
Abstract
Abstract
Introduction:
Sacrococcygeal teratoma (SCT) is the most common teratoma presenting at birth. Life-threatening bleeding is a major complication during tumor excision in children. In this study we demonstrate our technique for laparoscopic division of median sacral artery (MSA) during dissection of SCT in 2 pediatric patients as a safe technique to minimize risk of hemorrhage.
Methods:
Two female infants diagnosed with types III and IV SCTs underwent preoperative evaluation in the postnatal period. The first patient was an 18-month-old girl who presented with metastatic type IV teratoma, resected after neoadjuvant therapy, and the second patient was a 6-day-old girl with prenatal diagnosis of cystic type III teratoma. Using laparoscopy in both patients, the presacral space was reached by opening the peritoneal reflection with blunt dissection and the MSA was identified. Then it was carefully isolated and divided with 3 or 5 mm sealing device. The pelvic components of the tumors were partially dissected using laparoscopy. The first patient's tumor resection was completed using a posterior sagittal approach and the second patient required a standard Chevron incision. Along with the description of our technique, a review of the current literature for the management of SCT and MSA was performed.
Results:
Both patients underwent successful laparoscopic division of the MSA and resection of the SCTs without complications.
Conclusion:
Laparoscopic MSA division before SCT excision offers a safe approach that can reduce the risk of hemorrhage during surgery.
Introduction
S
One of the most serious complications of SCTs is life-threatening hemorrhage.5,12 Hemorrhage can occur in utero, perioperative period, and can occasionally occur during the surgical excision of the tumor. 12
To prevent tumor hemorrhage, several surgical techniques have been investigated. Clamping of the abdominal aorta above the bifurcation with an open surgery approach has been shown to be successful in reducing the risk of hemorrhage. 13 Most recently, with advances in minimal invasive surgery, laparoscopic techniques have shown excellent results for patients with type I tumors.5,14,15 Laparoscopic isolation followed by ligation or clipping of the MSA before tumor resection can prevent bleeding.5,12,16
We present 2 cases of laparoscopic division of the MSA and laparoscopic-assisted dissection of the pelvic SCT component in 2 pediatric patients with types III and IV SCTs as a safe method of minimizing hemorrhagic risk.
Case 1: Altman Type IV SCT
A 15-month-old previously healthy girl delivered at full term by normal spontaneous vaginal delivery presented to an outside hospital with bruising of the left buttock after a fall at daycare, as well as 1 month history of constipation. She was worked up for nonaccidental trauma, and a computed tomography scan revealed a large pelvic mass with suspicious metastatic nodules. She was then transferred to our hospital where magnetic resonance imaging (MRI) confirmed a large pelvic mass arising from the coccyx, measuring 6.2 × 5.8 × 9.5 cm with partial rectal obstruction (Fig. 1A). Further metastatic workup showed bilateral pulmonary nodules and numerous enhancing hepatic lesions. These findings and elevation of alpha fetoprotein (AFP) >60,000 supported the most likely diagnosis of Altman type IV SCT with pulmonary and hepatic metastasis.

MRI in sagittal and coronal views showing large SCT (red arrows) displacing the rectum anteriorly
She was taken to the operating room for laparoscopic liver biopsy, port placement, and diverting loop colostomy for impending bowel obstruction. A large pelvic mass was appreciated without any evidence of peritoneal metastases. The uterus and bladder were superiorly displaced by the mass. Pathology results were consistent with a malignant yolk sac tumor. Given the large size of the tumor, it was deemed unresectable and the patient was started on neoadjuvant chemotherapy.
After 6 cycles of chemotherapy, the primary mass and metastatic lesions had significantly decreased in size and the course of the MSA was identified with axial imaging (Fig. 1C, D). AFP had trended downward appropriately and was within the normal range at 7.9. On examination, the patient's abdomen was soft without palpable masses, the colostomy was functional, and the perianal bruising had resolved.
