
Abstract
Abstract
Background:
Although the feasibility of laparoscopic appendectomy (LA) in complicated appendicitis (CA) has been demonstrated, LA is typically underused in CA due to its high conversion rate. However, little is known regarding the clinical course of conversion in CA.
Materials and Methods:
Between January 2005 and April 2012, 1699 patients older than 16 years underwent an appendectomy at our institution. Of these, 207 were confirmed to have CA, which was defined as operative findings of gangrenous or perforated appendix, with or without abscess formation. Patients were divided into the following three groups: open group (OG), laparoscopy group (LG), and converted group (CG). Perioperative outcomes were compared between the three groups.
Results:
Thirty-eight patients underwent open surgery. Among the 169 patients for whom laparoscopic surgery was originally attempted, 20 (11.8%) were converted. Operation time was significantly longer and estimated blood loss was higher in the CG than in the other groups. Fewer overall complications were observed and the length of hospital stay (LOH) was shorter in the LG than in the OG and CG. However, no significant differences were observed between the OG and CG regarding the overall complication rate or LOH. Operation method was the only factor associated with postoperative morbidity in multivariate analysis.
Conclusion:
While completion by laparoscopy was associated with better outcomes than the other two procedures at all levels, open conversion did not increase the overall morbidity or LOH compared with open appendectomy. Laparoscopic approach could be a viable option even in the management of CA.
Introduction
A
Laparoscopic appendectomy for complicated cases requires a higher technical skill compared with other approaches. Recently, two randomized controlled trials comparing open and laparoscopic surgery in complicated appendicitis (CA) reported similar recovery outcomes.6,7 One of the main reasons underlying the hesitation to adopt laparoscopic surgery in CA is the possibility of conversion. The conversion rate of CA is known to be higher compared with uncomplicated appendicitis. 8 From this perspective, little is known regarding the impact of conversion during the laparoscopic management of CA.
In our institution, the operative approach for patients with CA is based on each surgeon's preference. To investigate the clinical impact of conversion in CA, a retrospective study was conducted to compare the clinical outcomes of open appendectomy, laparoscopic appendectomy, and converted appendectomy in CA.
Materials and Methods
Patients
Between January 2005 and April 2012, a total of 2095 patients underwent appendectomy at Gangnam Severance Hospital, Yonsei University College of Medicine. Among the 1699 patients who were older than 16 years, 216 were confirmed to have CA, defined as operative findings of gangrenous or perforated appendix, with or without abscess formation. 9 Patients who underwent combined resection (cholecystectomy or oophorectomy) or interval appendectomy were excluded. Thus, 207 patients were finally included in this study. Patients who underwent ileocecectomy were also included in this study in terms of “intent-to-treat” (Fig. 1).
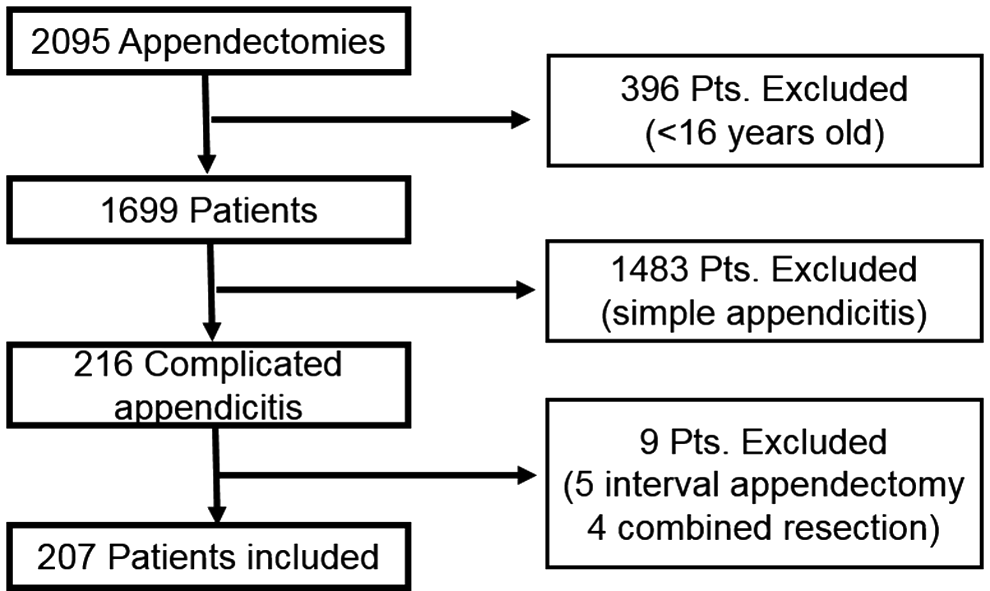
Patient selection for the evaluation of the impact of conversion in complicated appendicitis.
