
Abstract
Abstract
Objectives:
The effect of hysterectomy on vesicourethral and sexual functions remains controversial. The primary objective of this study was to compare the effects of a laparoscopic hysterectomy and a total abdominal hysterectomy on lower urinary tract function. The secondary aims were to compare the two surgeries in terms of postoperative vaginal length and dyspareunia.
Materials and Methods:
This was a prospective randomized clinical study in which 292 women were assigned to either the laparoscopic hysterectomy (n = 146) or total abdominal hysterectomy (n = 146) groups. The vaginal length and urodynamic measurements were taken, and the patients were asked to grade the presence and severity of dyspareunia using a visual analog scale 3 weeks before and 12 weeks after the surgery. The relationship between the postoperative vaginal length and the incidence of dyspareunia was evaluated. The urodynamic procedures used included uroflowmetry and voiding cystometry to record the maximum flow rate (Q-max) and to assess the bladder capacity.
Results:
The preoperative vaginal length was similar between the groups, whereas the postoperative vaginal length was significantly longer in the laparoscopic hysterectomy group. When the 15 patients who developed postoperative dyspareunia were evaluated, no differences in the postoperative vaginal length were seen, but a significant difference in the change in the length of the vagina was found when compared with the other patients. No significant difference was found with regard to pre- and postoperative Q-max, bladder capacity, and change in bladder capacity between the study groups.
Conclusions:
The change in the length of the vagina was much more remarkable after total abdominal hysterectomy, compared with laparoscopic hysterectomy. It seems that the Q-max and the bladder capacity increase after hysterectomies, regardless of the surgical type. Further prospective randomized comparative studies are warranted to ascertain whether laparoscopic hysterectomies cause less damage to the pelvic floor, compared with abdominal hysterectomies.
Introduction
T
The effect of a hysterectomy on vesicourethral function also remains controversial, and an earlier study has suggested that a simple hysterectomy increases the risk of vesicourethral dysfunction, due to neurological abnormalities caused during the operation.7,10 In numerous prospective studies, however, this association could not be established.11–13 It appears that prospective studies comparing pre- and postoperative urodynamic findings are necessary to evaluate the effects of a hysterectomy on vesicourethral function. 14 Several prospective studies have been presented in this area, and most of them showed improved results according to their urodynamic findings.11,15–17
The primary objective of this study was to compare the effects of laparoscopic hysterectomy (LH) and total abdominal hysterectomy (TAH) on lower urinary tract function. The second aim was to compare the two surgeries in terms of vaginal length and dyspareunia.
Materials and Methods
This prospective randomized clinical study was performed in the Obstetrics and Gynecology Department, Zeynep Kamil Women Health Training and Research Hospital, Istanbul, Turkey. The study was approved by the human ethics committee of the hospital (approval number 2014-135-136) and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The manuscript was prepared in accordance with the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines. 18
All of the patients who had urinary symptoms suspected to be due to a bulky, highly anteverted or myomatous uterus and for whom an LH or abdominal hysterectomy was planned for benign reasons were considered for recruitment, during the period from January 2014 until April 2015. The exclusion criteria included the unwillingness of the patients to participate in the study, sexual inactivity, having a partner with erectile dysfunction, the presence of psychiatric symptoms or diagnoses (psychosis, hallucinations, anhedonia, depression, body image dissatisfaction, or posttraumatic stress disorder), morbid obesity, and malignant pathology. After written and verbal informed consent, 292 women were assigned to either the LH (n = 146) or TAH (n = 146) group. Patients were randomized using computer-generated random allocations (randomization.com) in a ratio of 1:1 in balanced randomly permuted blocks.
The vaginal length and urodynamic measurements were performed, and the patients were asked to grade the presence and severity of dyspareunia using a visual analog scale, ranging from 0 (absence of pain) to 100 (the worst possible pain), 2 weeks before and 3 months after the surgery according to the validated questionnaire. 19 Mild pain was defined as a score of 1–50, moderate pain as 51–80, and severe pain as 81–100. The measurement of the vaginal length was performed using ring forceps, from the hymenal ring to the posterior fornix. Additionally, the relationship between the postoperative vaginal length and the incidence of dyspareunia was evaluated. As the patients were candidates for surgery also for the urinary symptoms, a sequential surgical management was determined, so after exclusion of the effect of the uterus on urinary functions by means of hysterectomy, subjects underwent pre- and postoperative urodynamic assessment. The urodynamic procedures included uroflowmetry and voiding cystometry to record the maximum flow rate (Q-max) and assess the bladder capacity. A six-channel sonar urodynamic monitor (model UD-200; Medical Measurement Systems BV, Enschede, The Netherlands) with computer analysis was used for this study. All of the procedures and the questionnaire on sexual function were performed by the same surgical team, including three surgeons, and the data were interpreted by a single observer.
