
Abstract
Abstract
Background:
The management of neonatal short bowel syndrome can be challenging, and it is critical that these babies are managed in a multidisciplinary team setting with specialists who are experienced in the complex management of these children. One of the surgical strategies, initially published by the Bianchi team in Manchester, UK, is controlled tissue expansion program (CTE) which is done via the insertion of catheters into the proximal and distal bowel in the form of tube stomas. The clamping of the proximal tube allows for an increase in length and circumferential diameter of the proximal bowel for a period of time, whilst the distal tube stoma allows for easy refeeding of proximal bowel contents into the distal bowel.
Method:
CTE is associated with the risk of dislodgement and exposing patients to further surgical procedures with the risk of losing more bowel length. This article describes a new method in the management of such a complication through a less invasive approach of an image-guided procedure by interventional radiologists.
Conclusion:
Radiologically guided tube stoma reinsertion in a child with ultrashort bowel syndrome is a promising technique and should be considered in a CTE program in the management of short bowel syndrome.
Introduction
Short bowel syndrome (SBS) can be defined as a multisystem disorder caused by malabsorption of nutrients due to inadequate bowel length. 1 It is a common cause of intestinal failure especially in the neonatal period. The significant reduction in the functional gut mass below a critical threshold causes disturbances in growth, hydration, and/or electrolyte balance.2,3
It was recorded in 0.7% (89/12,316) of very low birth weight infants born during the period 2002–2005 at the National Institute of Child Health and Development (NICHD) neonatal research network centers. Its frequency increased in an inverse relationship with birth weight. 4 Necrotizing enterocolitis is the most common cause of SBS in neonates followed by gastroschisis, intestinal atresia, and intestinal malrotation/volvulus. 3
The management of SBS patients is complex and needs a multidisciplinary approach. Advances in medical management and liver salvageable parenteral nutrition (PN) have significantly improved the outcome of these patients. 1 Surgical techniques, which include bowel expansion, different types of bowel lengthening, and restoration of bowel continuity, have been integrated in the medical management of these children. Such an integrated system of management has produced improved results in recent years in highly specialized and experienced centers.1,5
The controlled tissue expansion (CTE) program for children with severe SBS was initially described by Bianchi, and a series was reported by the Manchester team in the United Kingdom in 2011. 6 The program aims to increase the length and circumferential diameter of the bowel for a period of time. This makes a new and greater surface area for absorption and more tissue for lengthening and tailoring.
Tube stomas are created surgically by inserting catheters into the proximal and distal bowel in a way similar to the standard surgical formation of gastrostomies. The catheters are brought out through the skin through separate stab incisions in the anterior abdominal wall. CTE is done through clamping the proximal tube stoma in a graded manner with increasing enteral feeds. The effluent from the proximal tube stoma can be refed back into the remnant distal bowel through the distal catheter. 6 Occasionally these tubes can get dislodged. If the tract has matured, they can most of the time be reinserted easily through the tract. However, in some instances, the tract may have closed, which would ultimately put the child in intestinal obstruction if the dislodged catheter was the proximal catheter. Before this case report, surgery would be necessary to reinsert the catheter and to relieve the obstruction with a risk of losing more bowel as a result of the surgical procedure. In this case report, we describe a new technique used in CTE to manage such a complication using an image-guided procedure through interventional radiology.
Case Report
A 27 weeks gestational age preterm baby girl was diagnosed with stage 3 necrotizing enterocolitis according to the Bell Classification at the age of 3 weeks. She underwent exploratory laparotomy and resection of a large amount of gangrenous bowel. In the initial procedure, the abdomen was packed as the baby became unstable during surgery. A second look laparotomy was undertaken and further resections were carried out. The child was left with 9 cm of proximal jejunum and 2 cm of distal ileum. The distal ileum was over sewn and dropped back into the abdomen in an attempt to preserve the ileocecal valve. The proximal jejunum was brought out as a normal jejunostomy. The remnant bowel length placed the child in the ultrashort bowel group. Three months later, another laparotomy was performed and tube stomas were created in the proximal jejunum and distal ileum, and CTE was commenced in an attempt to expand the proximal jejunum and to enhance the quality of the distal bowel through refeeding. In addition, the child underwent an aggressive Liver Rescue Regime as previously described by the Manchester team in the United Kingdom. 1 This involved fat-free PN for a period of time followed by gradual introduction of small amounts of lipids in the PN while monitoring the liver function tests. Oral intake was enhanced during the CTE program, which in this child lasted for about 5 months.