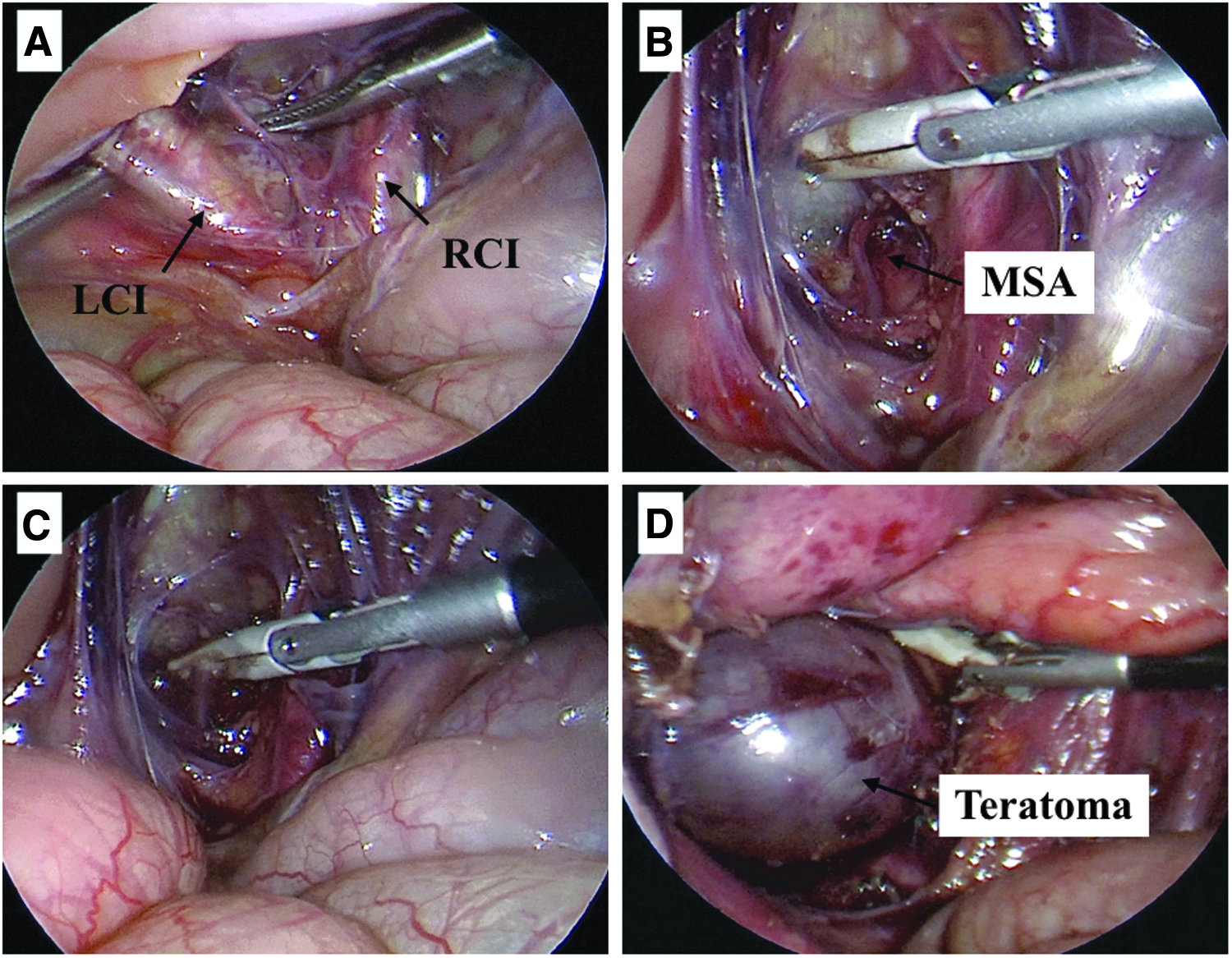
At 18 months of age, she underwent a diagnostic laparoscopy with laparoscopic division of the MSA followed by dissection of the pelvic tumor component and complete resection of the SCT. The abdomen was accessed with a 5 mm umbilical port and two other 5 mm ports were placed as working instruments. The uterus was lifted away from the pelvis using a percutaneous suture. With gentle blunt dissection, the presacral space was opened left lateral to the rectosigmoid mesocolon. The dissection was carried away from mesenteric vessels, ureters, and iliac vessels, which were under constant direct vision (Fig. 2A–C). The MSA was noted along the anterior surface of the sacrum and the vessel was isolated and taken proximally and distally with 5 mm LigaSure™ (Medtronic, Minneapolis, MN) while ensuring hemostasis. The pelvic components of the tumor were dissected using laparoscopy (Fig. 2D), and then the tumor resection with a complete coccygectomy was performed using a posterior sagittal approach. The diverting colostomy was left in place.