An LH was performed as follows: a Foley catheter was inserted to empty the bladder, and a uterine manipulator with a cup fitting into the cervix (which is designed for the LH) was used to mobilize the uterus and to visualize the fornix. Three laparoscopic puncture sites, including the umbilicus, were used: 10-mm umbilical, 5-mm left lower quadrant, and 10-mm right lower quadrant. After the diagnostic evaluation, the round ligaments, Fallopian tubes, and infundibulopelvic ligaments or utero-ovarian ligaments (when the ovaries were to be conserved) were resected. The vesicouterine space was dissected using scissors, and the bladder was pushed downward using sharp and blunt dissection and hydrodissection. After the bladder was dissected from the anterior cervix and the uterine arteries were skeletonized using hydrodissection, the uterine arteries were sealed and divided on both sides. For this step, a LigaSure™ (Covidien, Mansfield, MA) vessel sealing device was used. The anterior and posterior colpotomies were performed on the rim of the cup with a unipolar hook, and the vaginal cuff was closed with two or three sutures.
A TAH was performed intrafascially, using the clamp-cut-ligate technique. The vagina also was clamped and cut just below the cervix, and the vaginal cuff was closed using a running suture.
The following baseline and clinical data were recorded: age, body mass index, parity status, mode of delivery, surgical approach (LH versus TAH), pre- and postoperative vaginal length, pre- and postoperative maximum flow rate, pre- and postoperative bladder capacity, and pre- and postoperative dyspareunia.
Statistical analyses were performed using SAS statistical software (version 9.1.3; SAS Institute, Cary, NC). Continuous variables were summarized using the means and standard deviations and were compared between the groups using the Student's t test and Mann–Whitney tests as appropriate. Categorical variables were summarized with total counts and percentages and were compared between the groups using the chi-squared test with Fisher's exact test, if necessary. The changes from the pre- to the postoperative status for the vaginal length, Q-max, and bladder capacity values were assessed using the Wilcoxon sign rank test, and the change from the pre- to postoperative status for dyspareunia was assessed using the McNemar test. A difference was considered to be statistically significant when P < .05.
Results
Some of the demographic and clinical data for the study population are summarized in Tables 1 and 2. The groups did not differ significantly with regard to the mode of delivery as shown in Table 1. Figure 1 shows the flow chart of the trial.
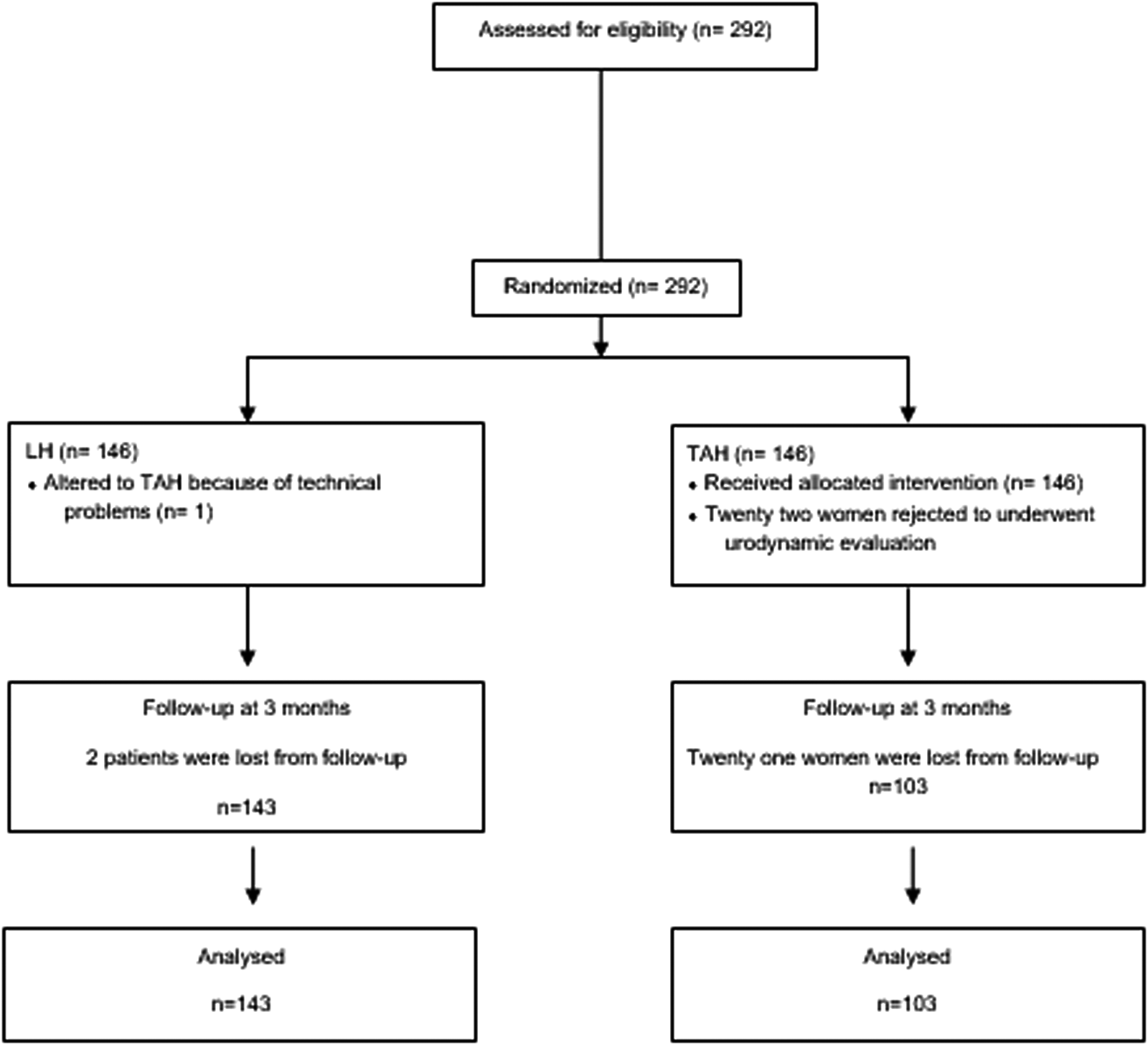
Flow of patients through the trial. LH, laparoscopic hysterectomy; TAH, total abdominal hysterectomy.