During the CTE program, her proximal catheter became dislodged and unfortunately the tract closed. The child remained stable with no signs of intra-abdominal leak. A multidisciplinary meeting was held and it was decided to attempt to reinsert the catheter through interventional radiology using ultrasonographic and fluoroscopic-guided access to the jejunum to save the patient another laparotomy with the potential risk of losing more bowel length.
Steps of the Procedure
A 4F Terumo glide catheter with a 0.035 guide wire was inserted through the mouth into the stomach and through the duodenum into the proximal jejunum. This was done under fluoroscopic guidance.
Water-soluble contrast was injected through the tube, which demonstrated the blind-ending jejunal loop of bowel, the lower margin of which was demonstrated both ultrasonographically and fluoroscopically to correspond with the site of the original stoma (Fig. 1).

Delineated blind jejunal loop (site of proximal stoma).
A 24-gauge Jelco catheter was inserted under ultrasonographic guidance adjacent to the old stoma tract and into the blind-ending jejunal loop.
Through the catheter, a 0.018 floppy-tipped guide wire was inserted into the bowel lumen under fluoroscopic guidance. A small incision was made around the wire. A 5F coaxial dilator was inserted over the wire. The wire was removed (Fig. 2). Contrast injected down the inner dilator demonstrated satisfactory placement of the outer dilator within the bowel lumen. The inner dilator was then removed.

Dilator/sheath inserted inside the lumen of proximal bowel.
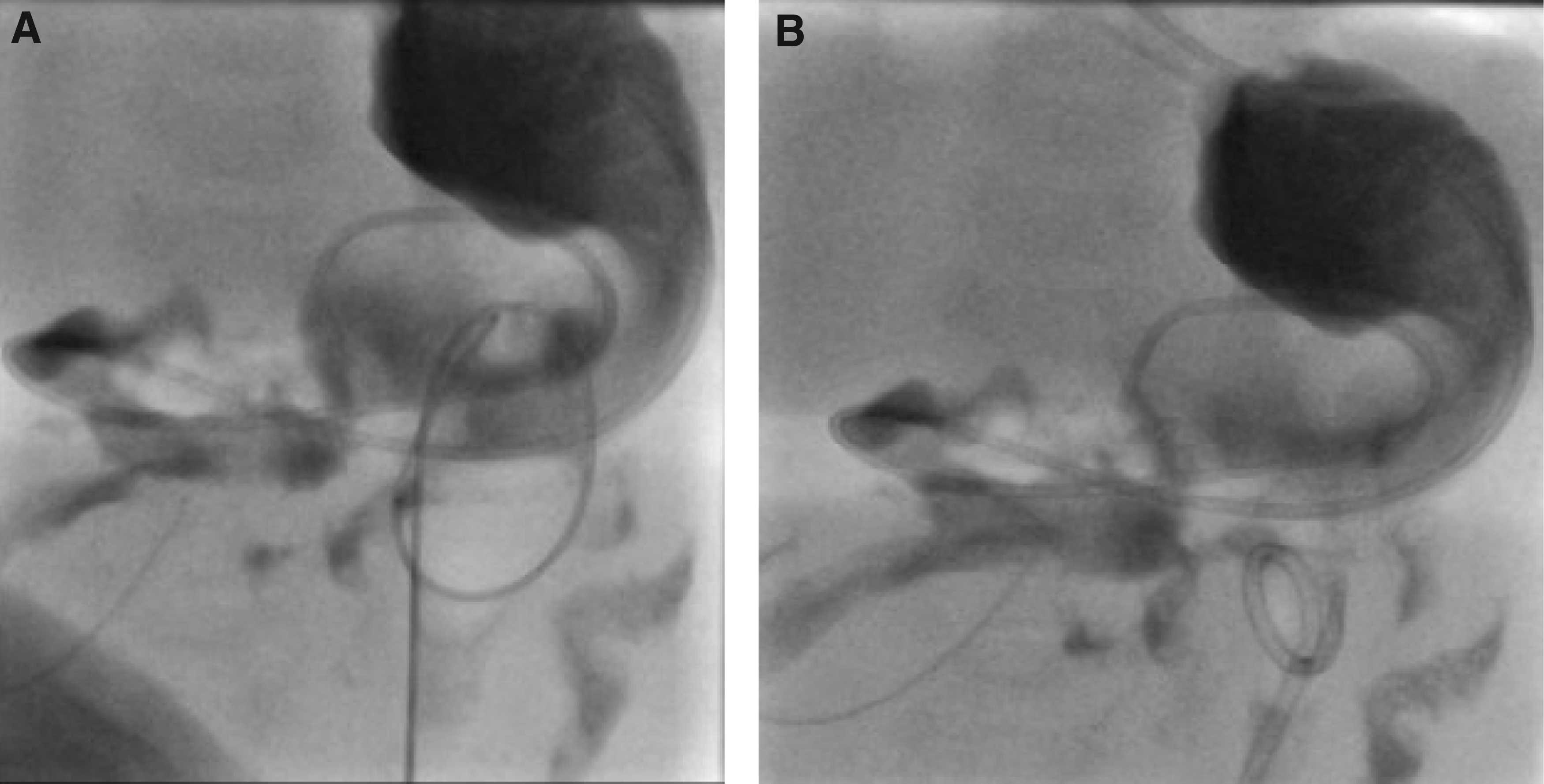
