
Abstract
Abstract
Introduction:
The optimal approach of resection for mid–low rectal cancer after neoadjuvant chemoradiotherapy (nCRT) is still controversial. The aim of this meta-analysis was to clarify the safety and feasibility of laparoscopic surgery compared with open resection.
Materials and Methods:
We performed a literature search for studies on PubMed, Embase and Cochrane Library up to March 1, 2018. Review Manager software was applied for data analysis. We used weighted mean difference (WMD) for continuous parameters and odds ratio (OR) for dichotomous variables. Confidence interval (CI) was set at 95% and a P value <.05 was considered statistically significant.
Results:
A total of seven studies met the inclusion criteria for the meta-analysis: 466 patients in laparoscopic group and 491 in open group. The pooled result revealed that laparoscopic resection had a favorable blood loss (WMD = −116.88 mL; 95% CI: −189.78 to −43.99; P = .002), analogous lymph nodes harvest (WMD = −0.30; 95% CI: −1.29 to 0.70; P = .56), less postoperative complications (OR = 0.63; 95% CI: 0.46–0.88; P = .006), shorter time to pass first flatus (WMD = −0.76 day; 95% CI: −1.00 to −0.51; P < .00001), and stay in hospital (WMD = −2.71 days; 95% CI: −4.54 to −0.88; P = .004), despite similar operating time (WMD = 11.17 minutes; 95% CI: −14.37 to 36.70; P = .39).
Conclusions:
Laparoscopic resection might be a technically safe and feasible approach for mid–low rectal cancer patients after nCRT compared with open resection.
Introduction
C
nCRT can reduce tumor body and decrease tumor stage, some tumors even achieve complete remission, and radical resection rate is improved. 10 It was reported that anal preservation rate was enhanced and local recurrence was less in locally advanced rectal cancer after nCRT. 11 Although reduced tumor size creates more maneuvering room in pelvis, tissue edema and fibrosis caused by chemoradiotherapy result in so much exudation that it is hard to identify correct anatomical layer. 12 The difficulty of laparoscopic radical resection is evidently increased.
In our meta-analysis, we collected data from previous studies to compare laparoscopic resection and open resection after nCRT concerning intraoperative and postoperative outcomes for mid–low rectal cancer patients with the aim of selecting appropriate surgical techniques.
Materials and Methods
Data search and study selection
We performed a literature search to conduct the meta-analysis for studies that addressed the safety and feasibility of laparoscopic resection following nCRT for mid–low rectal cancer patients up to 01 March 2018. The primary searched sources were PubMed, Embase, and Cochrane Library. Database-specific search terms of laparoscopic resection and open resection were combined with truncated search terms using the wildcard (“*”) character for rectal cancer patients after nCRT to ensure the integrity of search results. We also used “related articles” function and manual searches for reference lists to broaden the search.
Two reviewers (L.P. and Y.M.) independently retrieved and checked the literature and determined whether to include each study. Disagreement between them was resolved by discussion or third-party arbitration. The two reviewers evaluated the remaining full articles to ensure that they satisfied the inclusion criteria. Only the most recent and complete data were included if the results of a single study were reported in more than one publication.
The inclusion criteria of studies were as follows: (i) they evaluated efficacy of laparoscopic resection following nCRT in mid–low rectal cancer patients; (ii) they were randomized controlled trials (RCTs) or non-RCTs; (iii) rectal cancers were located 10 cm or less from the anal verge; and (4) they reported at least one primary outcome.
Studies were excluded if (i) the patients had rectal cancers that were located over 10 cm from the anal verge; (ii) they lacked the control group or control group was unreasonable; and (iii) they were case reports, reviews, or letters.
Quality assessment of included studies
The quality of RCT was evaluated using Cochrane collaboration's tool for assessing risk of bias. 13 The quality of non-RCT was evaluated using the Newcastle–Ottawa Scale (NOS). 14 RCT had a moderate risk of bias or non-RCT had a NOS score >5, which was normally considered as a high-quality study.
