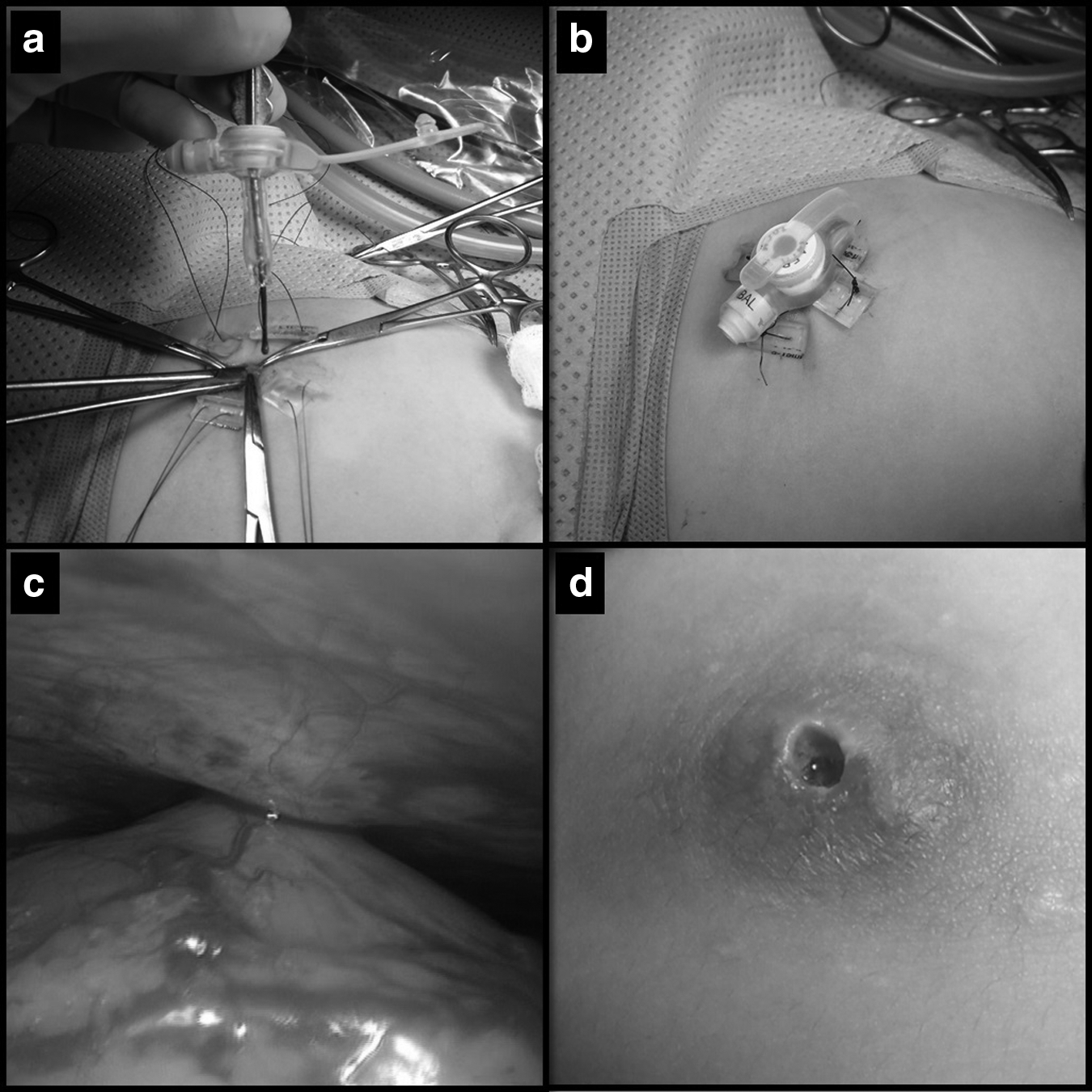
A lacrimal probe was inserted through an appropriate size, low-profile GT (MIC-Key® button; formerly Kimberly-Clark Health Care, now Halyard Health, Alpharetta, GA) in order to facilitate its intragastric placement (Fig. 2a). Once the balloon was inflated and its intragastric position was confirmed laparoscopically, U-stitches were carefully tied over the pledgets while avoiding excessive force that could result in skin ulceration (Fig. 2b). The gastric–abdominal wall attachment was visualized and tested laparoscopically by pulling down on the stomach (Fig. 2c). At the end, the GT's position was verified by injecting 30–40 mL of normal saline and aspirating it via the nasogastric tube. It is very important to push back all the gastric wall edges around the tube inside the abdomen before tying the U-stitches in order to prevent persistent stoma-like gastrostomy or gastric mucosa prolapse (Fig. 2d). After 24 hours, the tube was used with escalating feeds until the full feed volume was reached by the second postoperative day. Stitches are usually removed after 10 days unless there are concerns about the patient's healing ability.
Results
Between March 2008 and January 2015, 64 cases of LAG were attempted in our institute. Of these, LAG using GTU was attempted in 31 consecutive cases, but 2 were excluded: 1 case for technical difficulties related to the fundoplication, and the other patient had multiple previous abdominal surgeries. The remaining 29 cases comprised 14 girls and 15 boys with a median age of 37 (range, 0.3–154.9) months. LAG-Fundo was performed for associated gastroesophageal reflux in 20 cases, whereas LAG-only was performed in the remaining 9 cases. The mean operative times for LAG-only and LAG-Fundo were 41 ± 12.4 minutes and 148 ± 57.5 minutes, respectively (Table 1).
