
Abstract
Abstract
Purpose:
Thyroglossal duct cysts (TGDCs) may cause cosmetic defects or more serious impairments if left untreated. Our study was designed to examine the potential advantage of endoscopic surgery performed on TGDCs, especially the ability to completely resect the branches and to affect the cosmetic appearance.
Patients and Methods:
Thirty-two patients from Beijing Tongren Hospital, Beijing, China, diagnosed with TGDCs were selected. Seventeen patients with TGDCs underwent traditional Sistrunk's surgery, and 15 patients underwent endoscopic cystectomy.
Results:
All patients had complete resection and were followed up from 6 months to 4 years. None had a recurrence after endoscopic resection. However, patients in the traditional surgery group had a 5.9% (1/17) rate of recurrence. The incision length was approximately 2.1 cm in the endoscopic group compared with 5.2 cm in the traditional group. The mean time for the endoscopic operation was 97.7 minutes compared with 51.6 minutes in the traditional surgical procedure. The average length of hospital stay was 6.7 days in the endoscopic group compared with 9.7 days in the traditional group.
Conclusions:
Endoscope-assisted small-incision thyroglossal duct cystectomy is an efficient method. It causes fewer cosmetic defects and also decreases operative time. It will likely become the new standard procedure for patients with TGDCs.
Introduction
T
The surgical procedure, known as Sistrunk's procedure, involves making a transverse incision in the most elevated region of the cyst and removing both the middle portion of the hyoid bone itself and the surrounding tissues between the hyoid bone and the foramen cecum.5,6 This traditional surgical procedure, developed in 1920, reduces recurrence rates to 3%–5%. 7 However, it is also associated with certain problems. First, the procedure results in a 5-cm scar in the anterior of the neck. Second, removal of the tissue surrounding the hyoid bone and the foramen cecum, including muscles at the base of the tongue, during Sistrunk's procedure is associated with high levels of trauma. 8 Third, the tract is usually tiny and fragile; therefore, it is easily broken off and difficult to remove. In fact, in some patients, because the tracts between the hyoid bone and the foramen cecum are closed, muscles operated from the floor of the oral cavity, which still should be retained, are difficult to distinguish with the naked eye. 9 Fortunately, with the assistance of an endoscope, we are able to clearly identify if a branch is linked to the foramen cecum and to show a good appearance of the neck following the operation. Some studies showed excision of TGDCs with endoscope assistance by performing an incision at the cyst bump, but a transverse scar is left in the neck.
In order to improve the outcome of surgery, being less invasive and maintaining good neck shape and structure, the present study aimed to use endoscopic cervical dermatoglyphic incision in the complete resection of TGDCs.
Patients and Methods
Study patients
In total, 32 patients with preoperative diagnoses of TGDCs were identified in the medical records after the patients provided informed consent and the local ethics committee approved the study. The patients were randomized into two groups. One group consisted of 17 patients who were treated by the traditional Sistrunk's procedure. The second group consisted of 15 patients who underwent endoscopic surgery. Clinical charts, radiographic images and reports, and operative procedures were examined. Information was gathered and compiled into a central database. Collected data included age at presentation, sex, severity of symptoms, size and location of TGDCs, surgical approach, number and nature of further interventions, years of documented follow-up, patient condition at last visit, recurrence rate, and surgical complications.
Preoperative evaluation
The preoperative evaluation included the following:
1. Ultrasonography. If any solid element within the cyst was found, fine-needle aspiration cytology was needed in the differential diagnosis. 2. More than 3 years old 3. Excluded acute infection. Antibiotic treatment was used to eliminate the infectious symptoms before surgery. 4. Other preoperative examinations, including thyroid function tests to exclude other conditions, such as ectopic thyroid gland, lymphadenitis, and branchial cleft cyst.
Surgical instruments and equipment
The endoscope and monitoring devices used were produced by Karl Storz (Tuttlingen, Germany): the 0° endoscopic products (diameter, 4.0 mm), video surveillance systems, and the monopolar needle-knife. The ultrasonic scalpel (model ACE 23P) was from Ethicon, a Johnson & Johnson Company (Somerville, NJ). Foley catheters (10 French) and general surgical devices were also used.
Endoscopic surgical procedure
Patients in the traditional group were operated on according to the classic Sistrunk's procedure in the literature.3,5 Patients in the endoscopic group were operated on according to the procedure as follows. Each surgery was completed by the same surgeon.
