
Abstract
Abstract
Aim:
With consideration of the theoretical link between the stent insertion and the increased risk of tumor cells spillaged, which may lead to distant metastases, there is a concern about long-term clinical outcomes after the usage of self-expanding metallic stents (SEMS) as a “bridge to surgery” in the malignant colorectal obstruction (MCO) treatment. This cohort study aimed to compare the long-term oncological outcomes of SEMS as a bridge to surgery (SEMS group) with those of emergency surgery (ES group) for MCO.
Methods:
Twenty-seven patients who underwent semielective curative resection after endoscopic SEMS insertion were included from October 2007 to December 2012 in the SEMS group were compared with 33 patients who underwent emergency curative surgery for MCO during the same period in the ES group. The clinical pathologic characteristics and the overall survival (OS) rate were compared between the two groups.
Results:
There were no significant differences in demographics, tumor stage, location, and histology between the SEMS and ES groups. The median OS times were 37 months for the SEMS group and 23 months for the ES group. The proportions of patients who received postoperative adjuvant chemotherapy were comparable (SEMS group versus ES group, 70.4% versus 45.5%; P = .138). There were no significant differences in terms of the long-term oncological outcome between two groups in the 3-year OS rate (55.6% versus 39.4%; P = .2119) and the 5-year OS rate (48.1% versus 36.4%; P = .3570).
Conclusions:
Long-term oncological outcomes of the SEMS group were comparable to those of the ES group.
Introduction
C
In 1990, when self-expanding metallic stents (SEMS) for the treatment of malignant colorectal obstruction (MCO) were introduced for the first time, SEMS have been used as an alternative to ES. 11 Some studies show that SEMS enable primary anastomosis with a single-stage operation, reduce mortality and morbidity caused by ES, lower the rate of stoma formation, represent definitive palliation, obviate more invasive surgical interventions, and avoid a stoma and facilitate early administration of other treatments such as chemotherapy in patients with distant metastatic CRC presenting with acute obstruction.12–14 It has been reported that SEMS can decompress the obstructed bowel, provide an opportunity to clean the colon, allow physicians more time to perform a precise preoperative evaluation, and make patients become candidates for laparoscopic resection when used as a bridge to surgery.15–17 Despite these advantages, SEMS placement can cause complications, such as bleeding, perforation, stent displacement, stent migration, and restenosis.12,18 There are, however, concerns that the usage of SEMS may adversely affect the oncological outcomes. The principles of hematogenous spread of tumor cells by mechanical handling of cancers have been known for some time, leading to the development of a variety of minimal handling techniques. Studies have detected tumor cells in the peripheral blood of patients with colorectal malignancies undergoing colonoscopy, endorectal ultrasound scan, and stenting. Consequently, there is a potential to worsen the development of a potentially curable disease into a noncurable state.19–21 As is shown above, there is still controversy about the clinical outcomes, especially the long-term oncological safety of SEMS applying for MCO,22,23 more consideration and research on long-term oncological outcomes, such as survival rates after SEMS insertion, is still in need.
The objectives of this study were to compare the long-term oncological outcomes of SEMS as a bridge to surgery (SEMS group) with those of ES group for MCO, with respect to the long-term oncological safety.
Materials and Methods
Patients and study design
The MCO was defined by the presence of clinical symptoms or signs of bowel obstruction caused by CRC. The patients with MCO were included in this study. The signs of obstruction were defined as (1) distended proximal bowel, liquid surface, transitional zone, or collapsed distal bowel on abdominal CT scans or (2) in the colonoscopic evaluation, it is impossible to pass through the stenotic area. The clinical symptoms of MCO were defined as (1) constipation, (2) abdominal bloating, (3) vomiting, (4) or abdominal pain, and the patients who had at least three of the four symptoms were enrolled in the study.
Between October 2007 and December 2012, 74 patients with acute MCO of CRC were admitted to Chang-Hai Hospital and 12 patients of inoperable disease were excluded. For the remaining patients, doctors, patients, and families had a conversation about the treatment options and risks before operation. Based on the previous results and experiences, SEMS was the first option for patients with acute MCO of CRC in our center. We suggested patients to receive SEMS as a bridge to surgery. However, some patients and families rejected our suggestions for the reasons such as the cost of treatment (in China, SEMS is not included in healthcare insurance) or the relatively longer treatment period. As a result, ES was done for 33 patients (ES group), and SEMS were placed as a bridge to surgery on 29 patients. From the 29 patients, we additionally excluded 2 patients who underwent fluoroscopy-guided stent insertion. We retrospectively reviewed the medical records of patients in the two groups, including age, gender, comorbidity, tumor stage, site of obstruction, tumor size, surgical procedure, adjuvant chemotherapy after surgery, and time to death.
