
Abstract
Abstract
Introduction:
Thoracoscopic esophageal atresia repair has become increasingly popular, but is still limited to a few expert centers and has some challenges and shortcomings. One of them has a longer operation time compared with conventional thoracotomy. Magnetic compression anastomosis may contribute toward shorter operation times by avoiding the time-consuming anastomotic suturing. We aimed to establish a method of testing sutureless anastomoses in parallel to having swine eating the natural way.
Materials and Methods:
We used four juvenile Pietrain swine—aged 8 weeks, weighing 15 kg—to establish a living animal model after preceding cadaver tests. Esophagi were fully mobilized through right-sided thoracotomy to gain sufficient length to create an esophageal loop that served as a bypass for food after magnet deployment. Six hours later, patency of the bypass esophageal loop was assessed by passing an orogastric tube and by allowing swine to drink methylene blue-stained water. We also tested the device stability using the classical burst pressure test.
Results:
The esophageal lumen was patent for feeding tube. Swine were able to drink and methylene blue colored fluid reached the stomach. Clinical signs of obstruction such as regurgitation or coughing were absent. Magnets sustained burst pressures up to 200,000 Pascal until they became disrupted. At 6 hours after magnet placing, we already saw subtle esophageal mucosa erosions indicating the beginning of anastomotic formation.
Conclusion:
This animal model is useful to test different magnet designs for sutureless esophageal anastomosis or even future devices for in vivo tissue engineering.
Introduction
Since Cameron Haight's first successful repair of esophageal atresia in 1941, 1 pediatric surgeons strive to improve the anastomosis by other techniques than suturing: The first to use magnets were Hendren and Hale, whose work aimed to spare diseased children esophageal substitution by electromagnetic bougienage and subsequent esophageal lengthening.2,3 Despite their encouraging results, the idea of a magnetic compression anastomosis in esophageal atresia went dormant until Zaritzky et al. revived4,5 this technique. It was further improved and successfully tested in bowel anastomoses of both adults 6 and children. 7 Based on these successful clinical applications in gastrointestinal anastomoses, the next step was to use magnetic compression anastomosis in esophageal atresia to reduce the extraordinarily high stricture rates encountered by Zaritzky et al.4,5 Therefore, magnets were evaluated in an esophageal anastomosis model. This test was however limited by using adult swine and keeping them at nil per os for some days and postoperative oral feeding limited to water. 8 Nevertheless, it was an important first step to utilize magnetic compression anastomosis for esophageal atresia as it offers the potential to overcome a substantial shortcoming of thoracoscopic esophageal atresia repair; the longer operative times compared with conventional thoracotomy. 9
We aimed to not only evaluate the magnets in a juvenile porcine model to contribute toward a faster and easier esophageal anastomosis, but also to introduce a new method that allows simultaneous testing of esophageal anastomotic techniques in parallel to the swine feeding in a natural way in the immediate postoperative interval. Feeding per mouth is particularly important for long-term studies, because pigs will manipulate foreign bodies within their reach—especially in their penmates—as it is part of their normal behavior.10,11
Materials and Methods
Animals
We used four Pietrain swine (Sus scrofa domestica) of both sexes weighing between 13 and 17 kg aged 2 months. The Pietrain breed has been shown to be particularly useful for esophageal surgery. 12 Swine were housed in a closed facility with a 12 hours dark–light cycle with artificial lightning between 0600 and 1800 hours and were acclimatized to our husbandry conditions for 1 week. The study was approved by the state's competent authorities for the protection of laboratory animals (permit no.: G-17-1-033-E1) in accordance with the German Animal Welfare Act and the directive 2010/63/EU.
Surgical procedure
Before establishing the procedure in living swine, we explored the feasibility of the suggested method in two 35 kg swine killed for a different project at our institution. As it was successful, we proceeded to using live swine.
They received general anesthesia with endotracheal intubation. The thoracic cavity was opened through a right-sided thoracotomy in the fifth intercostal space with transpleural exposure of the esophagus at the carinal level. Two magnets of 8 mm diameter were per-orally placed sequentially using a specifically designed applicator. After positioning of the first magnet at the carinal level (Fig. 1A), a silicone vessel loop was used to keep the second orally placed magnet separated from the first within the true lumen (Fig. 1B). This allowed the magnets to mate in a side-to-side configuration, and the magnetic compression to form the future anastomotic site while at the same time forming a bypass loop for food transport with the magnets keeping the esophagus fixed in its desired position (Fig. 2). The thoracic cavity was closed in layers and a dressing applied to the wound.