Data extraction
Two reviewers (Y.L. and L.R.) independently assessed studies for inclusion based on the criteria described previously. Discrepancies between the two reviewers were resolved by discussion or third-party arbitration. The following information was extracted: first author's family name, publication period, region, study design, total number of patients in laparoscopic and open resection group, and outcomes.
Statistical analysis
Statistical analysis was performed using Review Manager Version 5.3 software (The Cochrane Collaboration, Oxford, England). Weighted mean difference (WMD) was used for continuous parameters. Odds ratio (OR) was used to analyze the dichotomous variables. Confidence interval (CI) was set at 95% and a P value <.05 was considered statistically significant. Median and range data were converted into mean and standard deviation using the method described by Hozo et al. 15 Heterogeneity among studies was quantified using the I2 statistics and Q test. A value of I2 > 50% was defined as high heterogeneity. The values of <25% and between 25% and 50% were respectively defined as low and moderate heterogeneity. 13 A fixed effects model was used for low and moderate heterogeneity, and a random effects model was used for high heterogeneity.
Results
Study eligibility
The primary search strategy retrieved 513 relevant publications in PubMed, Embase, and Cochrane Library (Fig. 1). After browsing titles and abstract, 490 articles, which were duplicate records or obviously did not meet the inclusion criteria, were excluded. The 16 remaining studies that did not conform to our research theme (rectal cancers were located over 10 cm from the anal verge), and other criteria were excluded after we reviewed the full texts. Finally, seven accessible studies were selected for further meta-analysis.16–22
