
Abstract
Abstract
Background:
Laparoscopic-assisted endorectal pull-through (LAEPT) procedure in the management of high-type anorectal malformations (ARMs) was first introduced in 1998 and is quickly accepted worldwide. However, evidence on long-term outcomes of this technique is constrained. This study aims to evaluate the long-term outcomes of LAEPT for high-type ARMs in Vietnamese pediatrics.
Materials and Methods:
A longitudinal study was carried out from January 2009 to July 2014 in 56 patients <3 years old. Variables included age of operation, associated anomalies, type of fistula, the duration of hospital stay, complications, and long-term functional outcomes (Krickenbeck modified standards were used for children ≥3 years).
Results:
There were 56 patients including 48 males and 8 females. The mean age at operation was 3.7 months, the mean hospital stay was 4.6 days. The mean operative time was 76.7 minutes. The mean follow-up time was from 38 to 104 months (mean follow-up: 71.5 months). There were 46 (82.1%) patients having feeling of urge, 42 (75.0%) patients having capacity to verbalize, and 40 (71.4%) patients having hold the bowel movement.
Conclusion:
LAEPT is feasible, safe, and effective in the management of high-type ARMs.
Introduction
The incidence of anorectal malformations (ARMs) ranges from 1 in 4000 to 1 in 5000 live births.1,2 Laparoscopic-assisted anorectal pull-through (LAARP) procedure was first reported by Willital in 1998, 3 and then developed by Georgeson in 2000 for ARM. 4 This approach has been accepted widely at the global pediatric surgical centers.5–7 Most of the studies reported good early postoperative outcomes; however, there is a lack of evidence about effects of this procedure in long-term outcomes. Therefore, the aim of this study is to evaluate the long-term outcomes of the LAARP procedure for children with high type of ARMs.
Materials and Methods
From January 2009 to June 2014, we conducted a cohort study at the General Surgery Department, National Children's Hospital (Hanoi, Vietnam).
Patients were children suffering high type of ARMs undergoing the LAARP procedure. All patients with high imperforate anus underwent colostomy at the left colon in the newborn period. Subsequent LAARP procedure was performed at the second stage after 1–3 months when the colostomy was closured.
Surgical technique
After general endotracheal anesthesia, a urinary catheter was inserted into the bladder and the patients were placed in Trendelenburg position at the middle of the operating table. The technique of the LAARP procedure has been described elsewhere. 3 The operation was performed using three trocars: (1) a 5-mm umbilical trocar was inserted as the scope; (2) two additional 5-mm trocars were inserted as working ports with one as the right anterior axillary line and one as the left anterior axillary line under the umbilicus 2 cm (Fig. 1). The abdomen was insufflated with CO2 to ensure pressure of 8–10 mmHg.
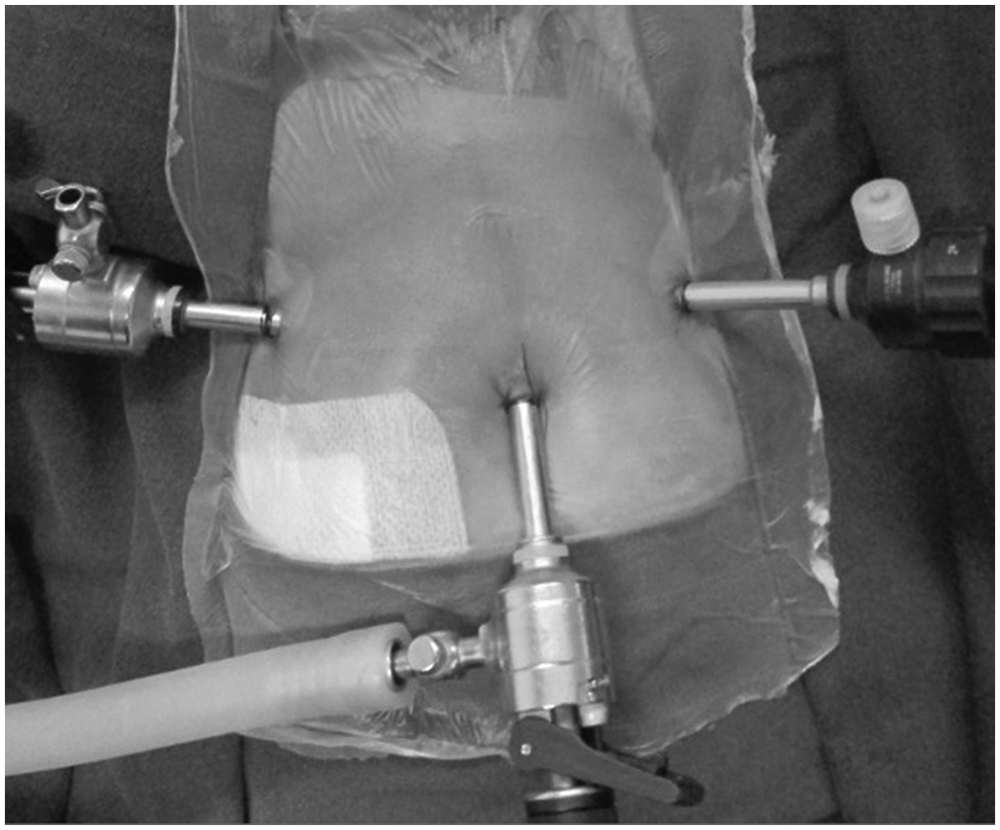
Trocar placement.