Construction of the esophageal loop bypass.
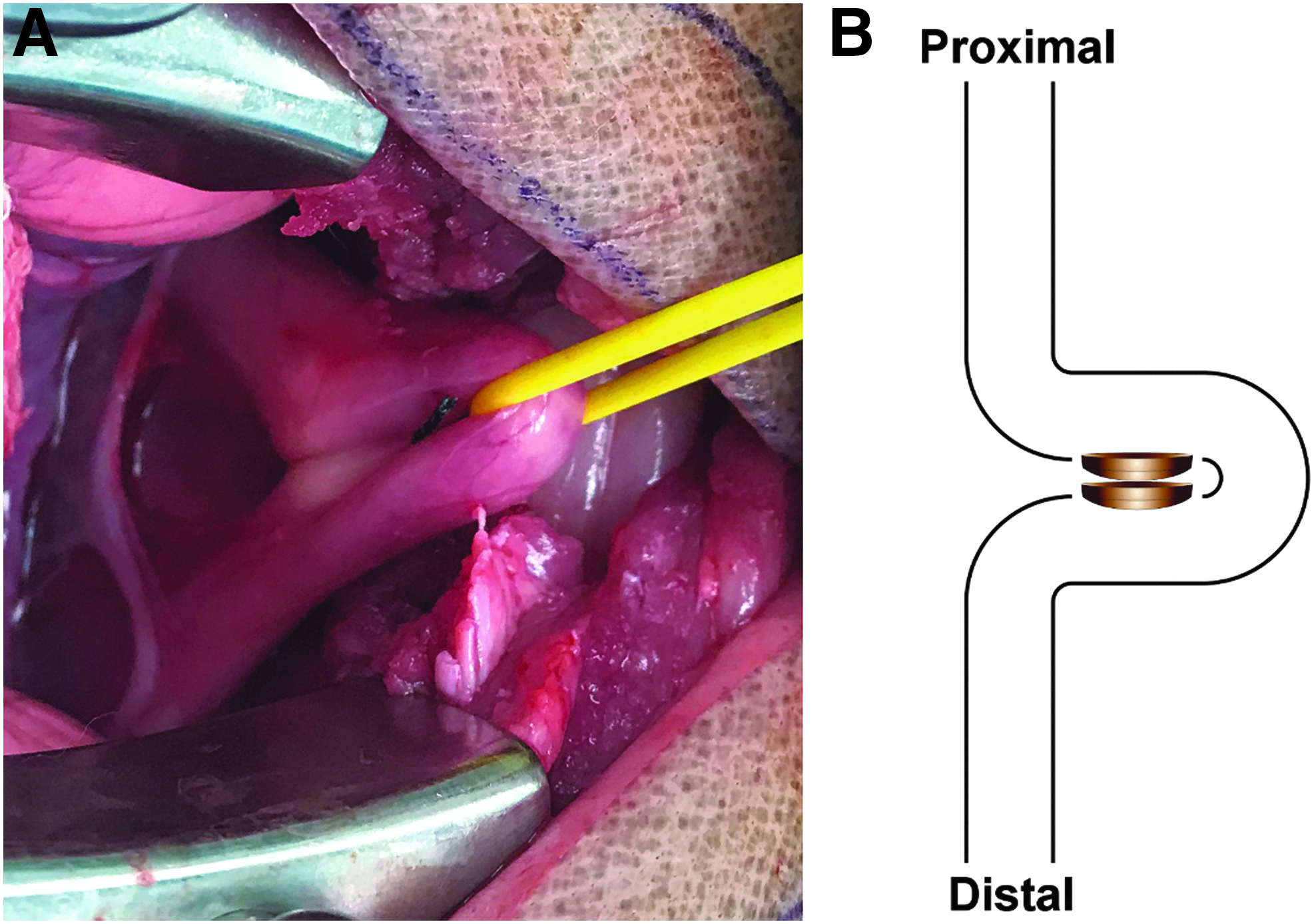
Esophageal loop bypass in situ.
The magnets were similar to those described elsewhere, 8 but had a reduced outer diameter of 8 mm to fit inside the esophagi of juvenile swine.