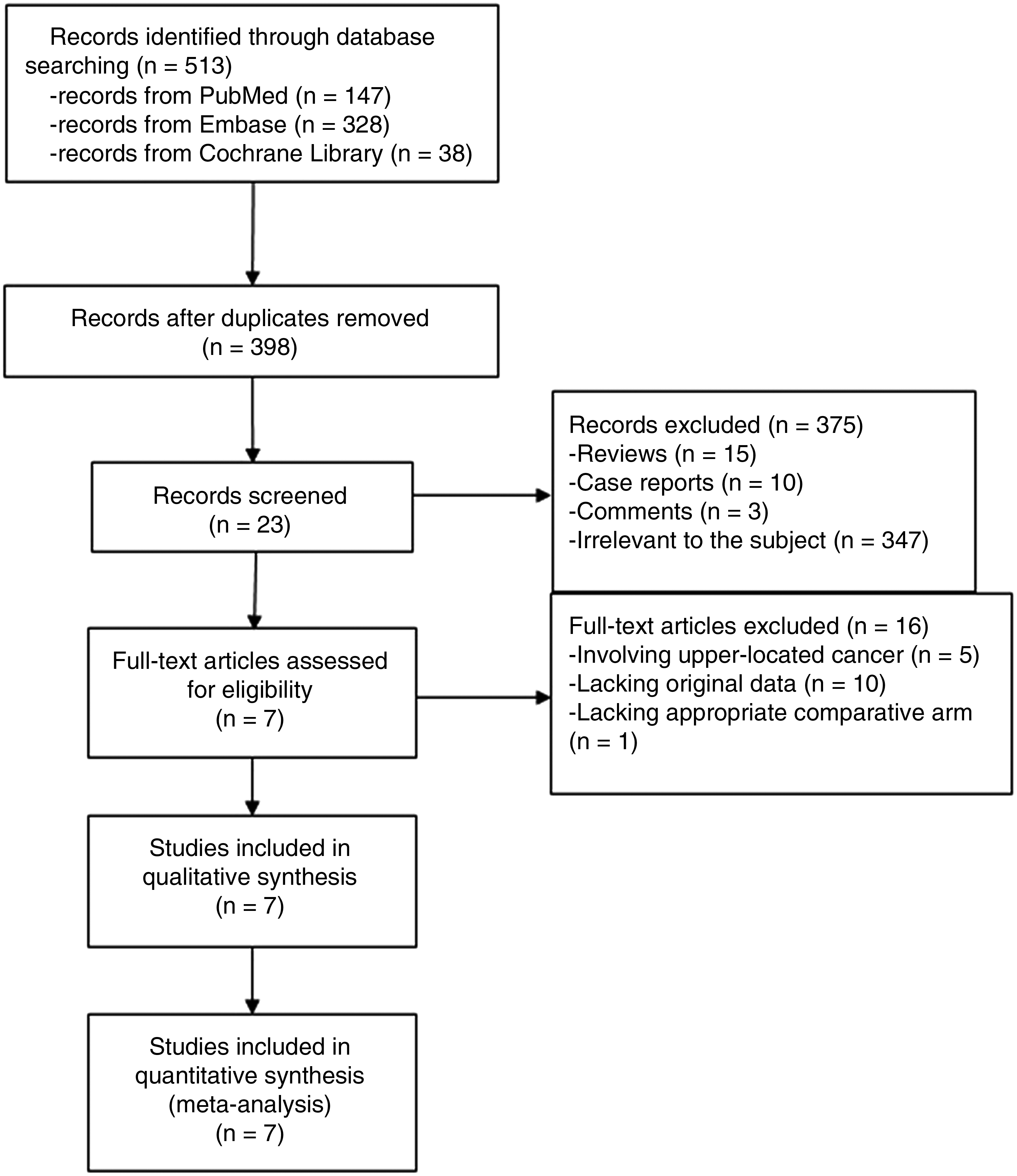
Flowchart of literature selection.
Study characteristics
Table 1 lists the characteristics of the included studies. There were totally 466 patients in laparoscopic group and 491 in open group. The seven studies for the meta-analysis included one RCT and six non-RCTs. Of the seven studies, six analyzed blood loss and lymph nodes harvest in operation, seven analyzed operating time and hospital stay, and five analyzed the time to pass first flatus. There were six studies analyzed postoperative complications, in which five clearly listed complications such as anastomotic leakage, ileus, and wound infection.
RCT, randomized controlled trial; LAP, laparoscopic resection group; OPEN, open resection group.
Comparisons of general parameters between laparoscopic and open resection
The mean blood loss of laparoscopic group was less than open group (WMD = −116.88 mL; 95% CI: −189.78 to −43.99; P = .002) (Fig. 2A). However, the differences in operating time (WMD = 11.17 minutes; 95% CI: −14.37 to 36.70; P = .39) (Fig. 2B) and lymph nodes harvest (WMD = −0.30; 95% CI: −1.29 to 0.70; P = .56) (Fig. 2C) between laparoscopic and open resection were not statistically significant. And the meta-analysis suggested that the patients in laparoscopic resection group were sooner to pass first flatus (WMD = −0.76 day; 95% CI: −1.00 to −0.51; P < .00001) (Fig. 2D) and exhibited shorter hospital stay (WMD = −2.71 days; 95% CI: −4.54 to −0.88; P = .004) (Fig. 2E) compared with open resection.