A total of 38 patients underwent open appendectomy, whereas a laparoscopic approach was attempted for 169 patients. Twenty patients were converted to the open procedure and then categorized in the converted group (CG). The other 149 patients, for whom the laparoscopic procedure was completed, were assigned to the laparoscopic group (LG). This study was approved by our Institutional Review Board.
Surgical procedure
The initial choice of surgical treatments depended upon the severity of the appendicitis, as assessed by laboratory and image findings. Although the open surgery was also chosen based on the surgeon's preference or the patient's general conditions, the correct reason for choosing open surgery could not be identified in this retrospective study.
Each operation in the three groups was performed after the same preparation method. All operations were performed under general anesthesia, and all patients received second-generation intravenous cephalosporin with/without metronidazole during the induction of anesthesia. The abdomen and suprapubic region were shaved before starting each operation. The umbilicus was also cleaned thoroughly for all laparoscopic procedures.
For open appendectomy or open conversion cases, a 5–8 cm McBurney skin incision was made on the right lower quadrant. Alternatively, a paramedian skin incision was made. Through the incision, the cecal base was found and pulled outside of the peritoneal cavity with the complicated appendix. The appendix was dissected and transected in a conventional method.
For laparoscopic appendectomy, a conventional three-port approach (using a 12-mm umbilical port with two additional 5-mm ports in the left lower abdomen and suprapubic area) was performed. Using monopolar electrocautery and repeating repeated dissection and suction, the complicated appendix and the appendiceal artery were identified. After the appendiceal artery was ligated with endoclips, the appendix was ligated thrice with endoloops and transected by an endoscopic scissor from the base of the cecum. The appendiceal stump was cauterized and the specimen was retrieved using a lap bag through the 12-mm port. Abdominal irrigation was performed after specimen retrieval according to the surgeon's preference. A Jackson-Pratt drain was inserted to eliminate the contaminated intraperitoneal fluid. The decision to insert a drainage tube was made by the operating surgeon at the end of the procedure.
Measurement of postoperative outcomes
Postoperative outcomes were retrospectively analyzed to compare the usefulness of the three surgical methods. Data were collected by reviewing the medical records of each patient. Collected data included body mass index (BMI), American Society of Anesthesiology (ASA) grade, surgical method, operation time, estimated blood loss (EBL), appendix size, complications, and length of hospital stay (LOH).
Statistical analysis
Groups were compared on an intention-to-treat basis. The differences in clinicopathologic features and perioperative outcomes among the OG, LG, and CG groups were analyzed using the two-sided Pearson's chi-square test or Fisher's exact test for categorical variables and with ANOVA or the Kruskal–Wallis test for continuous variables. Exact logistic regression analysis was also performed for the multivariate analysis of factors associated with morbidity or open conversion. A P value <.05 was considered to indicate statistical significance. All calculations and analyses were performed using the SPSS software package version 20.0 (IBM Corp., Armonk, NY).
