
Abstract
Abstract
Background:
Common bile duct stones (CBDS) are treated with endoscopic retrograde cholangiopancreatography (ERCP) followed by laparoscopic cholecystectomy (LC) or with the single-stage laparoscopic common bile duct exploration (LCBDE) and LC. Multiple ERCP attempts and failure increase the risk of postprocedural complications. In such circumstances surgery is advocated. The aim of the study is to compare the outcome of LCBDE and LC in patients who had never had an ERCP, to that of patients who underwent previously failed ERCP.
Methods:
A retrospective analysis of 54 patients undergoing LCBDE and LC between 2010 and 2017, was performed. Patients were divided in 2 groups: primary surgery (group 1), surgery after failed ERCP (group 2). Demographics and preoperative investigation results were collected. Comparative outcomes were common bile duct (CBD) clearance rate, operative time, conversion to open rate, postoperative morbidity, mortality, and hospital stay. Data were evaluated with the Student's t, Chi-square, or Fisher's tests. Results were considered as statistically significant when P < .05.
Results:
In both groups CBD clearance was above 90%. The mean operative time was longer in group 2 (130.3 minutes ± SD 83.72 vs. 178.73 ± 57.22; P < .05). There was no difference in the conversion to open and postoperative complication rates between groups. A bile leak occurred in 2 patients from group 1, 3, from group 2. No postoperative mortality occurred. The median hospital stay was longer in group 2 (2 days ± SD 2.54 vs. 5 ± 5.77; P < .05).
Conclusions:
LCBDE and LC is safe and effective in patients who had previous failed ERCP. If ERCP failure is anticipated and/or the risk of post-ERCP complications is high, surgery should be considered as the first-line treatment of CBDS. Longer intraoperative time and hospital stay are expected.
Introduction
Common bile duct stones (CBDS) are frequently encountered in clinical practice. It has been estimated that they occur in up to 20% of patients with symptomatic gallstones.1–9 The management of choledocholithiasis is still under debate. Some authors favor the sequential treatment, where the endoscopic retrograde cholangiopancreatography (ERCP) is followed by a delayed laparoscopic cholecystectomy (LC). Others prefer the single-stage approach, where both the laparoscopic common bile duct exploration (LCBDE) and cholecystectomy are performed at the same time.10–14
Occasionally ERCP fails in either cannulating the common bile duct (CBD) or removing CBDS. This may happen in the presence of hostile periampullary anatomy or impacted stones, respectively. In the second case, a biliary stent is often positioned to allow for the decompression of the biliary tree. Repeated endoscopic manipulation of the ampulla and CBD and the positioning of a biliary stent may result in increased local inflammation and fibrosis.15,16
Failure of the endoscopic treatment demands the use of the single-stage approach. 17 In such a condition, surgery may be technically challenging due to the local inflammatory changes.
The aim of the study is to compare the outcome of LCBDE and LC in patients who had never had an ERCP, to that of patients who underwent previous failed ERCP.
Materials and Methods
No Institutional Review Board approval was required for the study purpose and design. From November 2010 to May 2017, all the patients with confirmed diagnosis of CBDS, who underwent the single-stage treatment on an elective basis, were considered into the study. Exclusion criteria were: a planned open procedure, previous cholecystectomy, and the presence of causes of CBD obstruction other than choledocholithiasis. Patients were divided in two groups: primary LCBDE and LC (group 1), LCBDE and LC after previously failed ERCP (group 2), respectively.
Demographic data, American Society of Anesthesiologists (ASA) score, and results from preoperative investigations, were collected.
At our institution, CBDS are most commonly treated with the sequential endoscopic/surgical approach. If the ERCP fails, decision as to whether repeating endoscopy or performing surgery depends on the reason of failure. Therefore, LCBDE and LC are considered when the ERCP either fails once or multiple times or is contraindicated and the CBD diameter is ≥8 mm.