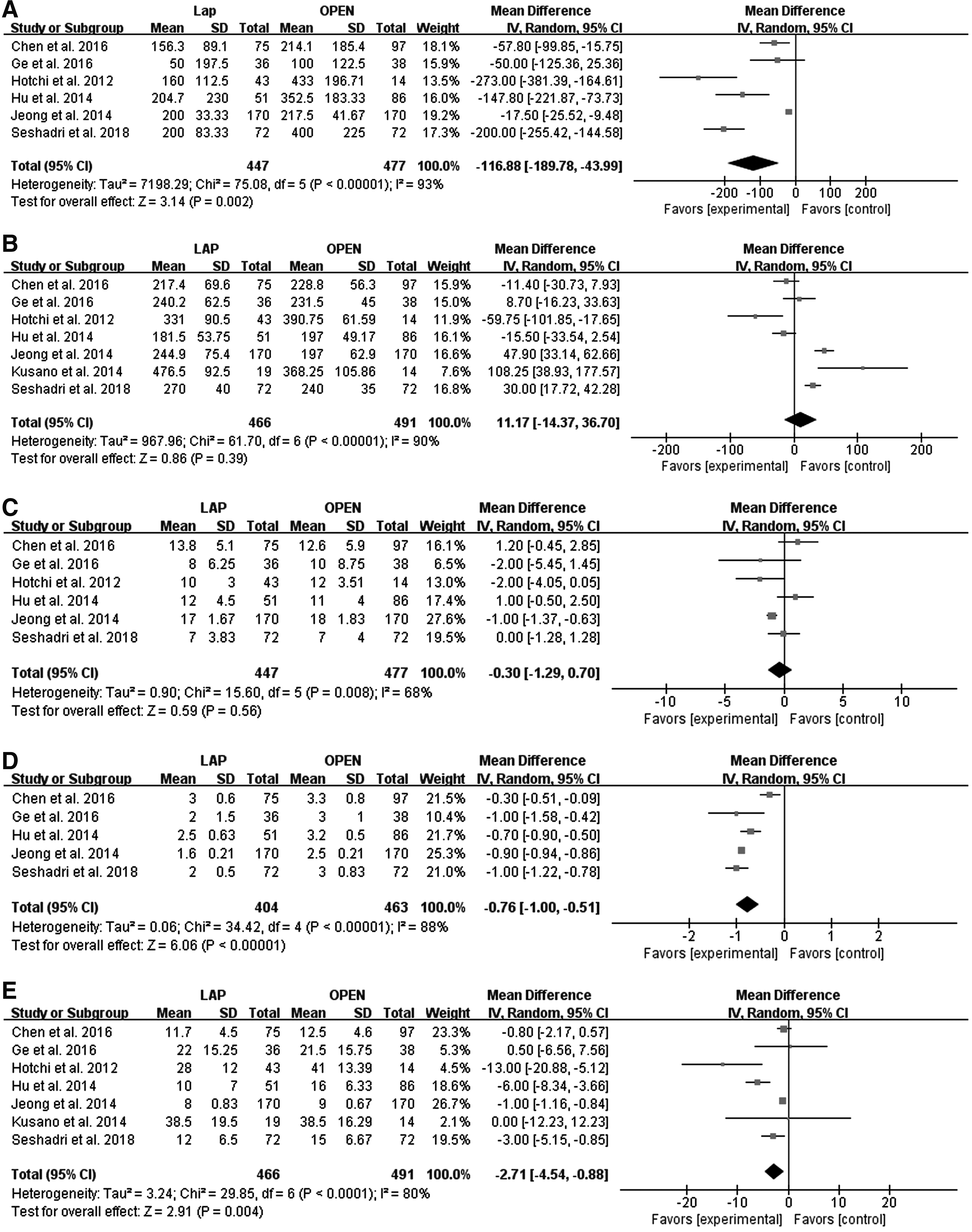
Comparisons of general parameters between laparoscopic and open resection.
Comparisons of postoperative complications between laparoscopic and open resection
Our meta-analysis on total postoperative complications showed that laparoscopic group significantly reduced their incidence compared to open group (OR = 0.63; 95% CI: 0.46–0.88; P = .006) (Fig. 3A). The present analysis revealed no significant difference in anastomotic leakage (OR = 0.67; 95% CI: 0.23–1.95; P = .46) (Fig. 3B) and ileus (OR = 0.77; 95% CI: 0.43–1.38; P = .39) (Fig. 3C) between the two procedures. But the wound infection in laparoscopic group was obviously decreased (OR = 0.46; 95% CI: 0.23–0.92; P = .03) (Fig. 3D).
