
Abstract
Abstract
Background:
The treatment of long-gap esophageal atresia remains an issue for pediatric surgeons. Many techniques for treating long-gap esophageal atresia have been proposed, but the optimal method has not been established. The thoracoscopic esophageal elongation technique has recently been developed. We previously reported a case in which two-stage thoracoscopic repair was performed using internal esophageal traction without esophageal tearing, and we retrospectively reviewed the outcomes of this procedure in this study.
Methods:
Five patients underwent thoracoscopic treatment involving internal esophageal traction for esophageal atresia involving a long gap or vascular ring over a 5-year period.
Results:
Between November 2010 and November 2015, 5 patients were treated with thoracoscopic traction. All of these patients successfully underwent thoracoscopic-delayed primary anastomosis. Conversion to open thoracotomy was not required in any case. The postoperative complications experienced by the patients included minor anastomotic leakage in 2 cases, anastomotic stenosis in 1 case, gastroesophageal reflux (GER) in 4 cases, and a hiatal hernia in 1 case. None of the patients died.
Conclusions:
Two-stage thoracoscopic repair for esophageal atresia involving a long gap or vascular ring is a safe and feasible procedure; however, we must develop methods for treating minor anastomotic complications and GER due to esophageal traction in future.
Introduction
L
Materials and Methods
Between November 2010 and November 2015, 5 consecutive patients, including 3 patients with pure esophageal atresia, 1 patient with a type C tracheoesophageal fistula (TEF), and 1 patient with a TEF associated with a right aortic arch and a vascular ring, underwent thoracoscopic treatment involving internal esophageal traction at our two institutions. In all cases, thoracoscopic internal esophageal traction was performed during the initial operation, and thoracoscopic-delayed primary anastomosis was carried out during a subsequent procedure. 8 The patients' ages at the time of the first operation ranged from 0 to 3 days, and their ages at the time of the second operation ranged from 6 to 24 days. The patients' birthweights ranged from 2115 to 2661 g. The associated malformations included an atrial septal defect/ventricular septal defect in 1 patient, VATER * association in 1 patient, and a right aortic arch with a vascular ring in 1 patient. The vertebral gap between the proximal and distal esophagus ranged from 1 to 6 vertebrae in length (Table 1).