Surgery is carried out with a standard 5-trocar technique. If the cystic duct (CD) is dilated at least as much as the size of the CBD stone(s), the common bile duct exploration (CBDE) is performed through the transcystic route, using a 3-mm choledochoscope. The stone is extracted with an endoscopic basket and the CD stump is closed with an endoloop or clips. If the CD is not enlarged or a stone is impacted in the CBD, a longitudinal choledochotomy is performed and a 5-mm choledochoscope is used. Stones are retrieved with the endoscopic basket or an inflatable balloon tip catheter. If present, the CBD stent is removed at this stage. The choledochotomy is repaired using interrupted slowly absorbable sutures and a T-tube drain is inserted in the CBD if there are conditions that may increase the risk of a postoperative bile leak (i.e., tissue edema and/or fibrosis). The gallbladder is then removed in the standard way.
For the study purposes, after extraction, CBDS number and size (≤1 cm or >1 cm) were recorded.
Primary outcomes of the comparison between groups were: CBD clearance rate, postoperative morbidity, mortality, and length of hospital stay. Postoperative morbidity and mortality were considered when occurring up to 30 days after surgery. Secondary outcomes were the operative time and conversion to open rate.
For statistical analysis, Student's t-test was used for nonparametric data; two-tailed Chi-square test or Fisher's test were used to compare differences in frequencies (SPSS, Inc., Chicago, IL). Results were considered as statistically significant when P < .05.
Results
Fifty-nine consecutive patients with confirmed diagnosis of CBDS underwent LCBDE and LC. Five were excluded from the study because of intraoperative diagnosis of metastatic liver disease (1) and planned open procedure (4), due to previous multiple intra-abdominal surgeries. Out of the 54 remaining patients, 21 were included in group 1 and 33 in group 2.
Preoperative data
Patients in group 2 were older (P < .05), had higher preoperative serum alkaline phosphatase (ALP, P < .05), and a larger CBD diameter (P = .0001) than group 1 (Table 1).
Demographics and Preoperative Clinical Data
Values shown in bold are statistically significant.
ALP, alkaline phosphatase; ASA, American Society of Anesthesiologists; CBD, common bile duct; SD, standard deviation.