This study was designed in a case–control pattern. The 27 patients in the SEMS group were matched to the subjects in the control group based on age (±5 years), sex, and TNM staging according to the 7th American Joint Committee on Cancer, as possible. The study was approved by the Ethics Committee of the Changhai Hospital and was conducted in accordance with the Declaration of Helsinki.
SEMS insertion
In our center, we use a two-person approach to colonoscopy. SEMS insertions were performed using a conventional endoscope (CF-H260,Olympus, Tokyo, Japan) by seven experienced, qualified endoscopists (E.-d.Y., Z.L., Rong-gui Meng, W.Z., Lian-jie Liu, Han-tao Wang, Li-qiang Hao, et al.) without fluoroscopic monitoring. Patients underwent cleansing enemas for bowel preparation and accepted insertion without sedation. Before stent insertion, general condition of patients needed to be evaluated, and three indicators associated with tumor (the site, length, and degree of obstruction) were assessed by at least one of the three inspection methods: colonoscopy, conventional CT, and upright abdominal films. The stent size (diameter, 18–24 mm, the most commonly used were 20, 22, and 25 mm) and length (80–170 mm, the most commonly used were 90 mm) were chosen according to the measured length of the obstruction, and uncovered SEMS were used as a bridge to surgery. The length of the stent was at least 3 cm longer than the stenosis at both sides to allow for adequate margins. Specific methods: inserted endoscope to the tumor site of obstruction, repeatedly washed using normal saline to expose the narrow hole of tumor. A flexible guidewire was inserted through the endoscope channel, then passed through the obstructive lesion under endoscopic guidance without fluoroscopy. 24 Once the stent had been inserted along the guidewire across the obstruction by endoscopy through the endoscope channel, the stent was deployed through direct endoscopic guidance. After placement, the correct position and expansion of the stents were confirmed by simple abdominal radiography.
Emergency surgery
All emergency surgeries were performed by five experienced surgeons who were familiar with colorectal procedures. The type and extent of surgeries were determined by the treating surgeon in charge according to the tumor location, clinical stage, and the general health condition of the patient. The surgeon tried his best to pursue a single-stage resection with a primary anastomosis. A Hartmann's operation was performed, if primary anastomosis was not possible.
Clinical outcomes
Long-term oncological outcomes were compared between the two groups. The last follow-up was based on the review of hospital records. The patients who did not attend a scheduled visit within 1 year after the previous visit were considered loss to follow-up and were censored. Overall survival (OS) rate was defined as the time interval from the date of operation or SEMS insertion to either death or the last follow-up visit.
Statistical analyses
Data were analyzed using SPSS software (version 19.0; SPSS, Chicago, IL) and MedCalc software (version 13.0.0.0; MedCalc software, Mariakerke, Belgium). Patient demographics and clinical characteristics were expressed as the mean and standard deviations or as numbers (percentages). The mean of continuous variables were analyzed between two groups using Student's t-test, and categorical variables were analyzed by the Chi-square test or Fisher's exact test. The mean of the variables that were not distributed normally were compared with the Mann–Whitney U-test. Survival analysis was performed using Kaplan–Meier method, and the findings were compared using a log-rank test and Cox regression. P < .05 was considered statistically significant.
Results
Baseline characteristics
The mean ages of the SEMS group and the ES group were 60.44 ± 14.11 and 59.36 ± 14.47 years, respectively. The groups were well balanced with regard to clinical variables, such as age, gender, comorbidity, and adjuvant chemotherapy status (P = .722, P = .099, P = .387, and P = .138, respectively, Table 1). In the SEMS group there were 3 patients with hypertension only, 3 patients with diabetes only, and 1 patient with hypertension and coronary heart disease, whereas in the ES group there were 6 patients with hypertension only, 4 patients with diabetes only, 1 patient with hypertension and cerebral infarction, and 1 patient with diabetes and cerebral infarction. There were also no significant differences in terms of the location, stage, and differentiation of tumor characteristics between the groups (Table 2). The tumors were mainly located in the sigmoid colon and rectum, but the overall distribution did not differ between the two groups. Seventeen patients (9 patients in the SEMS group and 8 patients in the ES group) had liver or lung metastases at the time of initial presentation. In our center, two of these patients underwent metastasectomy synchronously with colectomy, whereas others did not undergo metastasectomy synchronously with colectomy, although some metastases were resectable.
