
Abstract
Abstract
Objective:
Vesicoureteral reflux (VUR) is a common condition associated with childhood urinary tract infection (UTI), which may lead to chronic renal failure and hypertension. Different antireflux approaches were advocated with differences in morbidity and success. The aim of this study is to review and analyze the surgical outcomes of pneumovesicoscopic ureteral reimplantation and endoscopic injection of dextranomer/hyaluronic acid (Dx/HA) in three tertiary centers.
Materials and Methods:
The medical records of 215 patients (159 boys and 56 girls) for a total of 323 ureters underwent surgical interventions for primary VUR from February 2002 to August 2014 were reviewed. Data on baseline demographics, preoperative symptoms, radiological imaging studies, and postoperative outcomes were analyzed. VUR resolution was defined as when no VUR was detected by micturating cystourethrogram at 3 months or later after the intervention. Independent t-test, Mann–Whitney U test, Fisher's Exact test, and Chi-Square test were used for different parameters. All results with P value ≤.05 were regarded as statistically significant.
Results:
The mean age at operation was 3.33 and 4.63 for reimplantation and Dx/HA injection respectively. A total of 234 ureters underwent Dx/HA injection and 92 ureters underwent pneumovesicoscopic ureteral reimplantation with mean preoperative VUR grading of 3.1 and 4.2 respectively (P = .0001). The overall VUR downgrading and resolution rates were both significantly higher in reimplantation than Dx/HA injection (97.8% versus 78.6% P = .0001 and 84.3% versus 65% P = .0011). Further subgroup analyses across the different VUR gradings showed higher downgrading and resolution rates in reimplantation group than Dx/HA injection for grade 4 (100% versus 81% P = .0147 and 82.4% versus 63% P = .0411) and grade 5 VUR (97.3% versus 50% P = .0022 and 81.6% versus 40% P = .0256). Dx/HA injection was associated with shorter operation time (41.5 minutes versus 147.5 minutes, P < .001), less postoperative analgesic usage (P = .049), and shorter hospital stay (1.06 days versus 4.44 days P < .0001). No major complications were identified in both groups. The mean follow-up time was significantly longer in reimplantation group than Dx/HA group (57.25 months versus 37.85 months, P = .002). There was no significant difference in the rate of subsequent UTI development during follow-up (P = .8).
Conclusions:
Both Dx/HA injection and pneumovesicoscopic ureteral reimplantation are safe and effective treatments for VUR. Reimplantation is associated with significantly higher VUR downgrading and resolution rates than Dx/HA injection especially in the higher grade VUR while Dx/HA injection has significantly shorter operation time, lower postoperative analgesic usage, and shorter hospital stay. Dx/HA injection can be considered as the first line surgical treatment especially for lower grade VUR. Pneumovesicoscopic ureteral reimplantation can be used for higher grade reflux or those who failed Dx/HA treatments.
Introduction
V
Most VUR patients are managed conservatively or with prophylactic antibiotics.8,9 Surgical intervention is recommended in the presence of breakthrough UTI indicating treatment failure that raises the concern of renal injury. 10 There is no universal consensus in terms of the treatment for VUR or established gold standard for antireflux surgery. Both endoscopic injection of bulking agents (dextranomer/hyaluronic acid [Dx/HA]) and ureteral reimplantation were available with differences in morbidity and success.10–22 However, traditional open ureteral reimplantation is associated with significant morbidities and bladder dysfunction. Pneumovesicoscopic ureteral reimplantation was introduced, which showed comparable success rate with open approach but with lower morbidity.23–27 This study aimed to review and compare the surgical outcomes of pneumovesicoscopic ureteral reimplantation and endoscopic Deflux injection in three tertiary centers.