A 0.035 Amplatz wire was then placed down the outer dilator, and the outer dilator was removed. Over the Amplatz wire, a 6.3F Dawson Muller tube was placed. The guide wire was removed (Fig. 3A, B). The Cope loop was formed and tied. Contrast injection demonstrated satisfactory placement within the bowel lumen.
To prevent the same loss of access to the afferent distal ileal stoma in the right upper quadrant, the catheter was exchanged for another 6.3F Dawson Muller tube and the position of the tube was confirmed with contrast (Fig. 4).
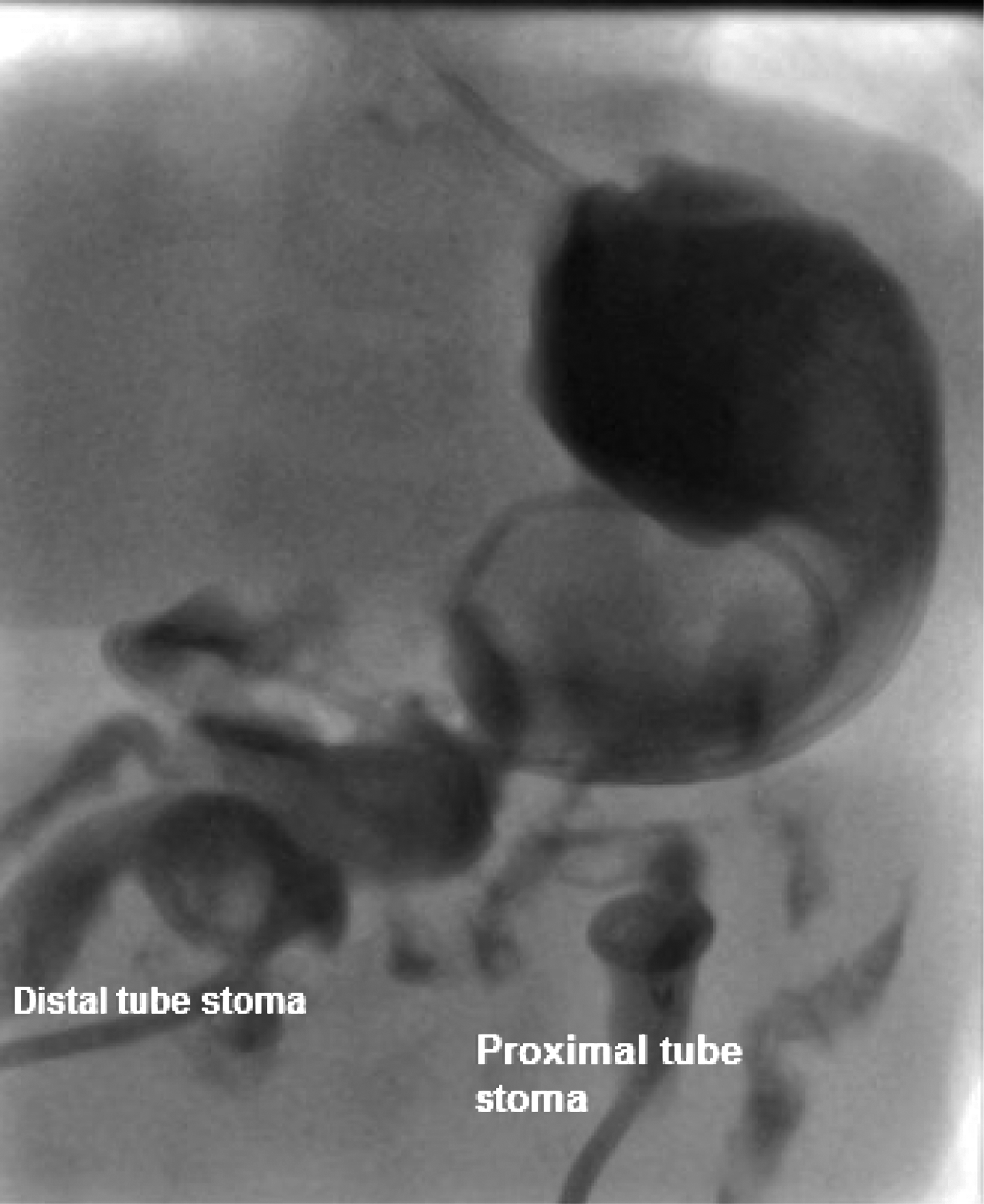
Successful ultrasonographic and fluoroscopic-guided access of jejunal proximal stoma and replacement of Foley catheter distal ileal stoma. Contrast goes smoothly intraluminal.
Discussion
The surgical management of the ultrashort bowel patient is a real challenge, and it should not be approached without multidisciplinary team and expertise.
The idea of bowel expansion as a stepwise procedure for bowel lengthening was initially introduced by Georgeson et al. 7 The authors described creating an intestinal obstruction through a nipple valve, which created a partial intussusception. This technique created noncontrolled bowel dilatation within a 5 week period. 8 In the intestinal rehabilitation program in Manchester, United Kingdom, Bianchi modified the nipple valve idea and established the CTE program. 9
In this program, successful bowel expansion can be achieved within 12–24 weeks through surgically placed tube stomas into the proximal and distal bowel as previously described. The goal of the program is for the child to achieve full complement of feeds with a 3–4-hour clamp of the proximal tube stoma. Tube stomas have the advantages of minimal risk of prolapse, minimal skin excoriation, easier nursing care, and precise measurement of effluents volumes. However, one of the most encountered problems is tube dislodgement, which usually needs surgical intervention if the tract had closed. 6
Surgery to reinsert a dislodged tube could potentially cause further loss of bowel length, which can severely affect the management of these patients. Our patient was an ultrashort bowel patient and hence it was extremely pertinent that we preserve all her remnant bowel. In such cases, we would advise that a reinsertion using the interventional radiology procedure described in this study would be a reasonable first step if feasible.
In our case, the image-guided procedure was successful without any complications. The proximal jejunum was still attached to the anterior abdominal wall, which made it easier for the interventional radiologist to cannulate the bowel. However, potential complications could be misplacement of the catheter or bowel perforation and peritonitis. To avoid this, meticulous insertion with full fluoroscopic and ultrasonographic guidance is advised. Monitoring the child postinsertion and restarting feeds again gradually are considered safe approaches after the procedure. The CTE program was completed and the child underwent bowel lengthening. The child is currently at home at the time of writing this article and has been weaned off PN and is on full enteral feeds.
We believe this case to be the first published case of successful radiologically guided tube stoma reinsertion in a child with ultrashort bowel syndrome. We believe it is a promising technique and should be considered in a CTE program in the management of SBS.
Consent for Publication
Informed consent was obtained from the parent of the patient for publication of this case report.
Footnotes
Disclosure Statement
No competing financial interests exist.