
Abstract
Abstract
Introduction:
Fibroadenoma is a common condition in adolescent girls. Most tumors are excised either through a periareolar approach or the inframammary approach. Both approaches produce visible scars in adolescent girls. We propose a new cosmetic approach to this lesion and report our experience with the transaxillary subcutaneouscopic approach for excision of the fibroadenoma of the breast. The purpose of this case report is to delineate an innovative surgical approach to resection of a breast fibroadenoma that yields an adequate resection without possible damage to the ductal system while optimizing cosmetic results by avoiding scars.
Materials and Methods:
We retrospectively reviewed the medical records of four adolescent girls who underwent the above approach for excision of fibroadenoma of the breast. The age range was 14–16 years.
Results:
There were no complications in all 4 patients. The final result at the 3-month follow-up revealed an esthetically pleasing skin incision that healed well and was hidden by the natural skin fold of the axilla.
Conclusions:
Transaxillary subcutaneouscopic excision of fibroadenoma of the breast in children is a safe and effective technique and should be considered for excision of benign breast lesions in children.
Introduction
T
The purpose of this case report is to describe a new surgical approach to resection of a breast fibroadenoma via the subcutaneouscopic approach, which yields an adequate resection while staying away from the ductal system and optimizing cosmetic results by avoiding scars.
Materials and Methods
We retrospectively reviewed the medical records of four adolescent girls who underwent the above approach for excision of fibroadenoma of the breast. The age range was 14–16 years. In all the patients the mass had been present for more than several months and was slowly enlarging in size. The patients denied any change in the mass with their menstrual cycles. On physical examination, the mass was nontender, palpable, firm, and mobile and located away from the nipple and areola. Ultrasound was suggestive of fibroadenoma in all 4 cases. Detailed counseling regarding all options was offered to all patients and their parents. This approach was only offered to parents and children who elected to undergo resection of the fibroadenoma using this approach.
Operative technique
The patient underwent general endotracheal anesthesia. She was then positioned supine on the operating room table with the left arm fully abducted. A small (5-mm) incision was made in the natural skin fold just behind the anterior axillary line. Using a Kittner dissector and a Foley balloon catheter, a space was carefully created subcutaneously. Once an adequate space was created, a second incision (3 mm) in the same line as the previous was made (Fig. 1). Following this, two ports (a 5-mm and a 3-mm step port) were placed through the incisions. Sometimes an additional 3-mm port may be needed to help with the dissection. The skin was then sutured closed around the ports to allow for a tight seal. The dissected space was then insufflated using 8–10 mm Hg of CO2 gas, which facilitated creation of a subcutaneous working space. The mass was circumferentially dissected free carefully using hook electrocautery (Fig. 2). The specimen was then removed through the 5-mm incision, extending it by a few millimeters if needed, and was submitted to pathology for review. The wound was irrigated with normal saline until the effluent was clear. The wound was then closed with a subcuticular 5-0 polyglactin 910 (Vicryl™; Ethicon, Somerville, NJ) suture and reinforced with liquid skin adhesive. The patient tolerated the procedure well.