ASD/VSD, atrial septal defect/ventricular septal defect; VATER, vertebral anomalies, anal atresia, tracheo-esophageal fistula, renal anomalies, and limb abnormalities.
Gastrostomy procedure and thoracoscopic technique
All patients underwent gastrostomy. Tracheal intubation was performed with an endotracheal tube, and we confirmed the position of the TEF using a bronchofiberscope. Then, the patient was placed in the semiprone position. A 5-mm bladeless trocar was initially inserted at a point along the fifth or sixth intercostal middle axillary line under thoracoscopic observation with a 5-mm, 0-degree telescope to prevent lung damage and the leakage of carbon dioxide from around the port. The pleural cavity was inflated at 6 mmHg and a flow rate of 0.5 L/min, and was then maintained at a pressure of 4–6 mmHg. A 5-mm, 30-degree telescope was inserted through the first port. Two additional ports were also produced: a 3-mm port was made along the third intercostal middle axillary line and a 3-mm port was made along the sixth or seventh intercostal posterior axillary line. The azygos vein was not ligated. The proximal esophagus was extensively dissected toward the cervical section, and the distal esophagus was also gently dissected and mobilized down to the diaphragm. TEFs were ligated with 4-0 absorbable sutures and divided if they were confirmed to be present. A traction suture (a 5-0 absorbable suture) was applied to both ends of the esophagus using pledgets to prevent the esophageal ends tearing (Fig. 1). In two cases, we attempted, but subsequently had to abandon, thoracoscopic primary anastomosis. Strong anastomotic tension was noted in one case involving a TEF, and the proximal esophageal pouch was located within a vascular ring in the other case. A traction suture was inserted through the cranial and caudal intercostal spaces using a laparoscopic percutaneous extraperitoneal closure needle, and suitable tension between the esophagus and the costal bone was achieved, as reported previously. 8
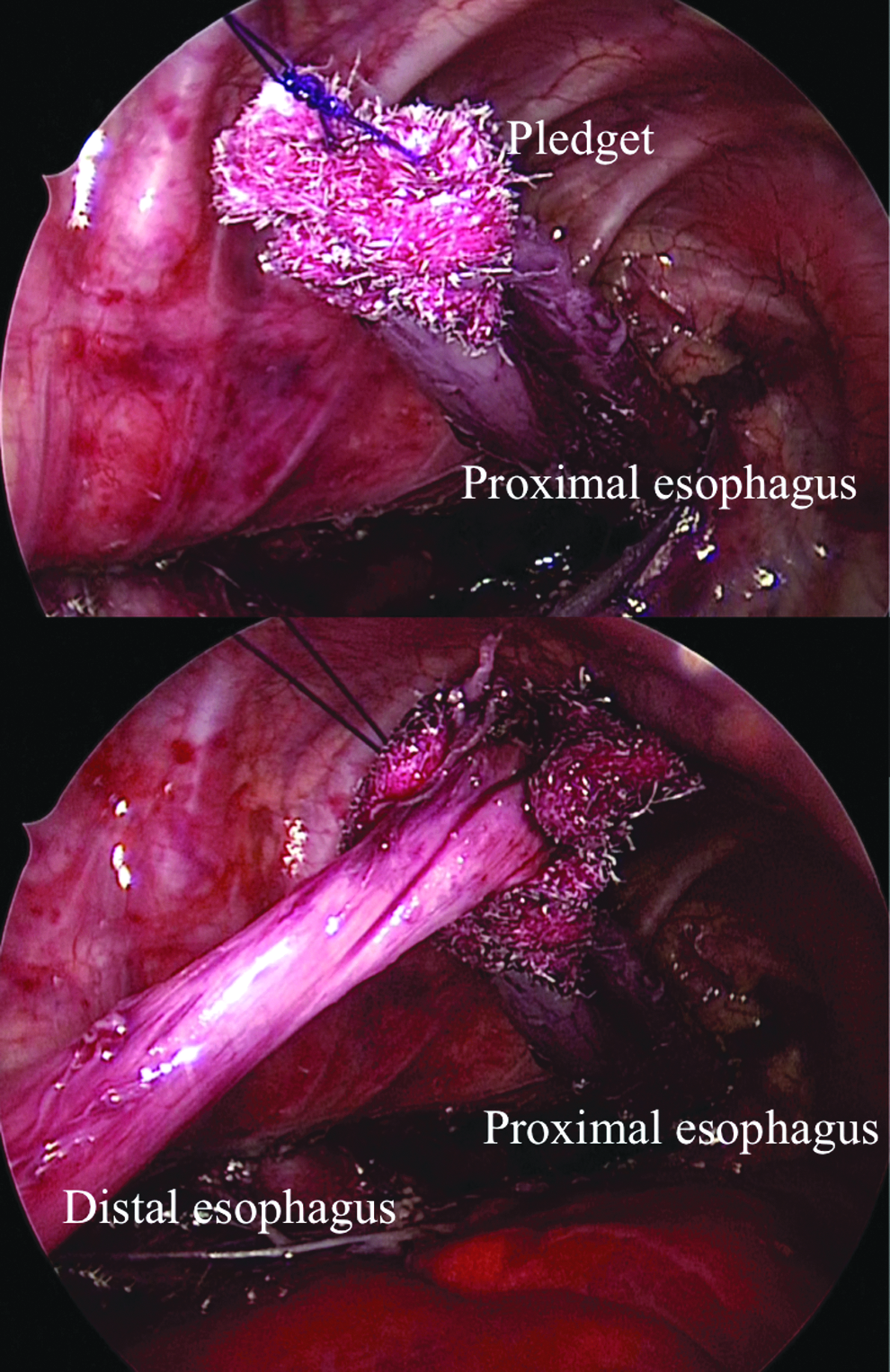
Thoracoscopic internal esophageal traction with pledgeted sutures.