Materials and Methods
Medical records of children in two tertiary referral centers treated for primary VUR by endoscopic Dx/HA injection and pneumovesicoscopic ureteral reimplantation from April 2002 to February 2014 were reviewed after approval of research ethics committee. All data were collected from the electronic Patient Record system and the hardcopy records retrieved. Patients who had any previous treatment for VUR, a duplex kidney system, neurogenic bladder, severe voiding or bladder dysfunction (diagnosed by urodynamic studies), history of previous pelvic surgery, reimplantation or Dx/HA injection performed only as a part of the treatment for other renal tract abnormalities (e.g., ureterocele), and those with significantly incomplete records were excluded. Baseline demographics, radiological imaging studies (including renal ultrasonography, micturating cystourethrogram, and renal nuclear scans), preoperative, intraoperative, and postoperative outcome parameters were analyzed and compared. VUR resolution was defined as when no VUR was detected by micturating cystourethrogram at 3 months or later after the intervention.
Surgical procedures
The operative technique used for the pneumovesical ureteral reimplant group was Cohen cross-trigonal ureteral reimplantation with three 3–5 mm laparoscopic ports. The camera port was inserted under cystoscopic view and then CO2 pneumovesicum was created for the insertion of the other ports under laparoscopic view. Five millimeter 30° laparoscope and standard 3 mm laparoscopic instruments were used for the reimplantation procedure (Figs. 1–4).
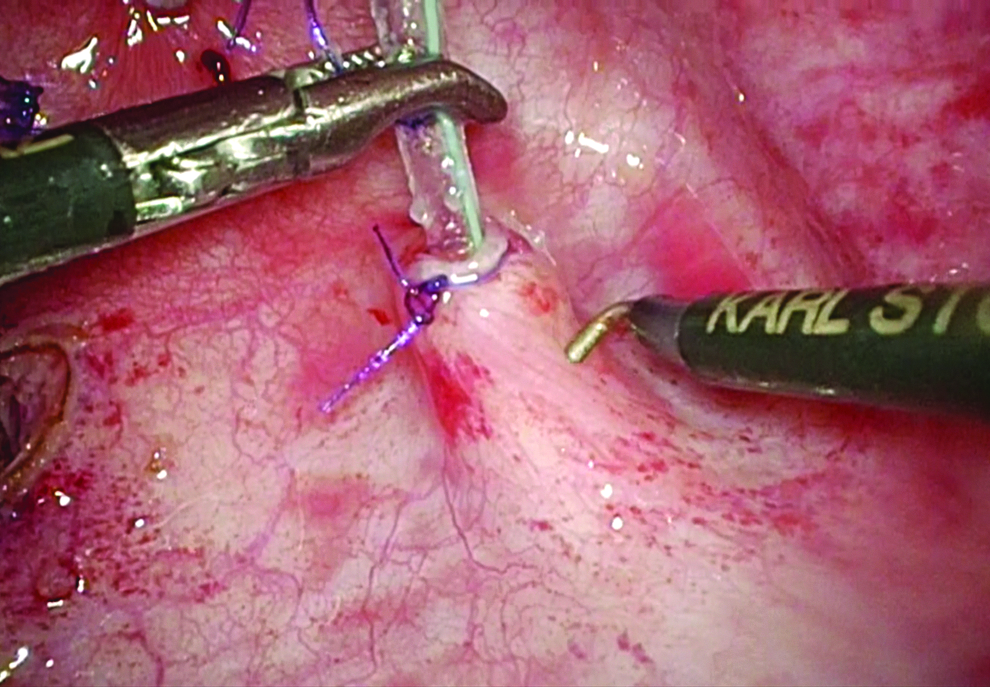
Mobilization of ureter.