Values are presented as mean ± standard deviation or n (%).
t-test.
chi-square test.
ES, emergency surgery; SEMS, self-expanding metallic stents.
Values are presented as mean ± standard deviation or n (%).
Chi-square test.
Wilcoxon rank-sum test.
ES, emergency surgery; SEMS, self-expanding metallic stents.
Only uncovered stents were used for the SEMS group. The median time interval from the stent placement to the surgery was 14 (range 2–89) days. Two patients experienced a longer wait (89 and 87 days, respectively) before surgery for SEMS insertion because of neoadjuvant chemotherapy before the surgery.
SEMS insertion-related outcomes
Of the 27 patients undergoing preoperative stenting, technical success was achieved in 27 cases (100%). The clinical success was achieved in 26 cases (96.3%) because there was 1 patient who had reobstruction after placement, but was successfully restented. The complication cases relating to SEMS insertion was two (7.4%). Apart from the reobstruction case mentioned above, there was one incidence of abdominal pain after SEMS insertion, but only for observing and the patient did not need special handling. There were no other complications relating to SEMS insertion.
Perioperation period-related mortality and complication
The 30-day mortality rate for SEMS group and ES group was 0% and 3.0% (1 patients), respectively. The perioperation period-related complication for SEMS group and ES group was 7.4% (2 patients) and 21.2% (7 patients), respectively. In the SEMS group, 1 patient developed hypoalbuminemia, a second patient experienced wound infection. There were no other significant postoperative complications. In the ES group, 2 patients developed anastomotic leaks, three had wound infections, one experienced chest infection, and one developed pulmonary embolism. In addition, all these 7 patients in the ES group developed hypoalbuminemia.
Other operation-related statistics
The operation time of the SEMS group and the ES group was 117.22 ± 6.42 and 173.64 ± 8.32 minutes, respectively (P < .0001, Table 3). Significant differences were observed with regard to mean length of hospitalization in the two groups (8.81 ± 1.55 and 14.76 ± 4.37 days, respectively; P < .0001) (Table 3).
t-test.
ES, emergency surgery; SEMS, self-expanding metallic stents.
Postoperative follow-up monitoring
Mostly, follow-up visit was conducted with imaging study (CT, MRI, abdominal sonography, CEA, CA199, and PET-CT when necessary) and endoscopic study. Biopsies were taken to confirm the recurrence in case of positive finding of these studies.
Overall survival
During the follow-up, 14 (51.9%) patients in the SEMS group and 21 (63.3%) patients in the ES group died. Of the 35 patients who died, 25 (71.4%) died of cancer, and 10 (28.6%) died of accident, comorbidity, other diseases, or unknown causes. According to the OS rate, follow-up observation was continued for 3 years in 9 patients of SEMS group (33.3%) and 12 patients of ES group (36.4%), 4 subjects (14.8%) and 5 subjects (15.2%) for 5 years, respectively. The 3-year OS rate for ES group and SEMS group was 55.6% and 39.4%, respectively (P = .2119), and the 5-year OS rate for ES group and SEMS group was 48.1% and 36.4% (P = .3570). The Kaplan–Meier curve showed no difference in the OS between the two groups (log-rank test, P = .536; Fig. 1, Table 4). Significant factors independently predicting the OS are shown in Table 4 in bold.