Anesthesia
The procedure was typically performed with the patient under general anesthesia with endotracheal intubation. All patients were placed in the supine position with the neck slightly extended. The surgeon stood on the right side of the patient, and the endoscopic monitor was placed on the head side of the patient.
Incision design
According to the striated distribution in the neck around the hyoid bone, a dermatoglyphic incision was made about 2.0 cm across the anterior of the neck (Fig. 1).
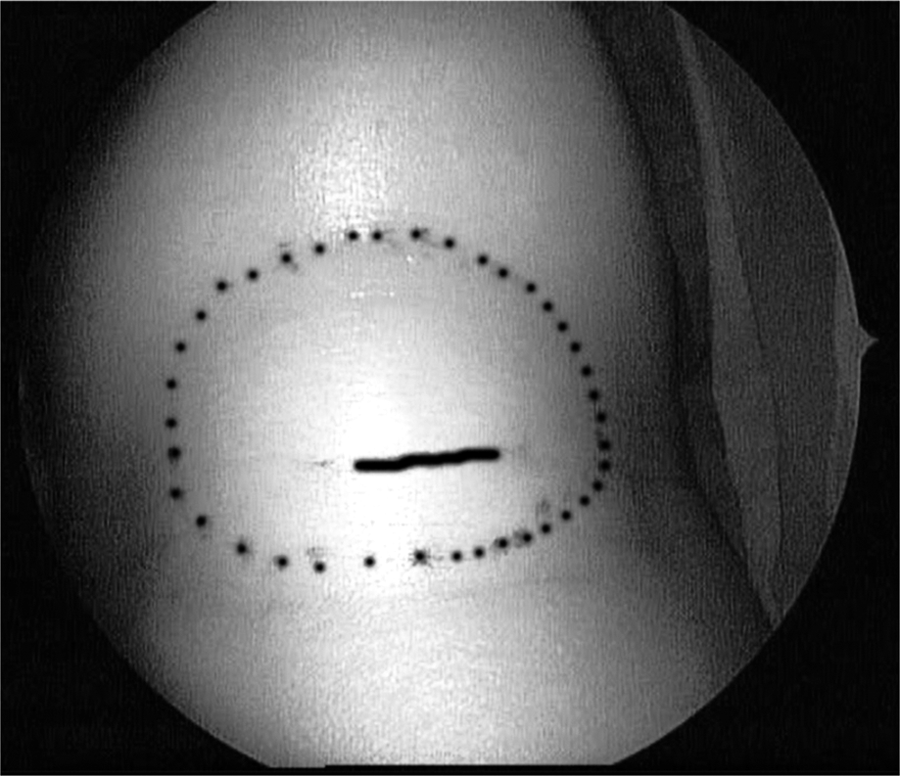
Incision design. The dotted line represents the outline of the thyroglossal duct cyst. The continuous line, located in the skin wrinkle, is about 2 cm long and represents the endoscopic incision.
Surgery workspace by water balloon inflation
The incision was made, and the skin flaps were dissected under the platysma. A Foley catheter was placed under the platysma muscle (Fig. 2). Sterile water (15–20 mL) was infused in order to continuously enlarge the subcutaneous lacunar. Then, after 5 minutes water was drained out under endoscopic visualization. Skin was made to hang using a Kirschner wire in order to fully expose the space from the superior border of the hyoid bone to the supreme region of the thyroid cartilage.