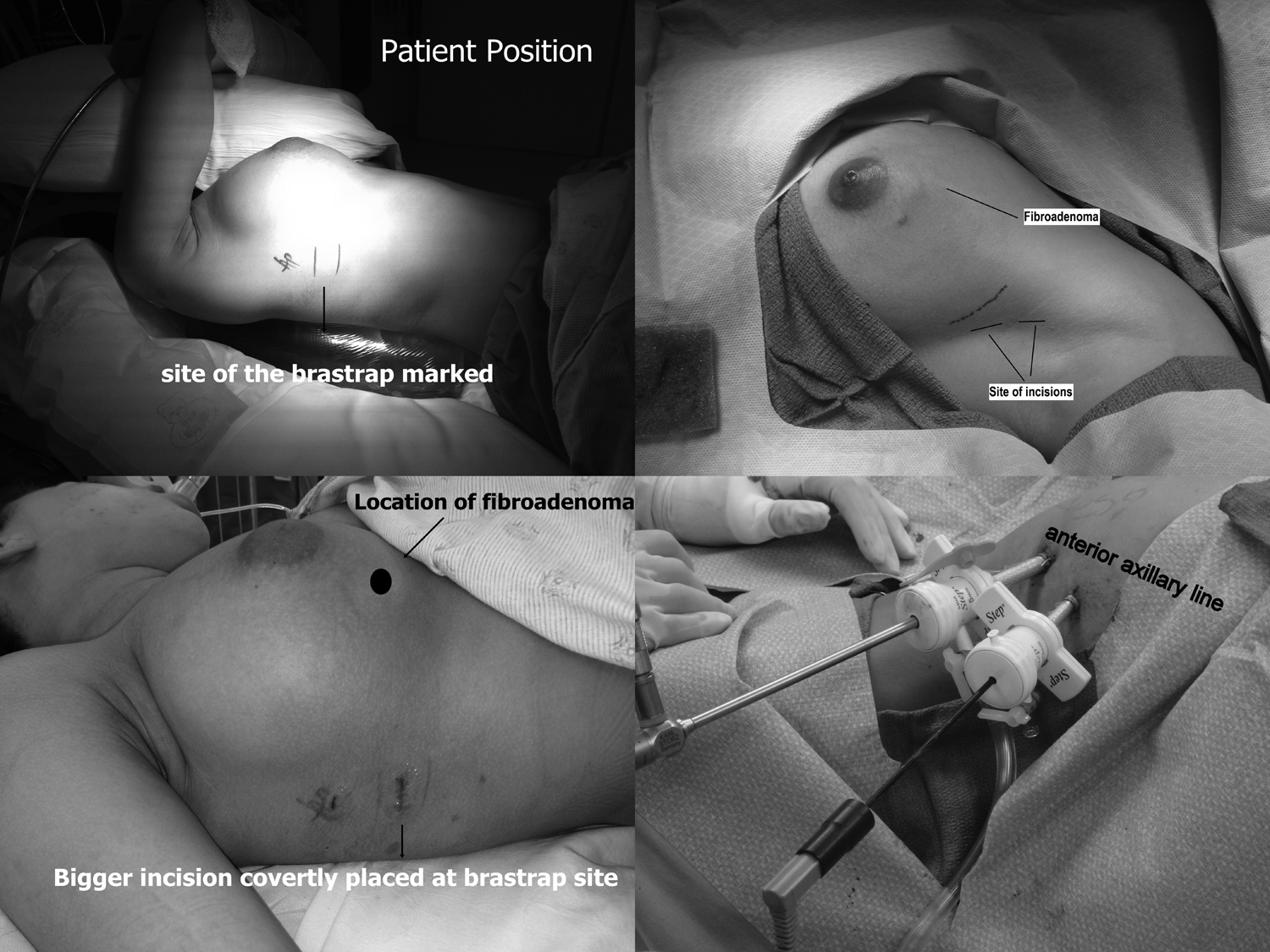
Location of the fibroadenoma, patient positioning, and placement of incisions and ports.