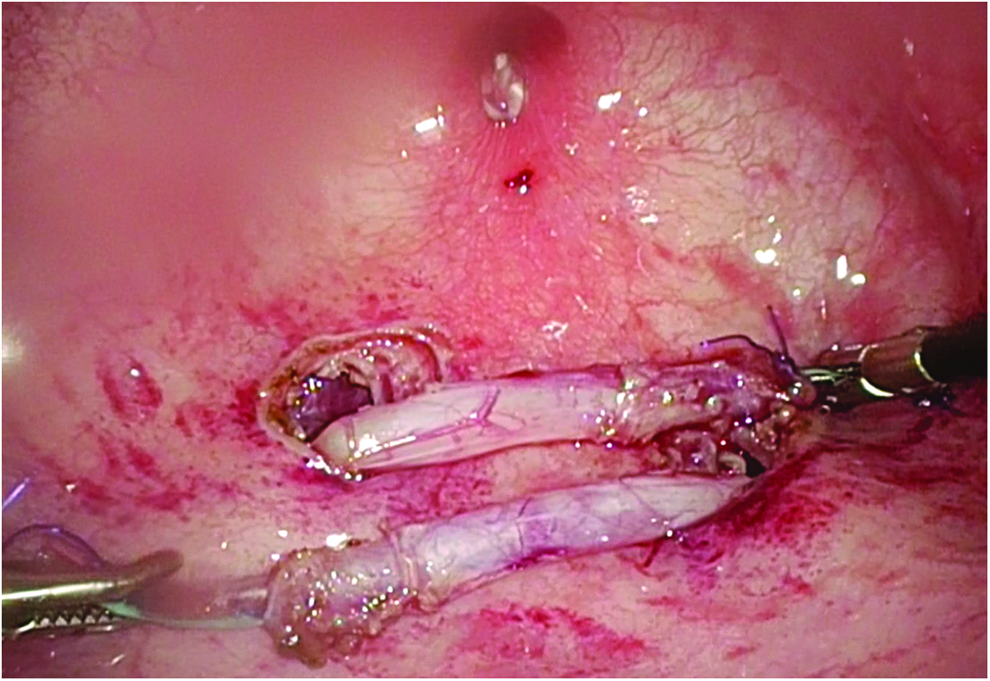
Mobilization of ureter till adequate length of four to five times ureteric diameter achieved.
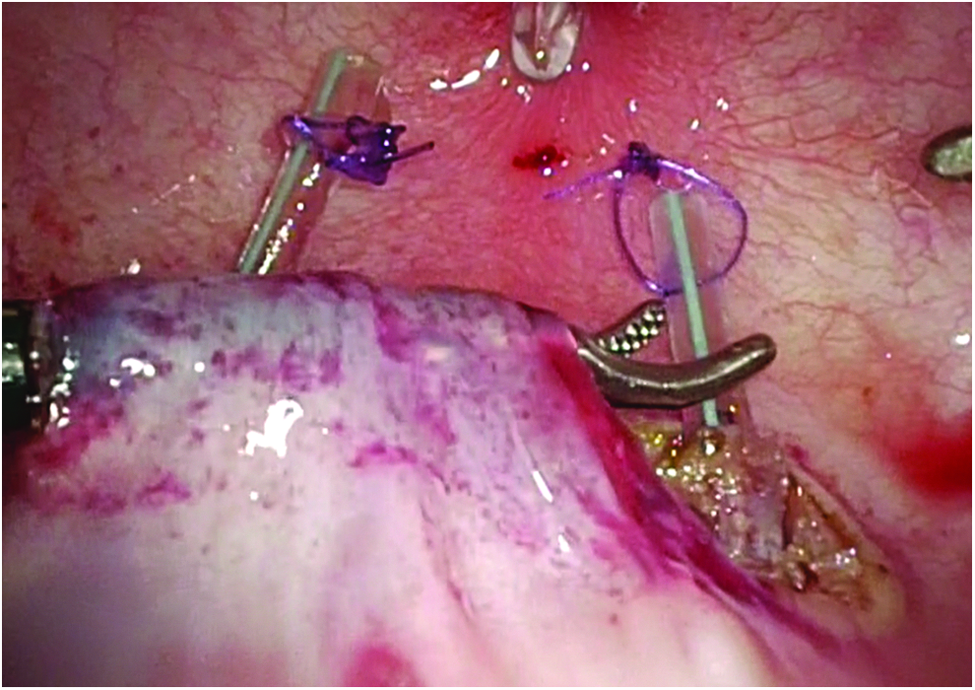
Submucosal tunnel created, ureter passed beneath the tunnel crossing the trigone.