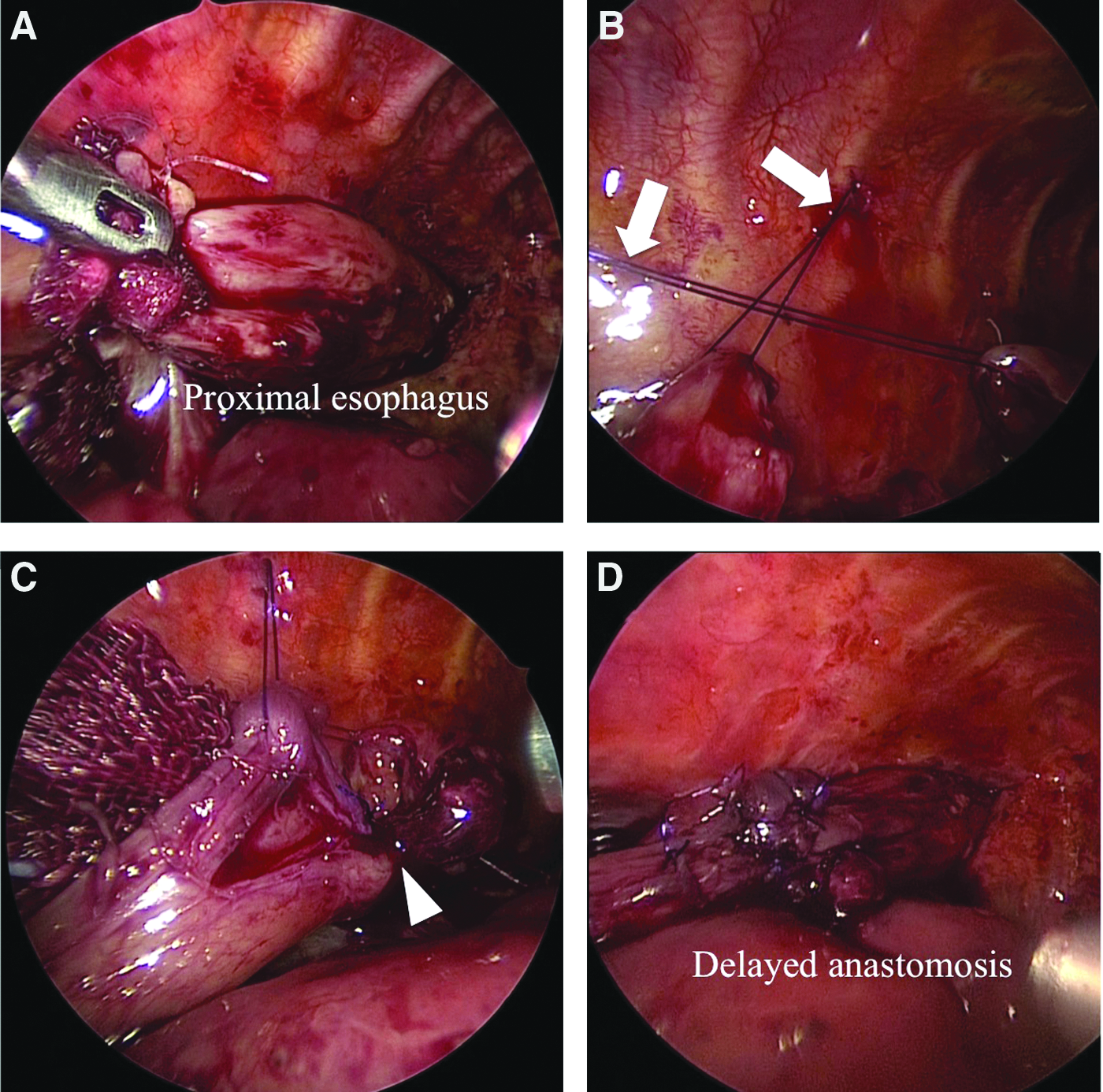
After about one week, the patient was taken back into the operation room to undergo the delayed primary anastomosis procedure. After thoracoscopic adhesiolysis had been carried out by carefully sweeping any adhesions between the esophagus and the lung, both esophageal ends were mobilized (Fig. 2A) and subjected to traction, and then tension was applied to determine whether anastomosis was possible. Next, both esophageal ends were opened and pulled closer together using traction sutures (Fig. 2B). These traction sutures facilitated the thoracoscopic-delayed primary anastomosis by decreasing the degree of anastomotic tension (Fig. 2C, D). A chest drain was inserted in all cases.