Intraoperative exposure of the MSA within the pelvis laparoscopically.
The patient was discharged home on postoperative day 2 with no immediate postoperative complications. Review of pathology confirmed that the entire tumor was removed with negative margins. Repeat MRI showed no evidence of recurrence and resolution of metastatic nodules. Her AFP levels have remained within normal limits since surgery and her colostomy was taken down 3 months after surgery.
Case 2: Altman Type III SCT
A newborn girl delivered preterm (GA 35w2 d) through spontaneous vaginal delivery was transferred from an outside hospital for management of a prenatally diagnosed sacral lesion. Prenatal MRI showed a multicystic mass in the presacral space with both internal and external components, most consistent with an SCT. She was followed up with serial ultrasonography until the date of delivery. There were no intrauterine complications, such as hydrops or cardiac decompensation.
On examination at our hospital, there was a 10 × 7 × 3 cm dark blue sacral mass that was completely covered by skin. MRI at 2 days of life showed a 3.3 × 5.1 × 8.1 cm predominantly cystic and septated abdominoperineal mass with small solid components and a small external component. These findings supported the diagnosis of Altman type III SCT amenable to surgical resection.
At 6 days of age, the patient was taken to the operating room for diagnostic laparoscopy, laparoscopic division of the MSA, partial dissection of the pelvic portion of the mass, and complete resection through a Chevron incision. The abdomen was accessed with a 3 mm umbilical port and three other 3 mm ports were placed as working instruments. The uterus was lifted away from the pelvis using a grasper. With gentle blunt dissection, the presacral space was opened left lateral to the rectosigmoid mesocolon. The dissection was carried away from mesenteric vessels and between the ureters and common iliac vessels, which were always under direct vision (Fig. 2A, B). The MSA was noted along the anterior surface of the sacrum and the vessel was isolated and taken proximally and distally with 3 mm JustRight™ Vessel Sealing System (JustRight Surgical LLC, Boulder, CO) while ensuring hemostasis. The pelvic components of the tumor were dissected using laparoscopy (Fig. 2D) and the remainder of the tumor resection with a complete coccygectomy was completed using a standard Chevron incision. A 7 Fr Jackson Pratt (JP) drain was placed within the remaining cavity.
There were no immediate postoperative complications; her JP drain was removed on postoperative day 6 and she was discharged on postoperative day 7. Final pathology of the mass showed a mature cystic teratoma. At 1 month follow-up, AFP was >8000, which was within normal limits using a gestational age-based nomogram (Figs. 3 and 4).