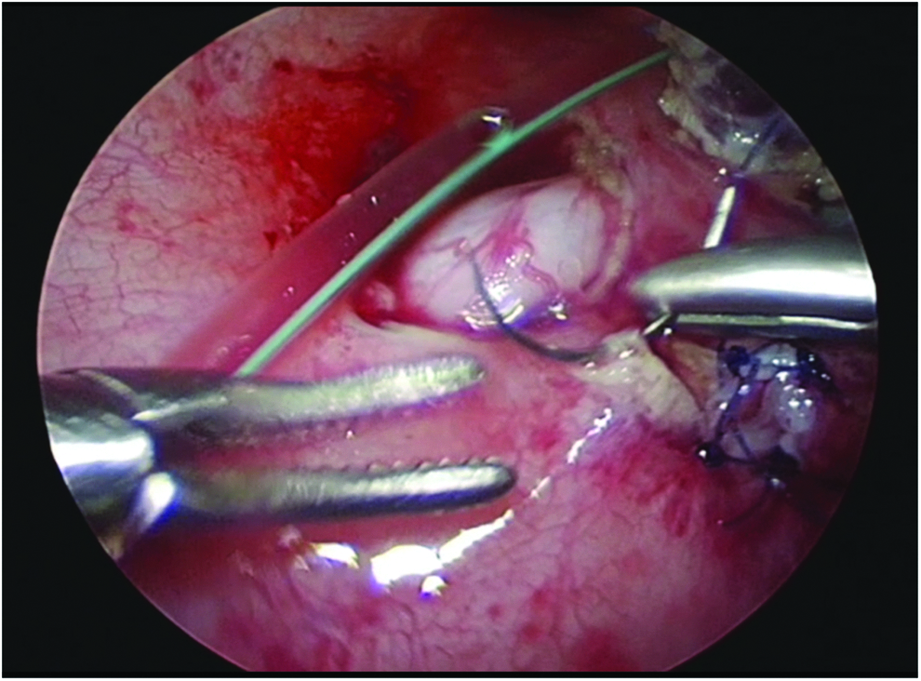
Most distal part of the ureter excised, opening spatulated and anastomosis done with absorbable sutures.
The operative techniques used for the Dx/HA injection were not standardized as limited by the retrospective nature of this study and incomplete data from part of the operative records. Different techniques were used including subureteric injection (STING), hydrodistention implantation technique (HIT), and proximal and distal intraluminal injections (Double HIT) techniques.
Statistical analysis
Data analyses were conducted using SPSS ver. 16.0. Ordinal variables were compared using Independent t-test and Mann–Whitney U test. Categorical nominal variables were compared with Fisher's Exact Test and Chi-square test as appropriate. Results with a two-sided P value of ≤.05 were regarded as statistically significant.
Results
Demographics
A total of 215 patients, including 159 boys and 56 girls (for total of 323 treated ureters) underwent surgery for VUR. There were 73 patients with unilateral VUR and 94 patients with bilateral VUR. Of all the 323 treated ureters, 234 ureters received Dx/HA injection and 89 ureters underwent pneumovesicoscopic ureteral reimplantation (5 patients with bilateral VUR received Dx/HA on 1 ureter and reimplantation on the other ureter) (Fig. 5).
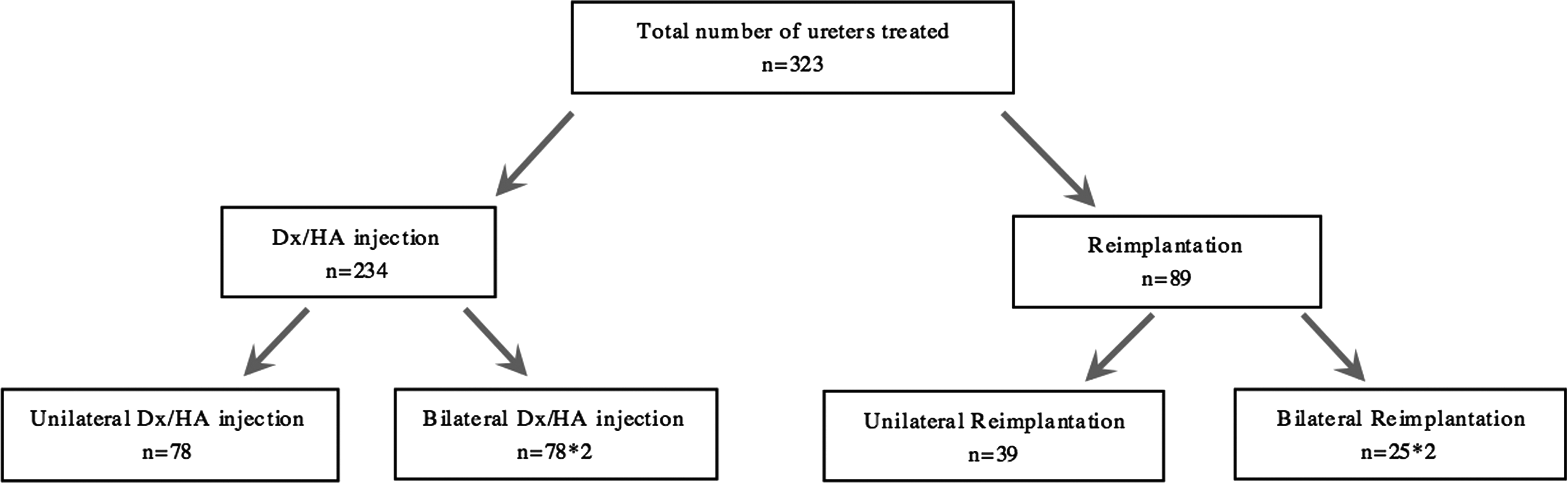
Treatment distribution. Dx/HA, dextranomer hyaluronic acid.
The mean age at presentation of VUR for Dx/HA and reimplantation group were 1.63 and 0.74 years respectively with significantly earlier presentation in reimplantation group (P = .033). There was significantly more antenatal hydronephrosis detected in the reimplantation than in Dx/HA group (15.7% versus 2.6% P = .0001). The mean age at operation was significantly younger in reimplantation group than Dx/HA group (3.33 versus 4.63 years old, P = .08). The VUR gradings are significantly higher in the reimplantation group that over 80% of the cases in the reimplantation group had grade 4 or 5 VUR while that for the Dx/HA group was only 40.2% (P < .0001). Significantly more renal scarrings were detected in the reimplantation than Dx/HA group (69.7% versus 53.8%, P = .017). The incidence of hydronephrosis was also significantly higher in the reimplantation group (36% versus 17.4%, P = .0009) (Table 1).