Evaluation of the esophageal loop
Swine were provided water mixed with methylene blue to evaluate fluid passage along the esophageal loop and killed with an overdose of pentobarbital 6 hours postoperatively. After killing, we explanted the esophagus, tested loop patency with a 24F orogastric tube (Fig. 1C), and macroscopically inspected the magnet contact area. Device stability was tested using classical 13 burst pressure tests. The explanted esophageal loop was occluded using straight mosquito clamps placed equidistant to the esophageal loop on both sides. Before clamping, a silicone tube was introduced into the distal esophageal lumen. A manometer and a syringe were connected to the other end of the silicone tube. A similar experimental setup has been depicted elsewhere. 14 We then slowly inflated the esophagus and recorded the pressure until the esophagus became disrupted. The pressure at disruption is the burst pressure measurement.
Results
Operation times were between 20 and 30 minutes per swine. The esophageal lumen was patent as demonstrated by the swine being able to drink postoperatively without regurgitation of water, coughing, or respiratory distress. The characteristic methylene blue stains coloring the stomach proved a free passage of fluids the swine drank postoperatively. After postmortem esophageal explantation, we verified this finding by passing a 24F orogastric tube through the esophageal loop without encountering resistance (Supplementary Video S1).
We also subjected the esophageal loop to burst pressures to evaluate its stability with magnets in place and observed disruptions of the magnets at burst pressures of 60,000 and 80,000 Pascal in three swine. Maximum burst pressures of 200,000 Pascal were recorded just once. Magnets were highly effective in creating an anastomosis as we already observed subtle erosions of the esophageal mucosa after 6 hours, indicating the beginning of anastomosis formation (Fig. 3).
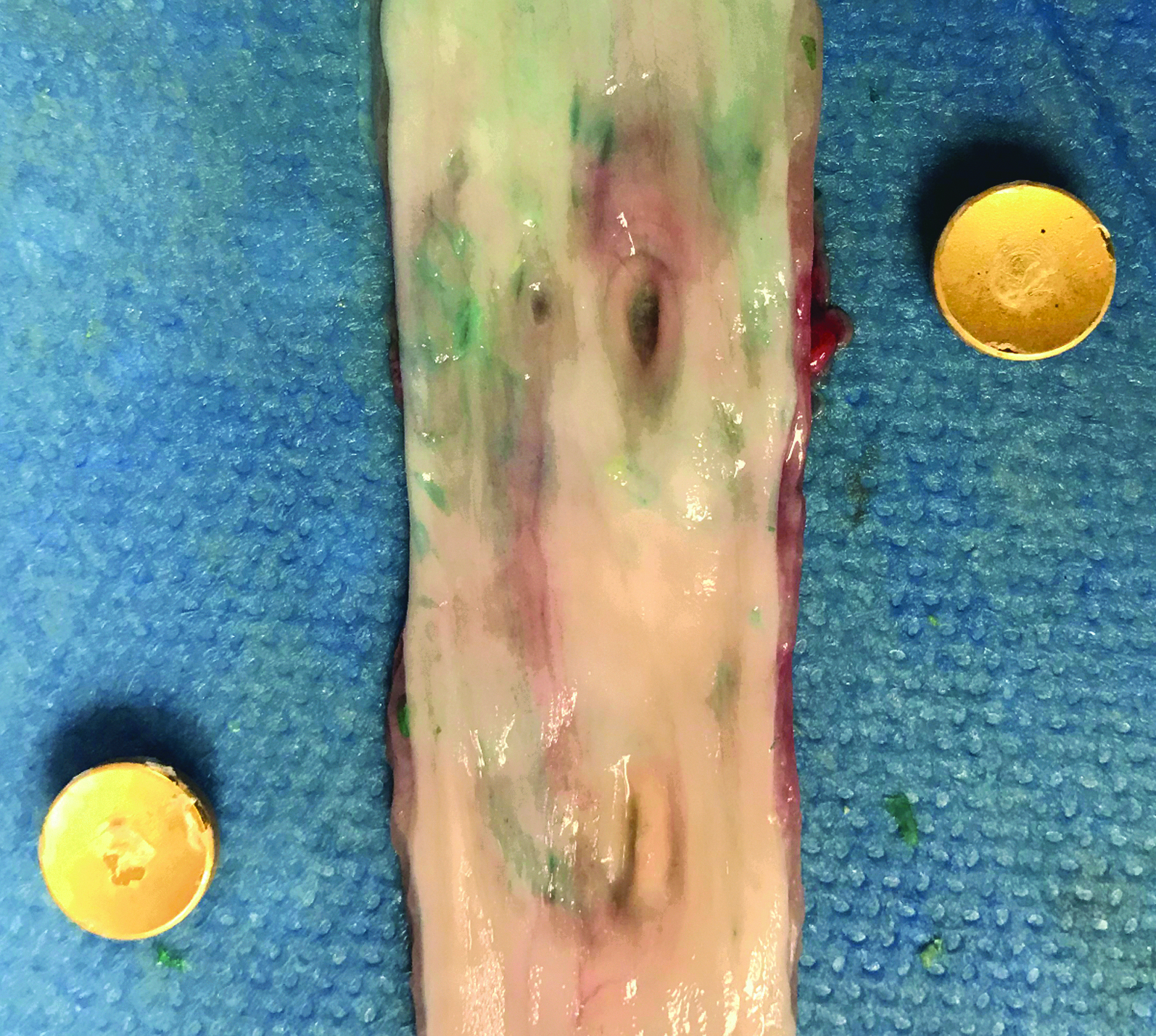
Effect of magnetism at the esophageal wall. Mucosal erosions after 6 hours in situ at the esophageal wall.
Discussion
Before being used in humans, a novel technique should be thoroughly tested in animal models. This is particularly important in children. In the case of esophageal atresia, the introduction of new anastomotic techniques have at times been haunted by high rates of leakages and subsequent mediastinitis and esophageal strictures: This included esophageal stents, 15 mesh replacement after esophageal resection, 16 and patch repair of esophageal segmental defects. 17 Magnetic compression anastomosis might be a potential candidate to aid with thoracoscopic esophageal atresia repair—which is still limited to highly specialized centers 18 —by obviating the need for intracorporeal suturing and thereby reducing operation times. This may facilitate truly minimally invasive esophageal atresia repair in the future. 19