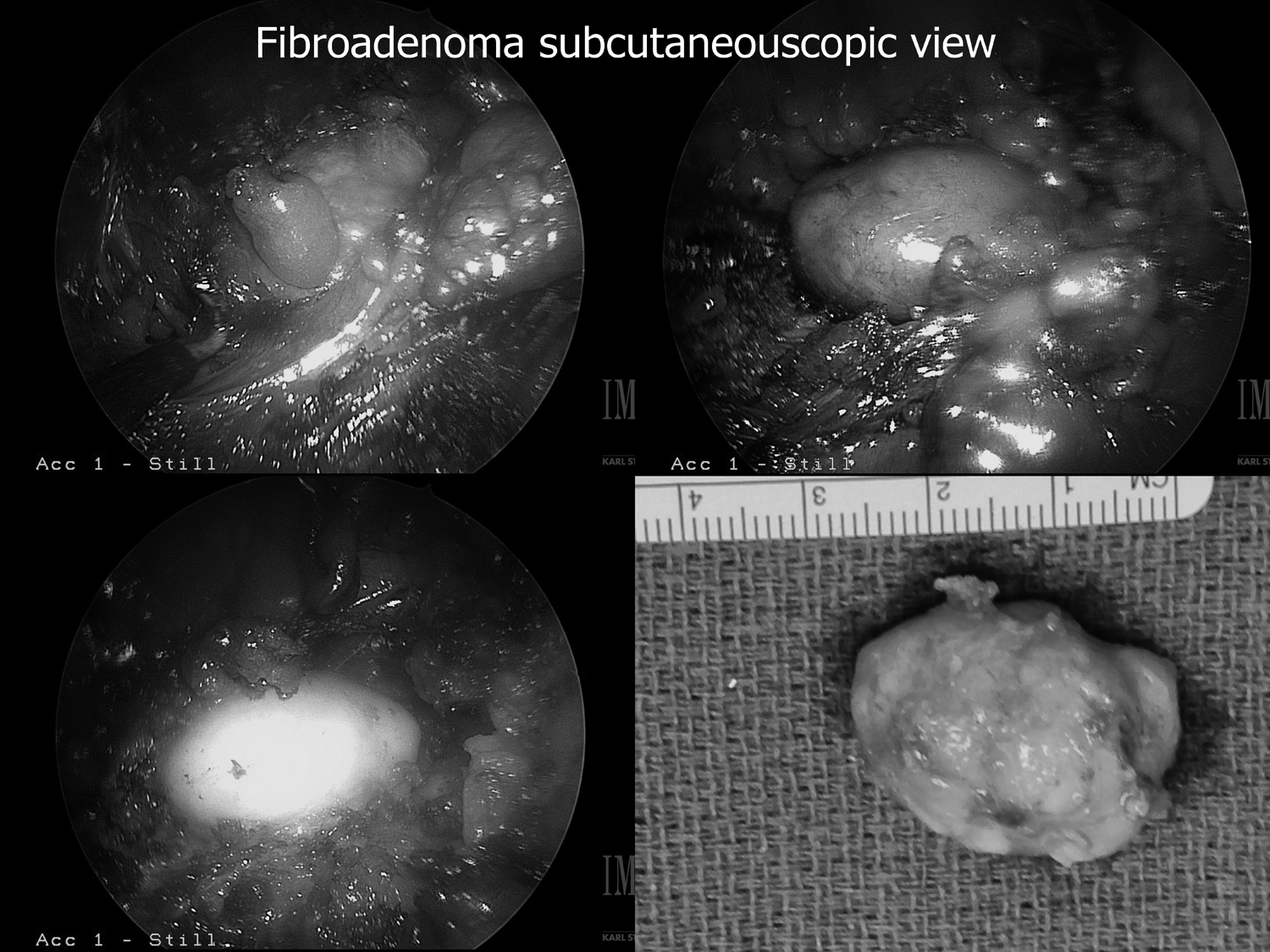
Subcutaneous views of the fibroadenoma and the retrieved specimen.
Results
There were no complications. The final result at the 3-month follow-up visit revealed an esthetically pleasing skin incision that healed well and was hidden by the natural skin fold of the axilla (Fig. 3). All patients also reported satisfaction with the final appearance at follow-up.

Excellent cosmetic results: no scar is seen on the breast at 3-month follow-up.
Discussion
Few authors have described use of a transaxillary approach to excision of a benign breast mass. The allure of using a transaxillary approach compared with the traditional approach, with an incision overlying the breast, is largely due to the desire of avoiding a large unsightly scar directly on the breast. Plastic surgeons have been using the transaxillary approach to the breast for over 30 years to perform breast augmentation. 1 Therefore it is a natural step for other surgeons to adopt a new technique that allows for a more esthetically pleasing scar. The technique of removing a breast mass via a transaxillary incision is surgically possible due to the axilla lying in a contiguous space with the breast tissue, thus allowing for relatively easy access.