p < 0.05.
DMSA, dimercaptosuccinic-acid; USG, ultrasonography; UTI, urinary tract infection; VUR, vesicoureteral reflux.
Outcome analysis
The overall VUR downgrading rate was significantly higher in the reimplantation than Dx/HA group with one to three injections (97.8% versus 78.6% P = .004). The overall VUR resolution rate was also significantly higher in the reimplantation than Dx/HA injection (84.3% versus 65%, P = 0.0011). Significantly more VUR were downgraded to nondilating VUR (grading ≤2) in the reimplantation group (95.2% versus 72.7%, P = 0.0001). Subgroup analysis showed higher resolution and downgrading rate in all the VUR gradings in the reimplantation than Dx/HA injection, but the difference did not reach statistical significance except for the downgrading rate of grade 4 and grade 5 VUR (P < .05) (Table 2).
p < 0.05.
The intraoperative and postoperative parameters were summarized in Table 3. Dx/HA injection was associated with significantly shorter operation time than reimplantation (41.5 minutes versus 147.5 minutes P < .001). There was no conversion to open procedure in both groups. The percentage of boys who underwent concurrent circumcision in the reimplantation and Dx/HA group were 45.2% and 29.4% respectively (P = .29). For postoperative pain, there was significantly less analgesic usage in Dx/HA injection than reimplantation in terms of the total dosage of paracetamol used (18.4 versus 36.8 mg/kg, P = .049) and stronger analgesics (nonsteroidal anti-inflammatory drug and morphine) requirement (1.2% versus 24.6%, P = .001). No major complications were identified in both groups. Dx/HA group was also associated with shorter hospital stay than reimplantation (1.06 versus 4.44 days P < .0001). De novo contralateral VURs were found in 10.2% and 5.41% of the patients in Dx/HA and reimplantation group respectively (P = .323). There was no significant difference in the rate of subsequent UTI development between Dx/HA and reimplantation group during follow-up (6% versus 6.7%, P = .8).
p < 0.05.
NSAID, nonsteroidal anti-inflammatory drug.