The challenges of creating an animal model for the testing of magnetic esophageal anastomosis in swine is to create a technique that allows them to feed right after the procedure, as swine tend to manipulate foreign bodies such as gastrostomy tubes or long-term intravenous catheters for total parenteral nutrition within their reach, typically in penmates.10,11
In our experiments, we were able to create a model that allows swine to drink postoperatively. We also demonstrate the extraordinary stability of the magnets separated by two layers of healthy esophageal wall. They were resistant to bursting pressures between 60,000 and 200,000 Pascal. Although this is much lower than the maximum pressures obtained from cadaveric human esophagi that sustained 1,189,000 Pascal, 20 it was similar to those burst pressures obtained from canine thoracic esophagi (187,654 Pascal). 21 More importantly, these burst pressures were above the physiologic swallowing pressures obtained from healthy humans, which were measured with 13,516 Pascal. 22 As swallowing pressures are higher in supine than upright position 23 —likely to overcome the missing gravitational forces—our results suggest that the magnets will stay in place during regular feeding and its esophageal pressures. We therefore postulate that in the immediate postoperative phase, the esophageal magnetic anastomosis construct is highly resistant to pressure and resistant to leak.
Moreover, our method is suitable for experimental evaluation of novel techniques beyond magnetic compression anastomosis. Although it has successfully been demonstrated that Göttingen Minipigs tolerate gastrostomies for weeks 10 or even months, 24 our esophageal loop guarantees a normal gastrointestinal food consumption of swine and thereby reduces their experimental stress. This allows a much less stressful long-term evaluation of sutureless anastomotic devices, such as esophageal stents, 15 magnets,8,25 or even prostheses for tissue engineering. 26 This is particularly useful as swine have esophageal tissue properties similar to humans—especially piglets27,28—but are at the same time prone to developing esophageal stenosis.27,29,30
After proving that the bypass loop indeed allows the passage of chow by natural way, the next step will be survival experiments in which the animals survive up to 2 weeks to characterize the evolution of the anastomosis and to assess stricture formation.
Conclusion
Our esophageal loop allows regular feeding per mouth despite testing sutureless anastomotic devices. The esophageal loop is easy to construct in less than half an hour and might be suitable to test magnets and other esophageal devices.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.