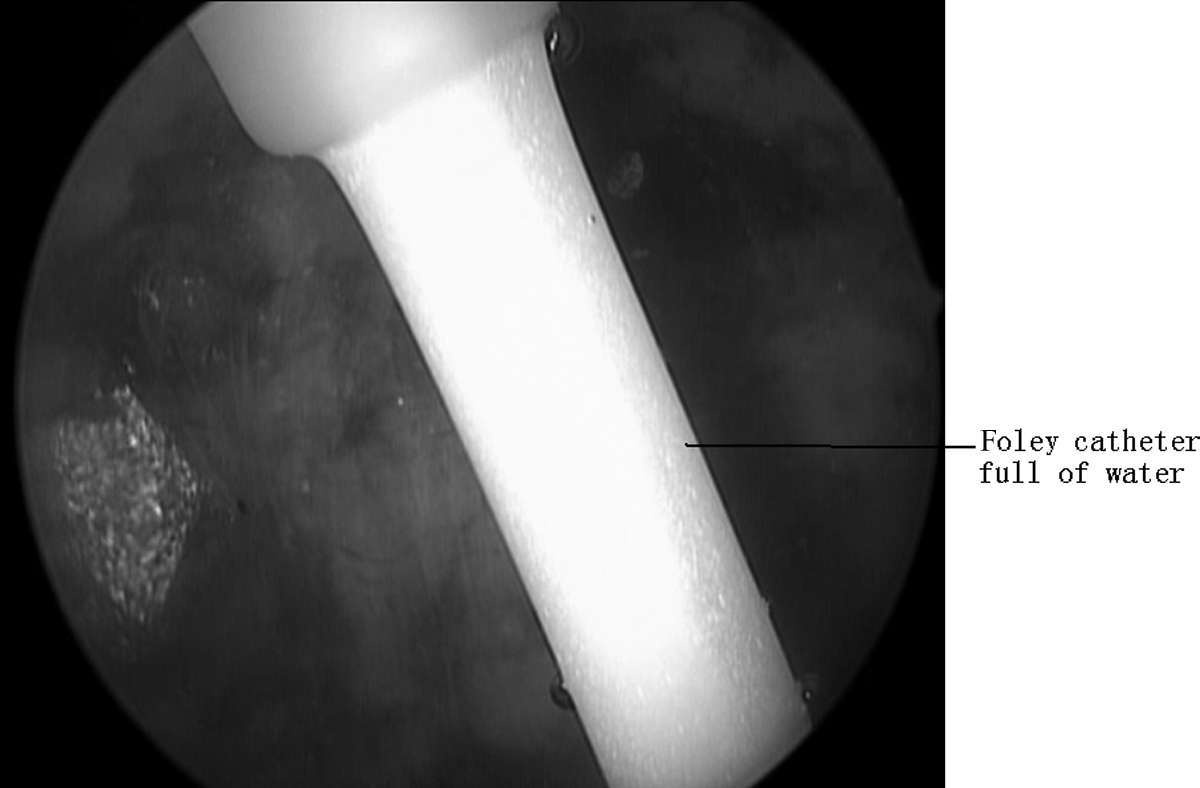
Surgery workspace created by water balloon inflation. A Foley catheter was placed under the platysma muscle.
Exposure of cysts
The white line of the neck was carefully distinguished, and both sides of the strap muscle were separated with monopolar electrocautery. The strap muscle was then cut off under the hyoid bone with an ultrasonic scalpel, fully exposing the anterior wall, side wall, and lower wall of the cyst. If the cyst was too large, fluid could be partially extracted in order to separate the cyst from surrounding tissue. The bottom edge of the cyst was lifted and isolated from this bottom region, continuing up to the back side of the hyoid bone.
Excision of hyoid bone
The genioglossus was broken away at the upper edge of the hyoid bone. The body of the hyoid bone was cut off from the inside, and the hyoid bone and cyst were turned over to expose the back of the hyoid bone. Carefully, we checked the upper side of the cyst with endoscopic assistance to identify branches reaching the foramen cecum. If the cyst went across the hyoid bone, we kept track to the foramen cecum and ligated it. We carefully checked and refilled the surgery space after cyst resection to make sure there was no residual fistula. Sistrunk's procedure removed the midportion of the hyoid bone in continuity with the cyst along with excision of a block of tissue between the hyoid bone and the foramen cecum.
Closure of the cavity
We flushed the surgical field and made sure that the cavity had completely stopped bleeding. We performed suction drainage and intradermic suture. A digital photograph of the incision was taken at 4 weeks postoperatively in both the endoscopic group and the traditional surgery group.
Follow-up
The length of follow-up for the TGDC patients ranged from 6 months to 4 years, with the mean time being 11 months in the endoscopic group compared with 12 months in the traditional surgery group.
Statistical analysis
Data were reported as mean ± standard deviation values or as medians (range). Statistical significance of the differences between the two surgical groups was determined by Student's t test. All statistical analysis was two-sided. Values of P < .05 were considered significant.
Results
In the endoscopic group, there were 6 males and 9 females, ranging in age from 4 to 47 years, with a mean age of 24 years. In the group undergoing traditional surgery, there were 7 males and 10 females, ranging in age from 6 to 51 years, with a mean age of 27 years. Prior to endoscopic surgery, cysts ranged in size from 1.5 to 4.5 cm, with the average size being 2.1 cm. Prior to traditional surgery, cysts ranged in size from 1.2 to 4.8 cm, with the average size being 2.4 cm (Table 1).