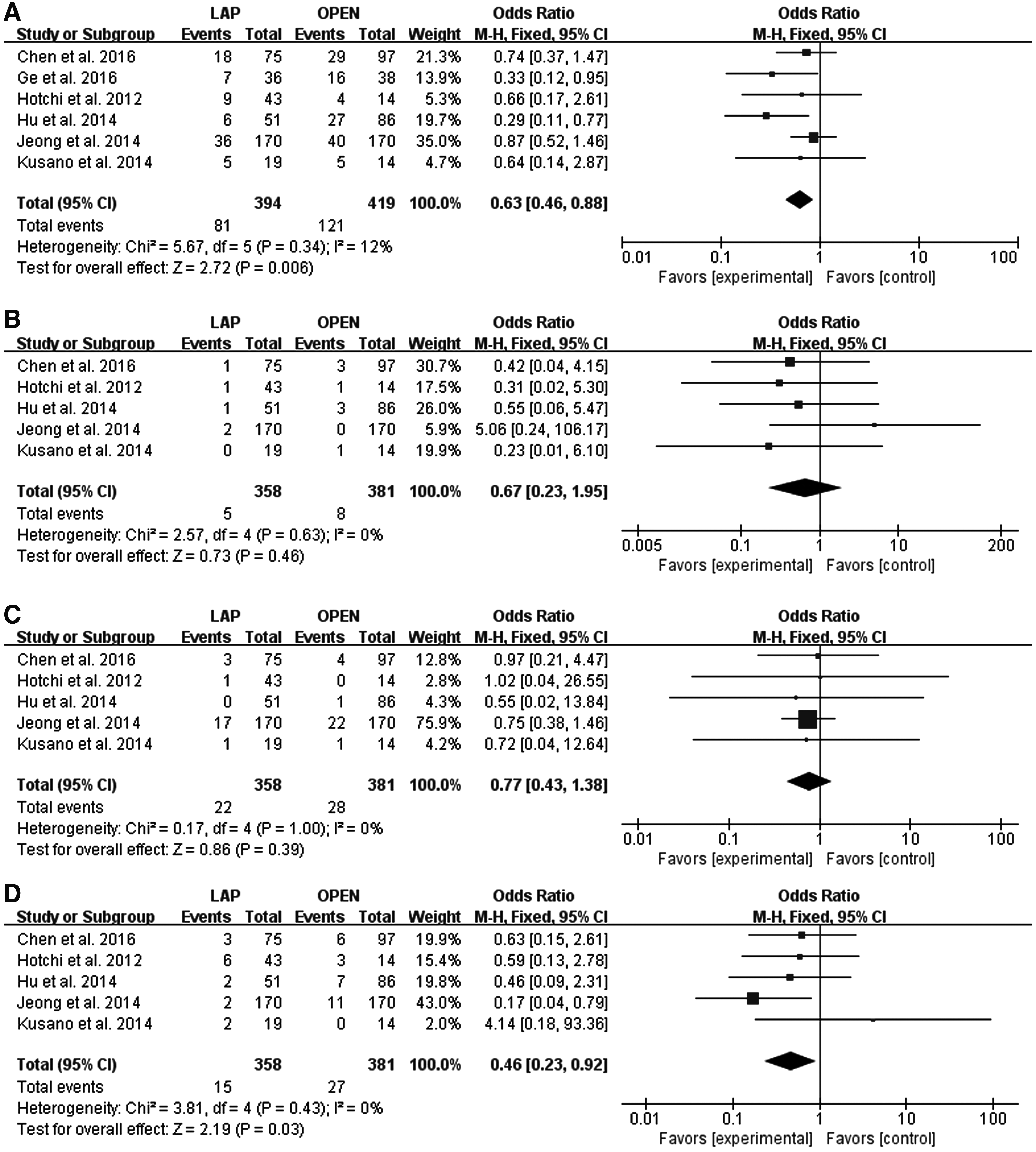
Comparisons of postoperative complications between laparoscopic and open resection.