Few authors have described an approach to removal of a breast mass via nontraditional methods. Khan et al. 2 described transaxillary excision of a breast fibroadenoma using a single incision. They performed a transaxillary dissection where the surgeon traversed through the deep subcutaneous plane and then into the breast tissue, where he created a tunnel until the tumor was reached. Next, a traction suture was placed through the mass to allow manipulation for dissection and removal. The subset of patients they reviewed was noted to be largely between 20 and 24 years of age, and the involved lesion was noted to be in the upper outer and lower outer quadrants of the breast.
Kitamura et al.3–5 also described extramammary resection of benign fibroadenomas in a series of patients. They performed this procedures using a subcutaneouscopic technique via three widely spaced incisions in the midaxillary line. They used a preperitoneal distension balloon to create a working space, and with the help of an endoscope they performed resection of the mass. Their patients were between 10 and 50 years of age, with a mean age of 27.6 years.
The average age of patients described as having undergone excision of breast fibroadenoma via a nontraditional method is mid-20s.
Subcutaneouscopic transaxillary excision of a breast fibroadenoma using 3-mm laparoscopy instruments in pediatric patients has not been described.
As with all new advances/procedures there are advantages and disadvantages to using the subcutaneouscopic technique. Advantages to performing a transaxillary excision of a fibroadenoma include the lack of scar on the breast with an esthetically pleasing incision hidden in a covert location (in a natural skin fold). This is especially important for patients who are prone to hypertrophic scar/keloid formation, as it would avoid such a lesion on the breast. Furthermore, location of the incision on the breast has also been identified in previous studies to play a role in the perceived sensitivity of the nipple–areolar complex. Esthetic breast surgeons have performed various studies investigating the location of the incision on the breast and sensation of the nipple–areolar complex.
In a study by Araco et al., 6 patients underwent breast augmentation via periareolar versus submammary incision. After performing a retrospective study of their patients, they noted the only factor associated with nipple–areola complex sensitivity alterations and areolar pain at 6 months was the type of skin incision used for the procedure. Patients who had undergone periareolar incisions were more likely to complain of alterations in nipple sensation. The periareolar incision increased the risk of nipple–areola complex sensitivity almost threefold and the risk of areolar pain by more than threefold.
Another concern that can be avoided by refraining from making an incision on the breast is possible damage to breast buds, areola, and the ductal system. Injury to the breast bud or its vascular supply prior to or during breast development can impair breast growth, resulting in breast hypoplasia. 7 Making a transaxillary incision and refraining from direct breast incision injury to the breast bud or vascular supply can be avoided. The latter is important for the psychological health of a pediatric patient. Significant asymmetry of the breast in an adolescent could negatively affect the confidence and self-esteem of a patient at this delicate age. Furthermore, via a transaxillary incision there is the possibility of performing resection of multiple masses via a few limited incisions.
Disadvantages of this technique are the lack of surgeon experience with the subcutaneouscopic approach, which could lead to longer operative times. Furthermore, because CO2 gas is used for the procedure, the patient must undergo general anesthesia. The use of this new technique in a children's hospital does not impact anesthetic choice as almost all of our patients undergo general anesthesia. Another concern is that the need for CO2 insufflation can lead to subcutaneous emphysema. This was not a problem in any of our cases.
Transaxillary subcutaneouscopic excision of fibroadenoma of the breast using 3-mm laparoscopy instruments in children is a safe and effective technique and should be considered for excision of benign breast lesions in children. One disadvantage is that this involves learning a new technique, when the majority of surgeons are already comfortable with the open approach. However, it should be noted that basic laparoscopic skills translate well to this technique, and competence can easily be achieved after only a few cases.
Footnotes
Disclosure Statement
No competing financial interests exist.