Operative and Demographic Data
LAG, laparoscopic gastrostomy tube insertion; LAG-Fundo, laparoscopic gastrostomy tube insertion with fundoplication.
The main indications for the procedure were a spectrum of pathologies resulting in central neurological deficits that interfered with the patients' ability to swallow properly. A GT was placed in 3 patients who had failed to thrive: 1 patient was a case of trisomy 21, and the other 2 patients had previously undergone repair of a diaphragmatic hernia and tracheoesophageal fistula.
During a median follow-up of 21 (range, 4–81) months, no procedure-related mortality was reported in the group (Table 2). A major postoperative complication occurred in 1 patient who had a GT placed for failure to thrive after diaphragmatic hernia repair. In this case the U-stitches were removed after only 5 days, resulting in instant gastropexy dehiscence evident by the prolapsing omentum through the gastrostomy wound. He underwent immediate laparoscopy, and a GT was replaced successfully using GTU.
Complications
GT, gastrostomy tube; LAG, laparoscopic gastrostomy tube insertion.
Granuloma formation was the most frequent complication and was encountered in 6 cases, all of whom had been treated with silver nitrate application once or twice. In 5 of the 6 cases, granulomas disappeared completely in 1–2 months; 1 patient was lost to follow-up. Three patients had external leak around the GT that improved with proper care (Table 2). Caregivers were instructed to wrap small gauze around the GT head in a way to keep it elevated. This resulted in a better seal between the intragastric balloon and the abdominal wall, which subsequently stopped the external leak. No gastrostomy revision was required in any of the patients for managing persistent leak, granulation tissue, or prolapsing mucosa. The gastrostomy wound healed spontaneously in the 2 patients who had their GT permanently removed during the follow-up period.
Wound infection and skin ulceration occurred in 1 patient who had excessive tension at the site of pledget-reinforced U-stitches. The infection subsided, and the ulcers healed once the pledgets were removed and a course of oral antibiotics was provided.
Discussion
Achieving a safe and secure gastropexy has always been one of the most critical steps in minimally invasive GT insertion techniques. An unsecured gastropexy can lead to catastrophic postoperative events such as intraabdominal leak of gastric contents and total gastrostomy disruption. On the other hand, an overzealous attempt to achieve secure gastropexy by creating a stoma-like gastrostomy may interfere with healing and can result in persistent leak, wound infection, and repeated dislodgment.
Gastropexy during PEG is achieved using a polymeric silicone (Silastic®; Dow Corning, Midland, MI) intragastric flange. Although the procedure is simple and effective, significant wound complications have been described in patients with buried bumper syndrome leading to feeding difficulties, pain, and leak in 2.4%–22% of the cases.4,11,12 The majority of these patients require surgical removal. 13 Moreover, major abdominal sepsis, peritonitis, and colocutaneous fistula have been reported in 2%–7%2,4 of PEG cases.
LAG has been shown to offer a safer alternative to PEG with fewer postoperative complications.6,7,9,10 Although most of the steps are straightforward, gastropexy is the most challenging part of the procedure. The widely described MOT involves dilating the laparoscopic port in order to adequately exteriorize the gastric wall and expose the fascia adequately to place the gastropexy and purse-string stitches.6,8–10 Fixing the gastric wall and the mucosa closer to the skin is likely to cause mucosal overgrowth around the wound edges, possibly leading to stoma-like gastrostomy due to the gastric mucosa prolapse, which may interfere with the natural tendency of the gastrostomy wound to heal or close. Although MOT seems to offer a more secure gastropexy as evident by the low incidence (0%–1.3%) of reported gastric dehiscence,7,14 we suggest that the higher risk of stomatization in MOT may be responsible for a variety of reported GT-related problems in these patients, including excessive granulation tissue formation in 42%–44%,7,14 stoma infection in 24.7%, 14 persistent external leakage in 24%–26%,7,14 catheter dislodgment in 4%–21%,7,14 and nonhealing gastrocutaneous fistula in 4% 6 of the cases. Although most of these are minor complications, they can add a significant burden on the caregiver and are likely to increase utilization of healthcare resources. 15
Recognizing these challenges, various specialized percutaneous gastropexy tools have been developed with an aim to avoid port wound dilatation and stomatization during the LAG procedure. 16 The widely described Seldinger technique involves inserting the GT through a peel-away dilator passed over a guide wire. Special T-anchoring stitches or simple large U-stitches are placed transabdominally to fix the anterior gastric wall to the abdomen. However, unintentional posterior gastric wall injuries due to guide wire insertion have been reported in 3.7% of the earlier series. 16 Furthermore, the special tools used in the procedure are often not readily available and add unnecessary costs to the procedure. 17
We described a safe and efficacious LAG technique using GTU to achieve a secure and minimally invasive gastropexy. As is the case with most of the new techniques, we encountered some challenges during the initial learning curve. Although granuloma formation and paratube leak occurred in a few patients, we noticed that most granulomas tend to improve spontaneously. Based on our experience, we suggest that burying the gastric mucosa back inside the abdomen, once the GT has been inserted during the LAG procedure, is a very crucial step to reduce the incidences of granuloma formation and mucosa prolapse. Moreover, wrapping the dressing under the GT not only helps in minimizing the leak, but also possibly prevents granuloma formation by reducing the friction between the GT and the edges of the wound.
Footnotes
Acknowledgment
We extend our appreciation to the deanship of scientific research at King Saud University for funding this work as part of the Undergraduate Students Research Support Program (URSP).
Disclosure Statement
No competing financial interests exist.