Discussion
Rectal cancer is one of the most common malignant tumors of the digestive system. Because of lacking specific symptoms in the early stage of the disease, 70% of the patients have been in locally advanced stage at the time of clinical diagnosis and the prognosis after single treatment is poor. 23 Currently, there is a consensus that the multidisciplinary and comprehensive plan, including surgery, is essential. nCRT combined with radical surgery has become the standard therapeutic mode for middle–low local advanced rectal cancer. It can effectively increase the R0 resection rate and reduce the risk of local recurrence compared with postoperative chemoradiotherapy.12,24 Laparoscopic surgery has the advantages of less trauma and less bleeding. It can also magnify the real-time picture of operative area on the monitor. Study by Kennedy et al. showed that laparoscopic radical resection of rectal cancer after nCRT was safe and feasible for patients with mid–low rectal cancer. 25 However, because of the chemoradiotherapy, tissue inflammation, edema, and bleeding were exacerbated and increased the difficulty of laparoscopy. 26 Therefore, whether laparoscopic resection wins out over laparotomy is not clear.
In this meta-analysis, we reviewed the data from seven studies to estimate the safety and feasibility of laparoscopic resection following nCRT for mid–low rectal cancer patients. The advantage of less blood loss in laparoscopic surgery was confirmed in our study. No significant difference was found between two groups in operating time. Laparoscopic operation is quite difficult and to a large extent, the surgeon's skills and experience need to be taken into consideration for the operating time. With the experience of surgeon increases, the duration of laparoscopic surgery will gradually shorten. 27 Our data showed that laparoscopic operation was not obviously slower than open resection, as laparotomy also progressed hard after nCRT. Also, the shorter time for patients to pass first flatus and stay in hospital suggested that laparoscopic surgery could get preferable restoration effect. Early recovery of intestinal peristalsis after operation can urge patients start eating earlier and avoid the occurrence of flora shift.
The number of lymph nodes harvested was used as an important indicator on the prognosis of patients. 28 Neoadjuvant therapy was effective in downstaging lymph nodes. 29 The current study showed that both laparoscopic group and open group achieved similar number, indicating that the two approaches could get same goal of radical resection.
TME, especially Miles' operation, inevitably leads to complications such as bleeding, wound infection, pelvic abscess, and anastomotic leakage. 30 Although the rates of anastomotic leakage and ileus, two common complications deteriorating the prognosis, were similar in two groups, the results showed that laparoscopic group decreased the number of total postoperative complications. Low location of tumor and nCRT themselves took responsibility for anastomotic leakage. 31 Owing to small incision in laparoscopic surgery, patients who got wound infection were fewer.
There are still limitations to our meta-analysis that should be considered. Heterogeneity among studies was observed for several continuous variables, including blood loss, operating time, lymph nodes harvest, time to pass first flatus, and hospital stay. Lacking RCT was a significant weakness of our study. And the studies of long-term outcomes were insufficient. Multicenter RCTs with great sample sizes and long-term follow-up assessments are needed in the future.
Conclusions
This meta-analysis demonstrated that laparoscopic resection might be a technically safe and feasible approach for mid–low rectal cancer patients after nCRT compared with open resection, with favorable blood loss, analogous lymph nodes harvest, faster restoration, and less postoperative complications, despite similar operating time. These results potentially impact the treatment options in mid–low rectal cancer patients who received nCRT.
Footnotes
Acknowledgments
This work was supported by grants from Science and Technology Planning Project of Shandong Province (2011GSF11846), Key Research and Development Project of Shandong Province (GG201703230169), and Shandong Provincial Natural Science Foundation, China (ZR2014HM110, ZR2015PH024). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Disclosure Statement
No competing financial interests exist.