Data are mean ± standard deviation values or n (%) as indicated.
BMI, body mass index.
Data are mean ± standard deviation values, n (%), or n as indicated.
Significant difference.
Q-max, maximum flow rate.
The comparisons between the pre- and postoperative data for all participants are presented in Table 3. A significant difference was observed between the pre- and postoperative findings in terms of the vaginal length, Q-max, bladder capacity, and rates of dyspareunia. However, there was no significant difference between the study groups with regard to mean age, body mass index, parity, preoperative vaginal length, pre- and postoperative Q-max, pre- and postoperative bladder capacity, and change in bladder capacity. The postoperative vaginal length was significantly longer in the LH group (Table 4), and the women who underwent a TAH had a significantly greater decrease in the vaginal length than the women in the LH group.
Significant difference.
Q-max, maximum flow rate.
Data are mean ± standard deviation values.
Significant difference.
Two patients in the LH group (1.4%) and 1 patient in the TAH group (1%) reported moderate preoperative dyspareunia, and their complaints remained 3 months after the operation (Fig. 2). In total, 8 (5.6%) and 10 (9.7%) patients had dyspareunia 3 months after the operation in the LH and TAH groups, respectively. When the 15 patients who developed postoperative dyspareunia were evaluated, no difference in the postoperative vaginal length, but a significant difference in the change in the length of the vagina, was found, compared with the other patients, with the exception of 3 patients who had preoperative dyspareunia.
Patients with dyspareunia before and after
Discussion
It has been shown that the vaginal length and pelvic floor disorders are affected by parity, the mode of delivery, menopause, and hysterectomy.20,21 In our study, the mean age, body mass index, parity, and the mode of delivery were similar between groups, which can reduce the bias when comparing the two groups. Although the preoperative vaginal length did not differ between the groups, the TAH significantly shortened the vaginal length. Our results showed that a vaginal cuff length of 1.7 cm was taken out, together with the uterus, for the TAH, whereas a vaginal cuff of 0.4 cm was taken out for the LH. One explanation is that the use of the uterine manipulator with the cup may help in clearly identifying and distending the vaginal fornices to enable performing the colpotomy on the rim of the cup. Furthermore, a running suture was always used in the TAH, whereas only two or three sutures were used in the LH to close the vaginal cuff. If the vagina is incised as close to the cervix as possible in the TAH, the shortening of the vagina may be prevented.