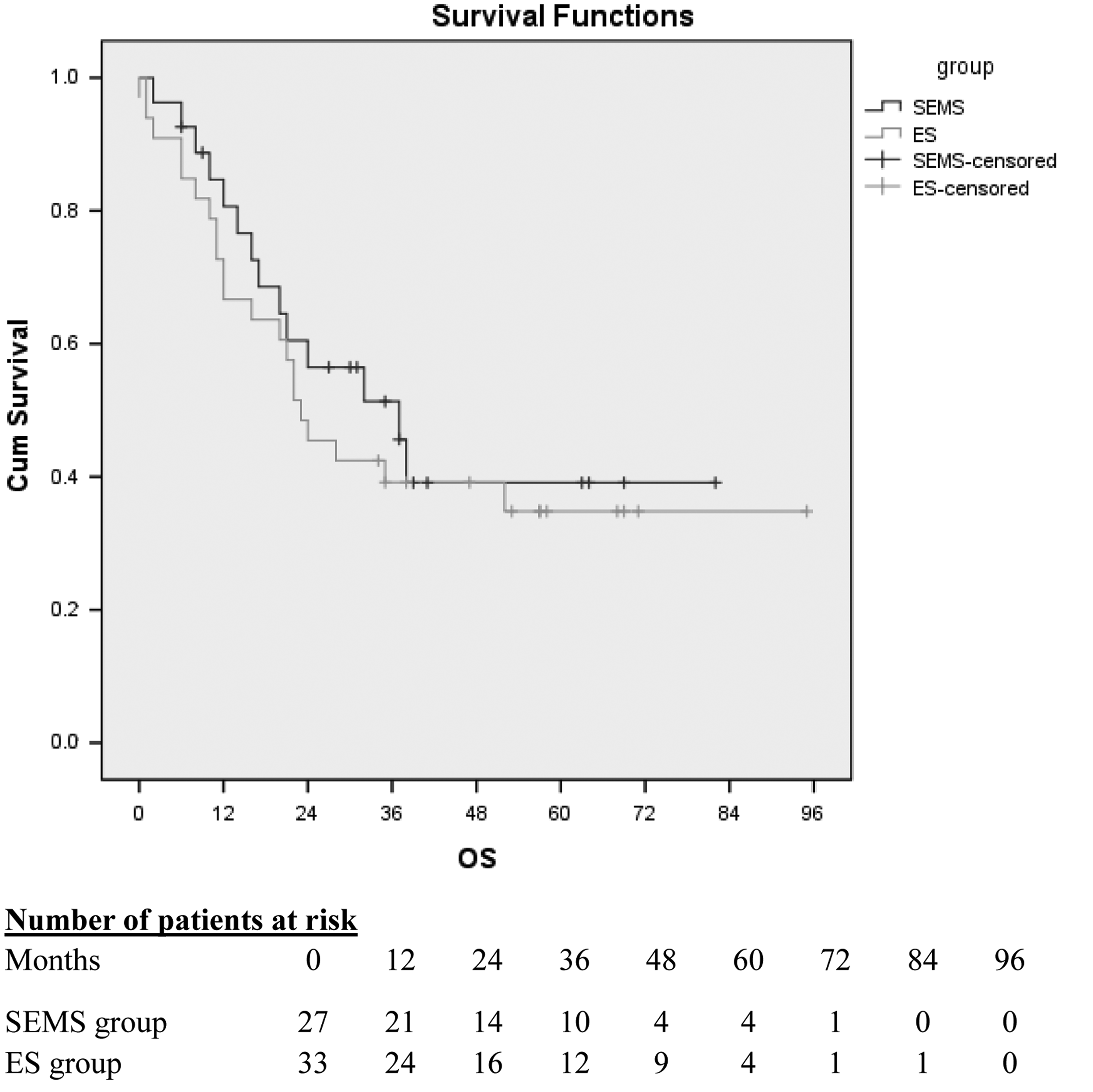
Kaplan–Meier curve of overall survival (OS) for the SEMS and ES groups. The 3-year OS rate for ES group and SEMS group was 55.6% versus 39.4%, P = .2119, and the 5-year OS rate for ES group and SEMS group was 48.1% versus 36.4%, P = .3570. The Kaplan–Meier curve showed no difference in the OS between the two groups (log-rank test, P = .536). Number of patients at risk is the number of individuals who are still alive at any time point and whose follow-up extends beyond the time in the curve. ES, emergency surgery; SEMS, self-expanding metallic stents.
Significant factors independently predicting the OS are shown in bold.
ES, emergency surgery; OS, overall survival; SEMS, self-expanding metallic stents.