The rectal was dissected using a hook cautery to create a window through the rectal mesentery, then continued circumferentially around the rectal pouch down to the fistula urethra. Stay sutures were placed to pull forward the peritoneal reflection and the bladder (Fig. 2). The fistula was exposed, divided, and then was closed by two sutures.
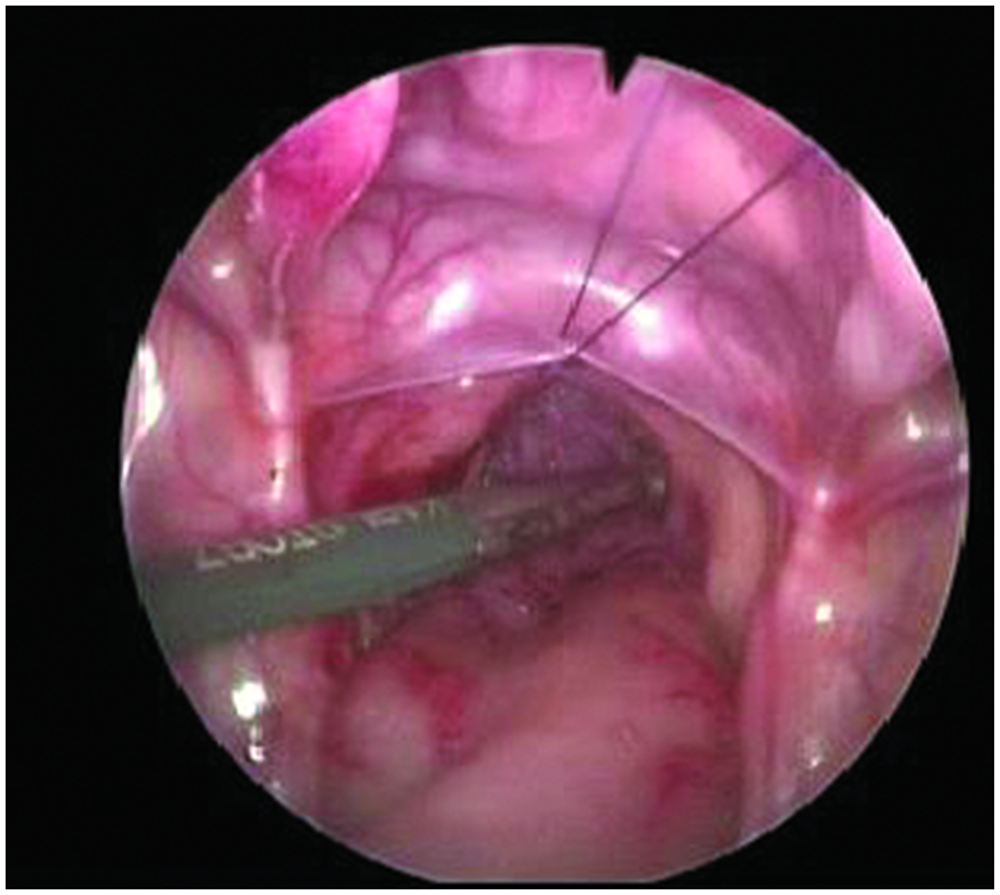
Stay suture to pull forward the peritoneal reflection and the bladder.
The center of the external sphincter complex was identified using an electrical muscle stimulator on the perineum. A cruciate skin incision was made through this point (Fig. 3). The skin and subcutaneous tissues were dissected to expose the external sphincter as much as possible (Fig. 4). A tunnel through the center of external sphincter and between two elevators and the electrical stimulator on the external sphincter was again used to identify the center. A mosquito forceps was advanced through the center of the external sphincter complex under the guidance of a laparoscope in the pelvic floor. Dilative channel was gradually enlarged using an anal dilator up to the size of 12-mm to help the dilator to pass easily. The rectum was pulled through the tunnel and anoplasty was performed by suturing the rectum to the external sphincter and then to the skin. Anal dilation was started 2 weeks after the operation and prolonged until closure colostomy. Colostomy was closed from 1 to 3 months after the rectal LAARP.

Wide cross-perineal skin incision.

The external sphincter was widely exposed.
Variables
We collected variables including age of operation, associated anomalies, type of fistula, duration of hospital stay, complications, and long-term functional outcomes (Krickenbeck modified standards was used for children ≥3 years).