A fluoroscopic contrast-enhanced study was performed about one month after the second operation to examine the esophagogastric configuration and evaluate the severity of any anastomotic stricture or sliding hernias. Anastomotic leakage was diagnosed based on the drainage contents of the chest tube. The timing of tube feeding was decided based on the patient's condition.
We retrospectively reviewed the patients' intraoperative and postoperative outcomes, including the operative time, intraoperative blood loss, conversion rate, the duration of the postoperative hospitalization period, postoperative complications, and mortality, and evaluated the feasibility of the two-stage thoracoscopic repair of esophageal atresia.
The study protocol was approved by each of the relevant hospital medical ethics committees.
Results
All patients successfully underwent thoracoscopic definitive primary anastomosis after thoracoscopic esophageal elongation using internal traction. In 4 cases, esophageal internal traction was performed because of long-gap esophageal atresia involving a gap of more than four vertebrae. In the remaining case, which involved a one-vertebra gap, we confirmed the presence of a vascular ring, abandoned the thoracoscopic primary suturing procedure, and decided to perform left-sided thoracoscopic TEF ligation and esophageal traction during the first operation. Detailed examinations that were carried out after the first operation showed that a patent ductus arteriosus (PDA) completed the vascular ring, so left-sided delayed primary anastomosis and dissection of the PDA were performed during the second procedure. 9 The patients' operative and postoperative outcomes are shown in Table 2. The mean operative times for the first and second operations were 230 and 214 minutes, respectively, and less than 5 mL blood loss occurred during both operations. None of the patients required conversion to open thoracotomy. Tubal feeding and oral feeding were started at 10 and 45 days after the second procedure, respectively. Two patients (40%) developed minor anastomotic leakage, which was treated conservatively. Anastomotic stenosis developed in 1 patient, who did not require endoscopic dilation as the stenosis was ameliorated using a conservative approach. The other postoperative complications experienced by the patients included gastroesophageal reflux (GER) in 4 patients, a hiatal hernia in 1 patient, and others in 1 patient. There were no deaths in this study. All 5 patients were followed up, and the duration of the follow-up period ranged from 7 to 67 months. A good weight gain was seen in all patients.
Discussion
Long-gap esophageal atresia remains an important challenge for pediatric surgeons. Many techniques for treating long-gap esophageal atresia have been developed, but none have proved ideal. Long-gap esophageal atresia used to eventually be treated with esophageal replacement.2–4 However, it was reported that this resulted in high postoperative morbidity and mortality rates. 10 The open traction technique was recently described by Foker. 5 In this technique, esophageal traction is applied day by day to elongate the ends of the esophagus, before an anastomosis is performed through a thoracotomy. Foker et al. were able to overcome long gaps (5.5 to 6.8 cm) in this manner. Kimura also reported another technique involving the translocation of the proximal esophagostomy along the anterior chest wall, but this approach often requires elongation to be performed multiple times before the primary anastomosis can be carried out. Three of the 8 (38%) patients who underwent this technique suffered minor leakage, and all 8 patients developed anastomotic stenosis. 6 Thus, these surgical techniques are complex and result in high rates of postoperative complications.