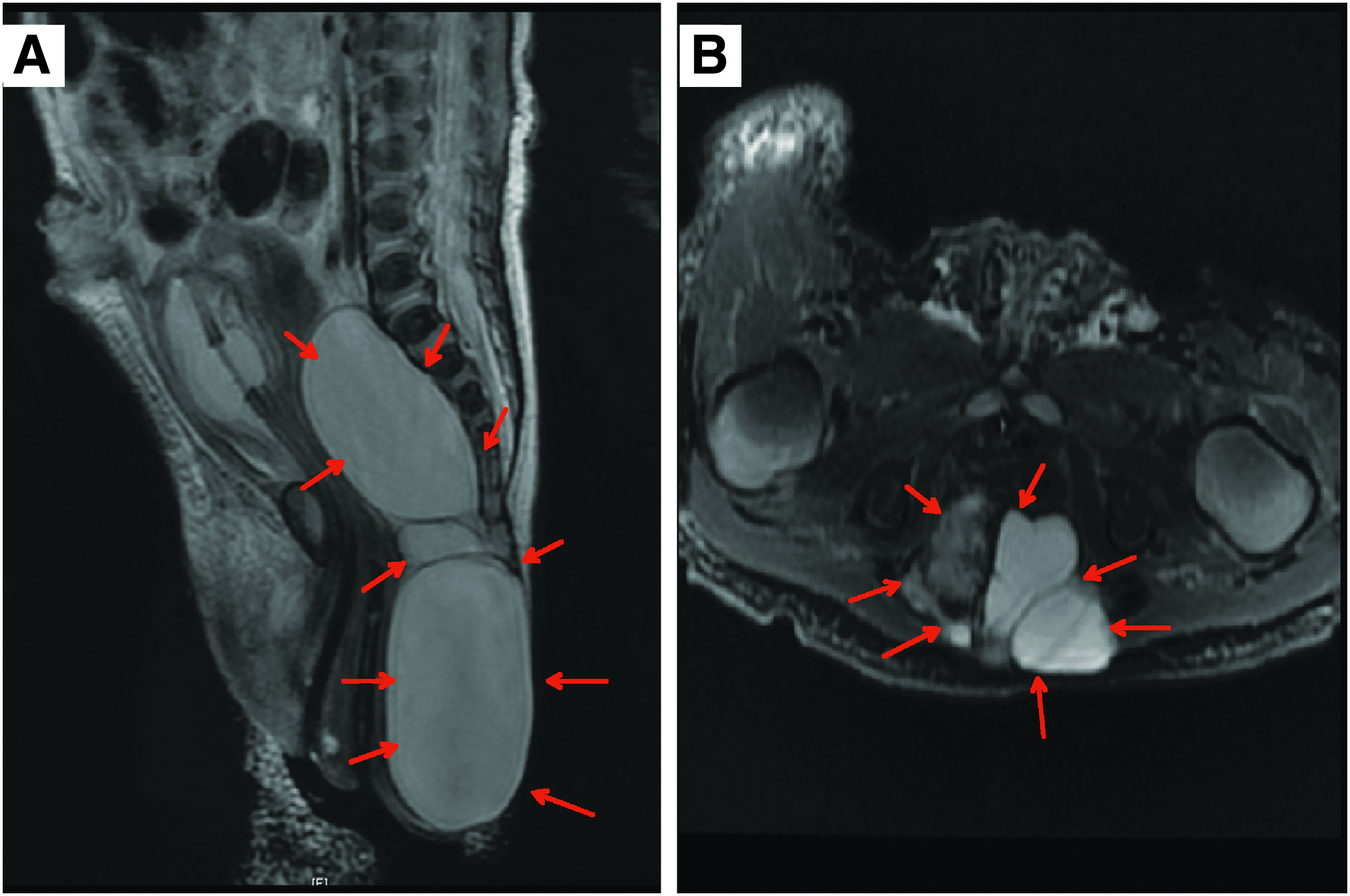
MRI in sagittal
The LCI and the RCI are clearly identified and seen bifurcating
Discussion
One of the most common serious and potentially lethal complications of resection of SCTs is life-threatening hemorrhage.5,12 As such, vascular control is of utmost importance in the surgical management of SCTs.5,13–15
In this report we demonstrate the safety and efficacy of laparoscopic division of the MSA and intrapelvic tumor dissection in both a neonate and a toddler with an Altman type III and IV tumors, respectively. As surgical tools are refined and downsized to be safely used in smaller and smaller patients, we will see an improvement in surgical techniques for even infants with large type I tumors. In our case, we were able to show the safety of 3 and 5 mm sealing devices to control the MSA without the need for clips or sutures. See Table 1 for a summary of the current literature.
CT, computed tomography; MRI, magnetic resonance imaging; MSA, median sacral artery; SCT, sacrococcygeal teratoma; US, ultrasound.
Conclusion
The 2 cases demonstrated that laparoscopic MSA division with vessel sealing devices is a safe and innovative approach to prevent exsanguinating hemorrhage during SCT resection in select cases.
Footnotes
Disclosure Statement
The authors of this article have nothing to disclose.