Data are mean ± standard deviation values unless indicated otherwise.
Clinical manifestation
All clinical parameters are summarized in Table 1. The average incision length made during endoscopic surgery was approximately 2.1 cm. In patients undergoing traditional surgery, the average incision size was 5.2 cm. The mean time of the endoscopic operation was 97.7 minutes compared with 51.6 minutes in the traditional surgical procedure. Decreasing trends of operative time are shown in Figure 3. Only 5.4 mL of blood was lost by the patients in the endoscopic group; this is in stark contrast to the 45.3 mL of blood lost during traditional surgery. No complications, such as infection or pharyngeal fistula, occurred following endoscopic surgery. However, there was a single case having both pharyngeal fistula and infection in the traditional Sistrunk's surgery group. The average length of hospital stay was 6.7 days in the endoscopic group compared with 9.7 days in the traditional group.
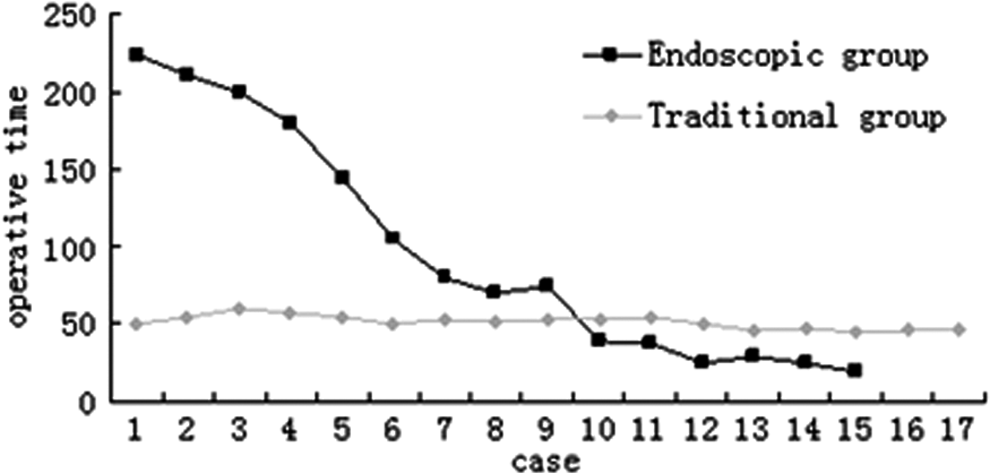
The trends curve of operative time (in minutes). Two distinct phasåes appeared, at Case 7 and Case 10.
Follow-up
All patients had complete resection of their cysts. Postoperative pathologic examination confirmed that all were TGDCs. The appearance of the incision in the endoscopic surgery group had a much better cosmetic effect than in the traditional Sistrunk's surgery group after 4 weeks postoperatively (Figs. 4 and 5). The sole patient complaint at the initial follow-up was mild odynophagia and dysphagia that resolved quickly without sequelae. None of the cases had experienced recurrent symptoms after endoscopic resection. However, there was one recurrence in the traditional surgery group (5.9%).

Appearance of the incision 4 weeks postoperatively after endoscopic surgery

Appearance of the incision 4 weeks postoperatively after traditional Sistrunk's surgery.
Discussion
In 1893, Schlange summarized the surgical treatment of cysts of the tongue; he proposed that because the hyoid bone is located in a central region, it should be resected when dealing with cysts of the tongue, as recorded by Mondin et al. 2 In 1920, Sistrunk 3 expanded on the surgical effect of TGDCs and proposed a basic process for excision of TGDCs. The classical Sistrunk's procedure involves making a transverse incision in the most elevated region of the cyst and removing the midportion of the hyoid bone in continuity with the TGDCs. This is typically done in conjunction with excision of a block of tissue between the hyoid bone and the foramen cecum.
However, this classical procedure is not without its shortcomings. A 5-cm transverse cervical scar in the midline of the neck is sometimes prominent and may even result in discomfort when swallowing. The branch is usually small and frail, and so it can be easily broken off and difficult to remove. This can lead to a high rate of recurrence. Additionally, the removal of the surrounding tissues between the hyoid bone and the foramen cecum, including the muscle associated with the base of the tongue, leads to significant trauma. 8 The purpose of the present study was to use endoscopic cervical dermatoglyphic incision, to completely resect cysts, to minimize cosmetic defects, and to maximize the amount of normal tissue to be retained.