Discussion
VUR is a common condition in children that may lead to chronic renal failure and hypertension. Many treatment options exist including conservative with observation, long-term antibiotics prophylaxis, and surgical interventions.10–22 Most VUR will resolve spontaneously as the child grows with the relative lengthening of the submucosal tunnel, however, the natural resolution rate for higher grade VUR is much lower.28,29 Prolonged antibiotics usage is associated with bacterial resistance with uncertain compliance rate. 30 Surgical intervention is recommended for patients with breakthrough UTI or progressive renal damage. 10
Traditionally, open ureteric reimplantation was once the most widely employed form of antireflux surgery. Common approaches include intravesical reimplantation such as technique described by Politano and Leadbetter in 1958, 17 cross-trigonal technique introduced by Cohen in 1975, 18 and extravesical reimplantation described by Lich and Gregoir in 1960s.19,20 Recent advances in laparoscopy marked the development of minimally invasive ureteral reimplantation. Laparoscopic extravesical ureteral reimplantation was introduced since 1990s with high successful rate.31–33 Pneumovesicoscopic ureteral reimplantation was introduced in 2005 with comparable success rate to open approach but associated with less postoperative morbidities.23–27 In recent years, robot-assisted laparoscopic ureteral reimplantation with extravesical and intravesical approaches were reported, the current literature on this is still limited but the preliminary results were encouraging.34–36
Apart from ureteral reimplantation, endoscopic procedure involving the injection of a biocompatible bulking material at the submucosa beneath the ureteric orifice under cystoscopy was introduced by O'Donnell and Puri. 11 Endoscopic injection gained its popularity due to the safety and efficacy reported although with variable results especially for higher grade VUR. Dextranomer/hyaluronic acid copolymer (Dx/HA) is one of the most commonly employed materials for endoscopic injection to correct VUR.11–16
There is no universal consensus in terms of the treatment for VUR or established gold standard for antireflux surgery. Different surgical approaches including reimplantation and endoscopic method are recommended as surgical treatment of choice with differences in success and morbidity. 10 The three study centers in our study provided both Dx/HA injection and pneumovesicoscopic ureteral reimplantation for patients with VUR indicated for surgical interventions and thus comparison of the outcomes of the two approaches could be done.
From the results of the patient demographics, there is likely selection bias in these two groups of patients for comparison limited by the retrospective quasi-experimental design of this study. The mean VUR grading is significantly higher in the reimplantation group than the Dx/HA group. Significantly more patients in the reimplantation group were associated with antenatal hydronephrosis, earlier presentation, and renal scarrings. This could be explained by the fact that more patients with lower grades VUR were offered Dx/HA and those with more severe VUR were offered reimplantation as the treatment of choice.
Despite the selection bias that more severe VUR were in the reimplantation group, the overall VUR downgrading and resolution rates were both significantly higher in reimplantation than Dx/HA injection (97.8% versus 78.6% P = .0001 and 84.3% versus 65% P = .05). If treatment success was defined as downgrading VUR to nondilating VUR (i.e., VUR grading ≤2), the success rate is significantly higher in the reimplantation than Dx/HA injection (95.2% versus 72.7%, P = .0001). Further subgroup analyses across the different VUR grades also showed significantly higher downgrading and resolution rates in reimplantation group than Dx/HA injection in grade 4 and grade 5 VUR. The downgrading and resolution rates were also higher in reimplantation group than Dx/HA group for the lower grade VUR (grade 1–3) but not reaching statistical significance. No conversion or major complication was observed in either group, which suggested both procedures are safe to perform. Although Dx/HA treatment was associated with less postoperative pain and shorter hospital stay, the success rates are lower especially in the higher grade VUR.
Conclusion
Both Dx/HA injection and pneumovesicoscopic ureteral reimplantation are safe and effective treatments for VUR. Pneumovesicoscopic ureteral reimplantation is associated with significantly higher VUR downgrading and resolution rates than Dx/HA injection especially in the higher grade VUR while Dx/HA injection has significantly shorter operation time, lower postoperative analgesic usage, and shorter hospital stay. Further prospective studies are required to validate the results.
Footnotes
Disclosure Statement
No competing financial interests exist.