Discussion
This study included a relatively large number of patients and provided a relatively long period of follow-up. The study found that SEMS insertion as a bridge to curative resection for MCO did not have unfavorable effects on long-term oncological outcomes.
It has been known that acute bowel obstruction occurs in 8%–29% of patients with primary CRC. CRC with MCO tends to occur at more advanced stages, with an increased risk of potential for local extension and distant metastasis than nonobstructive cancer. 6 Traditionally, patients with MCO have been managed by emergency surgical decompression on an unprepared bowel. However, as these patients were usually in poor general condition, emergency surgical intervention was associated with high mortality and morbidity. 25
Since 1991, when Dohmoto reported the first clinical experience of endoscopic stenting for rectal cancer as a palliative measure, there has been a heightened interest in the use of SEMS as an alternative to ES, particularly in patients with potentially curable CRC. 11 Through the use of SEMS as a bridge to elective surgical resection, perioperative morbidity and mortality, the rate of stoma formation, and the length of hospital stay were significantly reduced.26,27 In this study, the rate of stoma formation, which means the rate at the first surgery time for SEMS group, was obviously lower than that of ES group [7.4% (2/27) versus 45.5% (15/33), χ2 = 10.587, P = .001]. SEMS can decompress the obstructed bowel, provide an opportunity to clean the colon, allow physicians more time to perform a precise preoperative evaluation, and even make patients become candidates for laparoscopic resection. In this study, the laparoscopic surgery rate for SEMS group was 18.5% (5/27), without conversion to open, and 0% (0/33) for ES group. In contrast of those favored short-term outcomes, there was a concern for long-term oncological outcome of stenting, because of the manipulation of the tumor that may lead to the increased risk of tumor cell dissemination. 19 Kim et al. 28 showed that SEMS had a deleterious effect on the long-term outcome of colon cancer. However, in Kim's study, SEMS group enrolled patients who had left-sided CRC with obstruction, and the control group enrolled patients with nonobstructing left-sided CRC based on stage according to AJCC criteria in the ratio of 1:10. This discrepancy may be a possible selection bias, because the presence of MCO has been known as a poor prognostic factor. Zhang et al. 27 demonstrated that there was no difference between SEMS and ES groups. Gianotti et al. 29 even found the longer survival in the SEMS group (hazard ratio, 0.412; 95% CI, 0.217–0.785; P = .007) in a prospective study. Taking these discrepancies into consideration, the long-term oncological outcomes of colorectal SEMS for MCO have not yet been well established. There have been only a few studies on the long-term consequences of colonic SEMS as a bridge to curative surgery.
In our study, the long-term outcomes of SEMS as a bridge to surgery were comparable with those of ES. The 3-year OS rate for ES group and SEMS group were 55.6% and 39.4% (P = .2119), and the 5-year OS rate for ES group and SEMS group were 48.1% and 36.4% (P = .3570). The Kaplan–Meier curve showed no difference in the OS between the two groups (log-rank test, P = .536; Fig. 1, Table 4), even at advanced stages. Additionally, this study found that SEMS insertion was not an independent prognostic factor or OS (Tables 4 and 5).
OS, overall survival.
Bowel perforation is one of the related risks of potential tumor dissemination, but no stent-related perforation or microperforation or silent perforation cases occurred in this study.
There were some limitations in this study. First, this retrospective study is unable to fully evaluate possible confounders, such as the performance status and duration of symptoms at the time of initial diagnosis, owing to the retrospective nature of this study. Second limitation of this study was that further follow-up studies are required to more accurately define the long-term outcomes of SEMS, such as the complications related to the operation, not just the oncological outcomes.
In conclusion, the SEMS placement as a bridge to surgery is a feasible and effective intervention in the patients with MCO, and as the long-term oncological outcomes of SEMS were comparable to those of ES, SEMS should also provide patients with elective one-stage surgical resection while reducing stoma creation and postoperative complications. Certainly, it should be in the case of successful placement without perforation, when the procedure was conducted by an experienced endoscopist in a high-volume hospital. The oncological outcome of SEMS for MCO should be studied further in randomized controlled trials at high-volume centers or muticenters.
Footnotes
Acknowledgments
Changhai Hospital 1255 Project Fund (No. CH125542500). Key areas of Science and Technology Commission of Shanghai Basic Research Project (No. 13JC1407200).
Disclosure Statement
No competing financial interests exist.