In a prospective observational study comparing TAH with vaginal hysterectomy in terms of the vaginal length and incidence of dyspareunia, postoperative dyspareunia was found to be more common in the vaginal hysterectomy group, which was attributed to the postoperative shortening of the vagina. 6 However, no information about the mode of delivery was reported. From a study by Abramov et al., 22 we know that the prevalence of dyspareunia increases after pelvic reconstructive surgery, but this is not attributable to a postoperative decrease in the vaginal dimensions. Furthermore, most researchers found no differences in the sexual function after a hysterectomy, whether performed abdominally, laparoscopically, or vaginally.23–25 Some studies even showed an improvement in sexual function in the patients who underwent a hysterectomy.26–28 In fact, psychosocial variables, such as age, preexisting relationship conflicts, preoperative satisfaction with sex life, and religious beliefs, are the most important determinants of sexual function7,25,29; therefore we excluded those patients who had psychiatric symptoms and those who were sexually inactive in the preoperative period. The age and menopausal status were similar between the groups.
We found that the risk of the development of dyspareunia significantly increased after the LH or TAH, with an incidence of 4.8%, and this result was similar in both groups. Our results showed that this risk may be due to the greater decrease in the length of the vagina. One possible explanation may be that the more the vaginal length decreases, the more the sensory nerves are damaged. The source of genital stimulation may also affect the impact of a hysterectomy on sexual function. 7 One can expect a decrease in the sexual response and an increase in dyspareunia after a hysterectomy if the patient prefers vaginal and/or cervical stimulation instead of clitoral stimulation. 7
The effect of a simple hysterectomy on urinary symptoms and vesicourethral function remains controversial. 30 It has been suggested that the disruption of lower pelvic innervation during a hysterectomy may be the reason for bladder instability and urinary dysfunction after surgery 17 ; however, an earlier study failed to support this theory. 31 A recent systematic review of nine prospective studies published before 2009 showed that a simple hysterectomy does not adversely impact the urodynamic outcomes, nor does it increase the risk of urinary symptoms; in fact, it may even reduce the symptoms of urinary incontinence. 17 Additionally, prospective clinical studies, including pre- and postoperative urodynamic studies, have been reported to be necessary to detect the effects of a hysterectomy on lower urinary functions. 14
In a prospective study that compared the effects of LH and TAH on vesicourethral function, the maximum cystometric capacity was found to be increased significantly, and the Q-max was found to be stable following both types of hysterectomy. 11 The meta-analysis of the bladder capacity before and after a hysterectomy showed ambiguous results: some studies reported an increase, and others reported a decrease, in the bladder capacity. We found a significant reduction in the bladder capacity and a significant increase in the Q-max after a hysterectomy. None of these findings differed between the two hysterectomy groups. Advanced age, multiparity, obesity, and postmenopausal status were linked to a greater risk of urinary dysfunction 32 ; therefore obese patients were excluded from our study, whereas the age, parity, and menopausal status were similar between the groups.
Limited numbers of studies regarding the effects of the type of hysterectomy on the vaginal length, dyspareunia, or lower urinary tract function have been published, and controversial results have been reported. This study includes the largest sample size to date.
Conclusions
The results of our study suggest that the change in the length of the vagina is much more remarkable after a TAH compared with an LH. The dyspareunia rates increased after a hysterectomy regardless of its type. Additionally, we found a significant increase in the Q-max and a significant reduction in the bladder capacity, which is incompatible with the studies published so far. Still, further prospective clinical studies are warranted to ascertain whether an LH causes less damage to the pelvic floor compared with an abdominal hysterectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
M.P. was responsible for project development, data collection, and critical review. I.K. was responsible for data analysis, literature search, and manuscript writing and editing. T.S. was responsible for data collection. B.S. was responsible for data collection and manuscript editing. E.O. was responsible for manuscript preparation. A.K. was responsible for protocol development, data analysis, manuscript editing, and critical review.