Results
Patient characteristics
Patients were allocated into the open group (OG, n = 38, 18.3%), laparoscopic group (LG, n = 149, 71.9%), or converted group (CG, n = 20, 9.6%). No significant differences regarding sex, BMI, or ASA grade were observed between the three groups. However, patients in the OG were significantly older than those in the other groups (P = .001). Moreover, the duration of symptoms before admission to the hospital was shorter in the LG than in the others (P < .001) (Table 1).
Fisher's exact test.
ASA, American Society of Anesthesiology; BMI, body mass index; SD, standard deviation.
Factors associated with open conversion
For the 169 patients for whom laparoscopy surgery was attempted, potential associations of clinical factors with conversion were investigated. No differences of conversion rate were associated with sex, age, BMI, ASA grade, or preoperative white blood cell count. However, dichotomization of symptom duration before admission to the hospital into <3 or >4 days revealed that symptom duration was the only factor associated with conversion (8.5% in <3 days versus 23.1% in >4 days, P = .022) (Table 2).
Fisher's exact test.
ASA, American Society of Anesthesiology; BMI, body mass index; SD, standard deviation.
Perioperative outcomes
The operative results associated with each procedure are shown in Table 3. The CG exhibited a longer operation time than the other groups (152 minutes in CG versus 91 minutes in OG versus 91 minutes in LG, P < .001). The EBL and rate of ileocecectomy were both lower in the LG than the in the others (P = .002 and P = .003, respectively). The overall complication rate was lowest in the LG (16.8%, P < .001), whereas morbidity was similar between the OG and CG. Wound infection was the most common complication in all three groups; moreover, the rate of wound infection was similar between the OG and CG. The LG showed the lowest wound infection rate out of all three groups (P = .001). The LOH was significantly shorter in the LG (median 4 days, range 1–18), while the OG and CG showed similar LOHs [median 8 days in OG (range 4–32) versus median 9 days in CG (range 4–16), P < .001].
Fisher's exact test.
Kruskal–Wallis test.
EBL, estimated blood loss; SD, standard deviation.
Factors associated with postoperative complications
In univariate analysis, BMI and operation methods were both associated with morbidity. Operation method was the only factor associated with postoperative morbidity in multivariate analysis (Table 4).
Fisher's exact test.
ASA, American Society of Anesthesiology; BMI, body mass index; CI, confidence interval; HR, hazard ratio.
Discussion
This study found that conversion from laparoscopy to open surgery in CA did not jeopardize recovery outcomes in comparison to open surgery. In addition, laparoscopic surgery completed without conversion was associated with less morbidity and a reduced hospital stay. Therefore, laparoscopic surgery is a potentially suitable initial treatment choice in the management of CA.
Although laparoscopic surgery has been shown to be beneficial for CA,10–13 most previous studies were retrospective in design. Recently, a randomized controlled trial with a small sample size that compared laparoscopy and open surgery for CA showed similar outcomes with respect to postoperative recovery, hospital stay, and postoperative complications. 6 Another similar study did not observe any additional benefit of laparoscopy compared with open surgery. 7 It has been hypothesized that the abdominal contamination induced by the inflammation in CA may lessen the benefits of laparoscopic surgery in early postoperative periods. 6 In addition, the higher rate of postoperative abdominal abscess formation after laparoscopic surgery has been a typical reason for hesitating to apply laparoscopy in CA.14–16
The conversion rate in CA has been found to range from 2.7% to 26%.11,13,17,18 Dimitriou et al. reported a higher conversion rate in CA than in acute appendicitis (13.1% in CA versus 3.7% in acute appendicitis). 8 Wagner et al. demonstrated that advanced age, ASA score greater than 2, CT inflammation grade ≥4, and attending surgeon inexperience were independent predictors of conversion. 19 Liu et al. reported that age older than 65, diffuse tenderness on physical examination, a surgeon with less experience in laparoscopic surgery, and significant fat stranding associated with fluid accumulation, inflammatory mass, or localized abscess in CT scans were associated with conversion. 18 In our study, the conversion rate was 11.5%. The most common reason for conversion was severe adhesions with/without localized perforations. Among the clinical factors examined in this study, duration of symptoms before admission to the hospital was significantly associated with conversion in univariate analysis. Since abdominopelvic CT was not performed for all of the patients in this study, we were unable to investigate the extent to which CT findings are predictive of conversion. However, our data showed that longer durations from symptoms to admission to the hospital are a potentially simple predictor of severe appendicitis.