The successful use of a thoracoscopic Foker-like elongation technique and delayed primary anastomosis as a treatment for long-gap esophageal atresia were reported by van der Zee et al. 7 This approach made it possible to perform minimally invasive surgery in cases of long-gap esophageal atresia. Recently, the outcomes of this procedure were reported. 11 The two-stage repair of long-gap esophageal atresia was successful in 8 of the 10 patients. However, thoracoscopic esophageal elongation failed in the remaining 2 patients; the length of the esophageal pouch did not increase in one case, and esophageal perforation occurred in the other case. External traction of the esophagus was carried out during the first operation in all of these cases. In Foker's method, both esophageal ends were handled as minimally as possible, and esophageal traction was applied day by day to elongate the ends of the esophagus, which carried a risk of disruption of the esophageal ends. Contrary to Foker's method, our thoracoscopic internal traction method involved sufficient dissection of both esophageal ends during the first operation and constant esophageal traction. We then waited for the esophageal blood supply to recover and monitored the patient for esophageal injuries, before we successfully completed the definitive delayed primary anastomosis. 8
In our study, all of the patients exhibited small amounts of adhesion around the ends of the esophagus, but no intrathoracic infections or esophageal tearing occurred. No relationship was detected between the degree of adhesion and the time between the first and second operations. We were able to easily dissect between the esophageal ends and the lungs in all patients, and little intraoperative blood loss occurred. The median time between the first and second operations was 10 days. However, van der Zee suggested that traction that lasted for longer than 5 days did not lead to any further gain in esophageal length. 11
The use of pledgeted sutures and the absence of further traction should help to eliminate tearing at the esophageal ends, and there were no cases of such tearing in our study. However, Al-Qahtani reported that the sutures pierced the esophageal pouch in both cases in which they used pledgeted sutures combined with daily esophageal traction. A less reactive suture or pledget material might help to minimize inflammation and further reduce the risk of complications. 12
Three of the 5 patients in our study suffered anastomotic complications, and 2 and 5 of the 8 patients in Zee's study developed minor leakage and anastomotic stenosis after primary anastomosis, respectively. There were no cases of mortality in Zee's study. 11 Foker's open technique frequently resulted in anastomotic complications, which sometimes required additional surgery, although the long-term outcomes of this approach were good.12,13 Two-stage repair of esophageal atresia is frequently associated with minor anastomotic leakage, and strictures can be treated with open surgery or thoracoscopy. GER occurred frequently in this study (in 4 of 5 patients) and Zee's study (in 7 of 8 patients). Two-stage esophageal anastomosis shortens the esophagus and pulls the stomach into the mediastinum. This can result in a physiological hiatal hernia, which increases the risk of GER. We must develop ways to overcome postoperative GER; however, it is difficult to resolve such problems because the distal esophagus must be pulled upward in cases of long-gap esophageal atresia, so esophago-esophageal anastomosis results in a distended His angle.
Compared with open surgery, thoracoscopic esophageal operations are associated with less adhesion, a small amount of bleeding, similar postoperative complications rates, and better cosmetic results. We primarily select thoracoscopic procedures for both pure esophageal atresia and cases involving hemodynamically stable patients with TEF. If strong anastomotic tension is noted during the first operation, an internal esophageal traction is performed.
A right aortic arch is found in 5% of neonates with TEF and might be associated with vascular rings. If a right aortic arch is found during the first operation, such as in case 4, only ligation of the TEF should be performed, and then a computed tomography examination should be carried out to search for a vascular ring and determine the optimal approach for the second operation.
Conclusion
In conclusion, thoracoscopic internal traction and subsequent thoracoscopic delayed primary anastomosis for cases of esophageal atresia involving a long gap or vascular ring are safe and feasible procedures. Further innovations are required to overcome postoperative GER.
Footnotes
Disclosure Statement
No competing financial interest exists.