Previous ERCP was attempted once in 15 patients, twice in 12, 3 times in 4, and 4 times in 2. Causes of ERCP failure were mainly impacted or multiple CBDS and the presence of a periampullary diverticulum (Fig. 1).
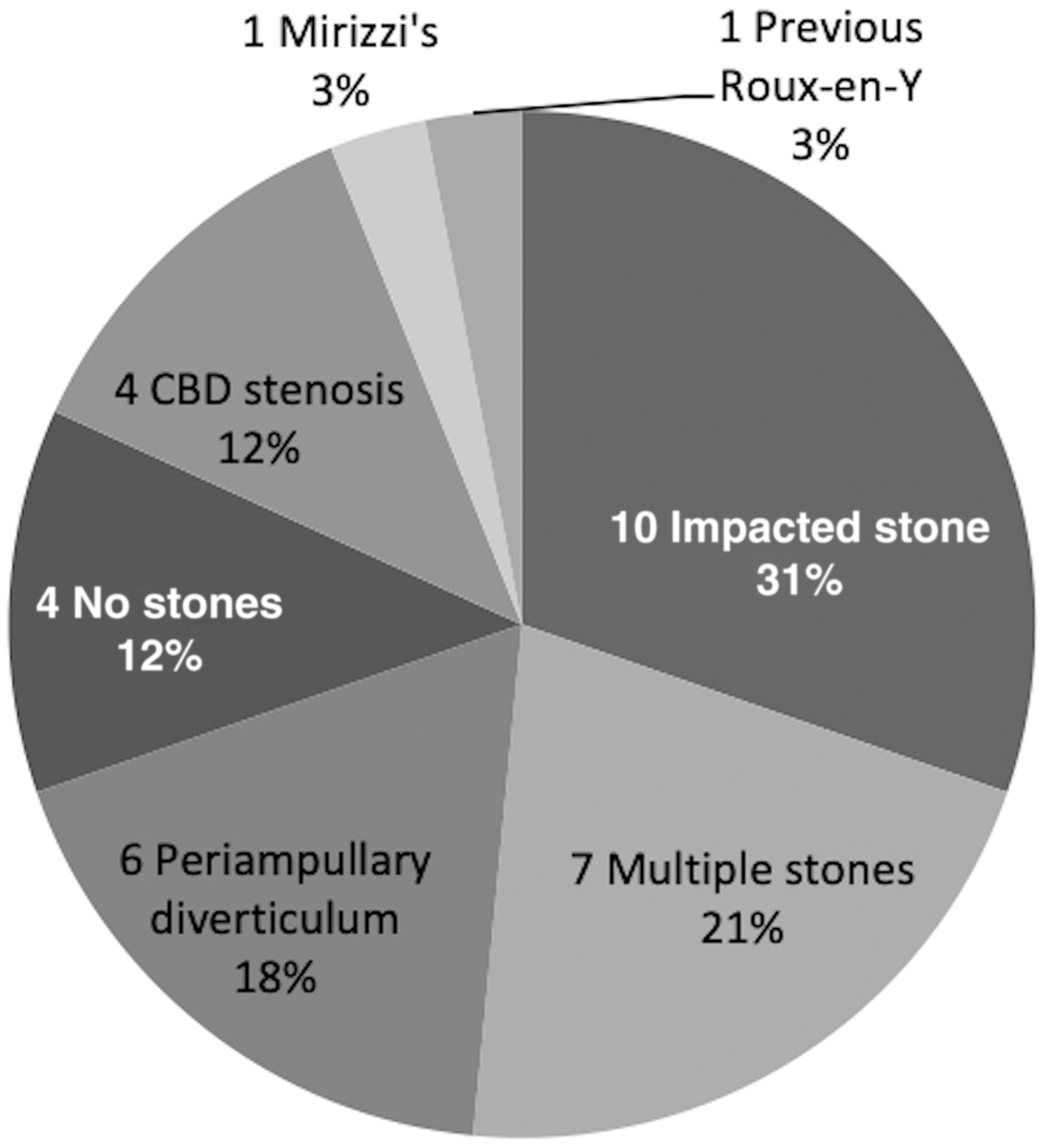
Causes of endoscopic retrograde cholangiopancreatography failure. CBD, common bile duct.
Intraoperative data
Local dense tissue fibrosis was described in 19% of group 1 patients and in 48.4% of group 2 (P < .05) (Table 2). Conversion to open was necessary in 6 cases, 2 in group 1, and 4 in group 2. Reasons to convert were dense adhesions in 5 (2 in group 1, 3 in group 2) and rupture of the endoscopic basket in a patient from group 2.
Intraoperative Data
Values shown in bold are statistically significant.
CBD, common bile duct; CBDE, common bile duct exploration; CBDS, common bile duct stones; SD, standard deviation.
The transcystic approach was used in 66.7% cases from group 1 and the transcholedochal in 87.9% from group 2 (P = .0001).
CBD clearance was achieved in 19/21 (90.5%) patients from group 1 and in 30/33 (90.9%) from group 2. In group 2, 18 out of 19 stents were removed during surgery. One was taken out endoscopically 2 weeks after surgery.
A T-tube was used in 1 patient from group 1 and in 5 from group 2.
Mean operative time was longer in group 2 (P < .05).
Postoperative data
No postoperative mortality was recorded in both groups (Table 3). Overall 7 (13%) patients developed complications after surgery, 2 in group 1 and 5 in group 2. None of them underwent conversion to open during the first procedure. A bile leak occurred in 5 patients, 2 from group 1 and 3 from group 2. A T-tube was not inserted in any of them upon primary surgery. All the 3 patients from group 2 had a stent inserted at previous ERCP, 120, 108, and 42 days before surgery, respectively. The leak occurred at the choledochotomy site in 4 patients and in the CD stump in 1. Three patients underwent ERCP and CBD stenting, including the case of CD stump leak. Two patients had open surgery with resuturing of the choledochotomy; a T-tube was positioned in one case. Two other patients from group 2 developed wound infection and pulmonary embolism, respectively.
Postoperative Data
Values shown in bold are statistically significant.