In our analysis, the wound infection rate was significantly lower in the laparoscopy group. The lower wound infection rate in this group may be related to the routine use of an endoscopic bag for removal of the specimen. This approach can avoid direct contact between a contaminated appendix and visceral or fascial surfaces. In contrast, another study found that the converted group was associated with higher postoperative infectious morbidity for perforated appendicitis. 14 Cho et al. also reported that open conversion was a significant predictor of surgical site infections. 20 Likewise, our analysis showed that the converted group showed a higher wound infection rate than the laparoscopy group. Interestingly, the rate of wound infection in converted group was similar to that of the open surgery group. Wound protection has been reported to diminish the surgical site infection rate. 21 During the study periods, wound protection was not routinely applied in either the open or the converted group. Further investigations are needed to determine if a wound protection system can effectively reduce the wound infection rate in CA.
The rates of postoperative abscess formation in CA have been reported to range from 0 to 22.9% in open appendectomy and 2.7 to 14% in laparoscopic appendectomy.10,13,15,16,22,23 Paik et al. reported that postoperative abscess formation after surgery for perforated appendicitis was significantly higher in the laparoscopic approach than in the open approach (9.0% in laparoscopy versus 2.7% in open surgery). 24 In this retrospective study, the overall rate of abscess formation (2.8%) was lower than has been previously reported. In addition, the three groups did not exhibit significantly different abscess formation rates. A protective Jackson-Pratt drain was inserted in almost all patients in the open and converted groups, whereas suction drainage was used less often in the laparoscopic surgery group. Protective drain insertion and adequate conversion in cases of severe inflammation or adhesions might be possible reasons underlying the lower rate of postoperative abscess formation. However, further investigations are needed to determine whether drain insertion can effectively reduce the rate of postoperative abscess formation.25,26
The main limitation of our study is its retrospective design. In our study, laparoscopic surgery completed without conversion was associated with less morbidity and shorter hospital stays than converted or open procedures. However, our study was also subject to some selection bias. For instance, the initial surgical approach was decided by surgeon preference and/or the general conditions of the patient. Moreover, the open surgery group contained a higher proportion of older patients than the laparoscopic and converted groups. Furthermore, the mean duration of symptoms before admission to the hospital was shortest in the laparoscopic surgery group (Table 1). Therefore, the improved outcomes in the laparoscopy group in our study do not conclusively demonstrate the superiority of laparoscopic surgery in CA. One important finding of this study was that the converted group showed similar clinical outcomes to the initial open surgery group, even though the clinical course in this group was delayed compared with the laparoscopy group.
Taguchi et al. reported one successful interval appendectomy after laparoscopic drainage and proposed that the use of a laparoscopic approach in CA could reduce the fear of failing to remove the severely inflamed appendix. 6 We found that conversion to open surgery in CA did not jeopardize the clinical outcomes compared with initial open surgery, a conclusion that may also help lessen a surgeon's hesitation to apply laparoscopic surgery for the treatments of CA.
In conclusion, although open conversion was associated with prolonged operation times and increased blood loss, the clinical outcomes of open conversion were not inferior to those of open surgery. However, completion by laparoscopy yielded the best outcomes. These findings suggest that laparoscopy could be a viable option even in the management of CA.
Footnotes
Disclosure Statement
No competing financial interests exist.