Sistrunk's procedure involved complete removal of TGDCs and its possible branches. It also involved removal of the midportion of the hyoid bone and midline tissues extending from the hyoid bone toward the foramen cecum, including the genioglossus and the mylohyoid muscle. 5 The branches of the posterior of the hyoid bone were very thin and fragile. Thus, they could easily be broken off. In order to avoid omissions, Sistrunk drew a vertical line and a horizontal line in the upper edge of the midportion of the hyoid bone; he defined the point of intersection as the foramen cecum, which serves as the landmark of TGDCs resection. 3 Some researchers had proposed preoperative injection of methylene blue as a color marker to trace the distribution of branches, but not all small branches become colored.10,11 Notably, it was difficult to work in a limited surgical field when viewing with the naked eye. Endoscopic magnification (four- to sixfold) allowed clear identification of a branch that was linked to the foramen cecum. 12 Endoscopic operation clearly showed this type of branch and improved the opportunity for surgical resection. Minimally invasive surgery and clear surgical field were distinct advantages.
One of the other major advantages of using the endoscope was a good cosmetic appearance of the neck following the operation. Because the depth of the surgery field could be assessed and adjusted with the endoscope, the incision design was less complex. 13 Hu and Wang 14 resected cysts under the arm and breast areola, injecting carbon dioxide to maintain the surgical space. Zhang et al. 15 performed endoscopic excision of TGDCs by no-gas injection technology, along the arc incision above the sternal notch. These approaches had minimal cosmetic defects due to miniscule incisions, but a main disadvantage was that these incisions were made at a long distance from the cyst. These approaches were also associated with lengthy operative times and large tissue trauma. Using carbon dioxide gas injection to maintain space increased complications, such as hypercapnia, respiratory acidosis, subcutaneous emphysema, and air embolism, as well as increased operation costs.16,17
In contrast to these surgeries, our study design involved a dermatoglyphic incision in the neck and a shorter surgical procedure. Usually, the cervical striate of the submental area were lower, located below 1–2 cm of the most elevated cyst. This kind of incision was difficult to expose the superior pole of the cyst, especially to excise the hyoid bone and the tract behind the hyoid bone. However, with the endoscope, we could clearly identify the cyst and branches. Compared with other endoscopic surgeries, our surgical approach was associated with significantly shorter surgery and reduced injury.
In addition to a smaller incision length and a less noticeable scar, the use of the endoscope also helped reduce the bleeding and shorten the hospital stay.18,19 Because of a clear surgical field, the use of the endoscope can also preserve the muscle and reduce unnecessary trauma. Of the 15 cases in the endoscopic surgery group, none showed complications, and very few had significant blood loss during surgery.
The major disadvantage of endoscopic resection was that the procedure was more time consuming compared with the conventional opening method. 20 As can be seen in Figure 2, there were two distinct phases on the trend curve of operative time. It is important that the operative time of the last 4 cases was less than that for the traditional operation. With technical improvements in the first phase, the duration of the operation decreased considerably after the seventh case. Beginning from the 10th case, we began to focus on ultrasound surgery. This technique helped to stop bleeding more efficiently and thus decreased operative time. Additionally, we adopted water balloon inflations in the process of workspace creation, along with separating the cyst and surrounding soft tissues. In the subsequent cases, the operative time was shorter than that recorded for conventional surgery. With a more advanced endoscopic instrument and increased surgical experience, we believe that the operative time will decrease even further in the future.
The Sistrunk operation 3 from 1920 was able to reduce the recurrence rate to 3%–5%. In our study, the traditional surgery group had a 5.9% recurrence rate. Although 1 patient had a recurrence with the Sistrunk's procedure, stratified analysis showed limited numbers of individuals in each subgroup. Larger numbers of cases from different surgical centers are required to validate these findings. However, long-term follow-up is needed to confirm the results of our new surgical approach. Nevertheless, our approach was made technically feasible by advancements in surgical instruments and technology.
In summary, this study is the first to introduce water balloon inflations to create a working space, along with separating the cyst and surrounding tissues. This method is simple and practical, greatly reduces cyst separation time, and consequently shortens the surgical process. With the development of equipment and shortened operative time, endoscope-assisted small incision surgery will become a new option for patients with TGDCs.
Conclusions
Endoscopic thyroglossal duct cystectomy is an efficient, feasible, and safe method, which improves cosmetic appearance and is associated with less operative time. It promises to be a good option for patients with TGDCs.
Footnotes
Disclosure Statement
No competing financial interests exist.