Results
In the study period, 56 children with high type of ARMs including 48 boys and 8 girls were operated. The mean age of patients at LAARP was 3.7 ± 1.1 months (range: 3–9 months). Patients' weight varied from 4.0 to 9.0 kg (mean: 6.2 ± 1.0 kg). The types of ARMs according to Krickenbeck classification are presented in Table 1.
Type of Anorectal Malformation and Bowel Movement
Associated anomalies included Down syndrome, 5 cases; vesicoureteral reflux, 5 cases; ventricular septal defect or atrial septal defect, 4 cases; esophageal atresia, 1 case; single kidney, 4 cases; sacral anomalies, 8 cases; meningocele, 3 cases; tethered cord, 2 cases; congenital arthrosis, 1 case.
Simultaneous colostomy closure was performed in 3 patients due to tension during the rectal pull through. The colostomy was performed in all patients. No patient had conversion. Perforation of the vagina happened in 1 patient, which was detected and closed successfully without postoperative complication. Operative time varied from 45 to 120 minutes (mean: 76.7 ± 19.3 minutes). The average length of hospital stay in 56 patients was from 2 to 7 days (mean 4.6 ± 1.5 days). Postoperative complications including dehiscence of anocutaneous anastomosis were found in 2 patients. They were healed after that.
Follow-up
Among 56 patients, all children were ≥3 years old. The duration of follow-up was from 38 to 104 months (mean: 71.5 ± 15.5 months). Spontaneous defecation occurred in 53 patients (94.6%). Three patients suffered from constipation, and 4 patients had anal stenosis who required Y-V plasty. Twelve patients (21.4%) suffered from grade 1 or grade 2 soiling. Voluntary bowel movement was seen in 46 patients. The results are presented in Table 1.
Rectal mucosal prolapse occurred in 9 patients (16.1%), who required a second operation. All patients urinated spontaneously. No urethral fistula or diverticulum was detected. Voiding cystourethrography was performed in 48 male patients.
Discussion
It has been nearly 20 years since LAARP was first introduced. 3 However, this approach has not become a routine application in the management of ARMs. Several concerns were raised, especially difficulties in the separation of the rectal pouch from the urethra and the management of rectourethral fistula. 8 This study is one of the studies with the highest sample size using LAARP in ARMs. Our results showed no conversion to open surgery due to difficulties in performing laparoscopic operation as well as no mortality and low perioperative complications. These results suggest the feasibility and safety of the laparoscopic approach. Ming et al. showed that the overall morbidity rate of LAARP was lower than that in posterior sagittal anorectoplasty (12.5% versus 35.3%). 9
The operative time was relatively short (median: 76.7 minutes), which is consistent with a mean operative time for LAARP of 112.5 ± 12 minutes versus 120.4 ± 18.5 minutes for PSARP in Tong et al.'s study and 1.62 ± 0.4 hours for LAARP versus 2.13 ± 0.30 hours for PSARP in Ming et al.'s study.9,10
Although rectovesical fistula is easily divided and closed laparoscopically, management of fistula between the rectal pouch and the urethra is the most difficult step in the laparoscopic approach with a high risk of injury of the urethra, urethral diverticulum, or recurrence of the fistula.11–14 Alternative techniques have been proposed to facilitate the management of rectourethral fistula. Rollins reported a simple sharp division of the rectourethral fistula without clip or suture ligature for 5 patients. The duration of Foley catheter was long, ranging from 6 to 40 days. One patient developed a posterior urethral diverticulum. 15 Srimurthy performed a subseromuscular dissection of the distal rectum to create a mucosal tube. This tube was then ligated and closed. 16 Yamataka inserted a fine flexible endoscope into the rectum through an opening made in the anterior rectal wall. He stated that endoscopy of the rectum allowed the exact excision of the rectobulbar fistula. 17 Koga carried out intraoperative measurement of rectourethral fistula by combining laparoscopy and cystoscopy before dissecting it free from the prostate and divided for 5 patients without residual fistula. 18
With our technique, it is feasible for laparoscopic identification of the levator complex and accurate placement of rectal pouch within the center of the complex. Furthermore, the large cruciate skin incision on the perineum allows good exposure and direct visualization of the external sphincter. The external sphincter center can be easily identified using the muscle stimulator to facilitate precise positioning of the rectal pouch. These factors may lead to our good results in postoperative fecal continence.
The rate of postoperative rectal mucosal prolapse in our study was high at 16.1%. This figure is consistent with other reports.19,20 The dissection and mobilization of the upper rectal pouch should be limited to reduce this complication.
In summary, our experience of the LAARP technique in 56 patients with high type of ARMs showed that this approach is feasible, safe, with low complications, and good early outcomes. However, longer follow-up is necessary for more definitive conclusion on the outcome.
Footnotes
Acknowledgment
The author is grateful and expresses his thanks to Dr. Toshihiko Watanabe, National Center for Child Health and Development, Division of Surgery (Japan) for giving his advice and time to edit the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.