ERCP, endoscopic retrograde cholangiopancreatography; SD, standard deviation.
A postoperative ERCP was performed in 8 out of 54 (14.8%) patients, 3 in group 1 and 5 in group 2. The indications were failed CBD clearance (4), bile leak (1), failed CBD clearance and bile leak (2), and CBD stent removal (1).
The median hospital stay was longer in group 2 patients (P < .05). Five patients in total, 4 in group 1 and 1 in group 2 were discharged home on the same day of surgery. All of them underwent LCBDE through the transcystic route.
Discussion
Choledocholithiasis represents a common clinical scenario. Treatment options include the sequential endoscopic/surgical approach and the single-stage LCBDE and LC.
The ERCP is widely available and well tolerated by the patients and warrants a high CBD clearance rate, with a 5%–10% complication rate.18–20 A review by Andriulli et al. 21 reported 3.5% post-ERCP pancreatitis (severe in 11.4%), 1.4% cholangitis (severe in 19.8%), 1.3% bleeding (severe in 29.2%), 0.6% duodenal perforation, and 0.3% mortality. Reasons of ERCP failure are the inability to reach the ampulla of Vater, to cannulate the CBD, or the presence of single or multiple impacted stones.22–24 Distortion of the duodenal anatomy like stenosis or previous gastric surgery, reduce the ERCP success rate down to ∼62%.25–27 The presence of a periampullary diverticulum increases the risk of failure to cannulate the CBD. This is mostly described in octogenarians and the ERCP success rate in such circumstances is 78%. Moreover, if the ampulla is located at the bottom of the diverticulum, the success rate is only 38%.28,29 Distal choledochal stenosis, irrespective of the etiology, and Mirizzi's syndrome (both type 1 and 2) are other potential causes of ERCP failure, where CBD cannulation rate can be as low as 8.3%.30,31
Inability to cannulate the CBD and multiple ERCP attempts increase the risk of post-ERCP pancreatitis or duodenal perforation. When ERCP fails, surgery would be advocated.20,32–34
The single-stage treatment of CBDS yields the same success and complication rates as the sequential approach.7,35–53 One of the main advantages of this technique is the treatment of biliary stones during the same hospital admission, thus reducing the costs of hospital stay. However, LCBDE requires specific surgical equipment and the availability of a surgeon with advanced laparoscopic skills.54–58 The last two factors still represent arguments for many surgeons to prefer the sequential approach to the single-stage one.15,16
In the literature, LCBDE after failed ERCP is described as more technically challenging.23,24,59 In the present study, older age and dense fibrosis were described in group 2, where the transcholedochal approach was preferred. These factors probably account for the longer intraoperative time in such patients.
The authors did not find a significant difference in the postoperative complication rate between groups. The study of Karaliotas et al. 23 demonstrated the same results. In our series, a bile leak occurred in 5 patients. Interestingly, all the 3 patients from group 2 who developed a bile leak had a biliary stent inserted upon previous ERCP. It is known that long-term biliary stents stimulate local tissue inflammation and fibrosis, which might increase the risk of postoperative bile leak.
The hospital stay was longer in group 2. Perhaps the longer intraoperative time and the use of the T-tube in 5 patients, requiring time to manage it, may account for such a result. Only patients who had a transcystic CBDE were sent home on the same day of surgery.
Results from the present study show that the single-stage LCBDE and LC after previously failed ERCP, is safe and effective. However, intraoperative time and hospital stay may be longer when compared with patients who had never had an ERCP.
Although the choice to treat CBDS by sequential or single-stage approach depends on the available facilities and skills, 23 careful patient selection is necessary to address the most appropriate treatment.
Its retrospective nature and small population limit the present study; therefore a larger trial would be needed to draw more definitive conclusions. Within these limitations, the authors feel that LCBDE and LC should be considered as the first-line treatment of choledocholithiasis when ERCP failure is anticipated and the risk of post-ERCP complications is higher.
Footnotes
Disclosure Statement
Mr Di Mauro, Mr Ricciardi, Dr Siragusa, and Mr Manzelli have no conflicts of interest or financial ties to disclose.